
Abstract
Background
The effectiveness of the addition of docetaxel and/or zoledronic acid to the standard of care (SOC) for hormone-naive prostate cancer has been evaluated in the STAMPEDE trial. The object of the present analysis was to evaluate the cost-effectiveness of these treatment options in the treatment of advanced hormone-naive prostate cancer in China.
Methods
A cost-effectiveness analysis using a Markov model was carried out from the Chinese societal perspective. The efficacy data were obtained from the STAMPEDE trial and health utilities were derived from previous studies. Transition probabilities were calculated based on the survival in each group. The primary endpoint in the analysis was the incremental cost-effectiveness ratio (ICER), and model uncertainties were explored by 1-way sensitivity analysis and probabilistic sensitivity analysis.
Results
SOC alone generated an effectiveness of 2.65 quality-adjusted life years (QALYs) at a lifetime cost of $20,969.23. At a cost of $25,001.34, SOC plus zoledronic acid was associated with 2.69 QALYs, resulting in an ICER of $100,802.75/QALY compared with SOC alone. SOC plus docetaxel gained an effectiveness of 2.85 QALYs at a cost of $28,764.66, while the effectiveness and cost data in the SOC plus zoledronic acid/docetaxel group were 2.78 QALYs and $32,640.95.
Conclusions
Based on the results of the analysis, SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel are unlikely to be cost-effective options in patients with advanced hormone-naive prostate cancer compared with SOC alone.
Introduction
Prostate cancer is the second most common malignancy and the sixth leading cause of cancer death in males (1). Most prostate cancer patients are diagnosed with localized disease; however, patients may also be diagnosed with locally advanced or metastatic disease. Currently, the standard first-line treatment for locally advanced or metastatic prostate cancer is androgen deprivation therapy (ADT), which can be accomplished by bilateral orchiectomy or luteinizing hormone-releasing hormone (LHRH) agonists/antagonists (2). The addition of radiotherapy to ADT has also been demonstrated to be effective for locally advanced cases (3-5). Unfortunately, nearly all patients with advanced prostate cancer will become refractory to ADT and their disease will develop into hormone-refractory prostate cancer or castration-resistant prostate cancer (6). A range of treatment options, such as further hormone deprivation, bisphosphonates, cytotoxic chemotherapy and immunotherapy, are regarded as standard systemic therapies in the setting of hormone-refractory prostate cancer (7-10). The efficacy of combined or sequenced regimens in the first-line treatment of advanced prostate cancer, however, has not been demonstrated. Given the better tolerance of hormone-naive patients and the benefit they may gain from more aggressive treatments, it is of great importance to investigate new interventions in the setting of hormone-naive prostate cancer.
The STAMPEDE trial was conducted to assess the efficacy of zoledronic acid, docetaxel and celecoxib in patients starting on hormone therapy for locally advanced or metastatic prostate cancer. The celecoxib arms were closed for lack of sufficient activity in the interim analysis (11). The primary outcomes of the remaining arms including standard of care (SOC), SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel were presented at the 2015 American Society of Clinical Oncology (ASCO) annual meeting, suggesting that SOC plus docetaxel and SOC plus zoledronic acid/docetaxel could improve survival in advanced hormone-naive prostate cancer while SOC plus zoledronic acid produced no improvement on survival compared with SOC alone (12).
Regardless of the achievements of the new regimens, the addition of these drugs to SOC may increase both toxicity and cost. Given the growing demand for health-care services and the limited resources in many countries, a cost-effectiveness analysis focusing on the pharmacoeconomics of these 4 strategies is indispensable. In this study, we aimed to evaluate the cost-effectiveness of the 4 treatment options for patients with locally advanced or metastatic hormone-naive prostate cancer based on the STAMPEDE trial from a Chinese societal perspective.
Patients and Methods
Patients and Treatment
The patients modeled in the study were to reflect the participant population of the STAMPEDE trial. A cohort of patients with newly diagnosed locally advanced or metastatic prostate cancer as well as relapsed prostate cancer after previous treatment with radical surgery and/or radiation therapy was assumed. The other inclusion criteria for the model were: Eastern Cooperative Oncology Group (ECOG) performance status (PS) scores of 0 to 2 and adequate hematological function and liver/renal function. The standard methods of ADT included bilateral orchiectomy, LHRH analogues and LHRH antagonists. Antiandrogens alone were not permissible as hormone therapy for patients in the STAMPEDE trial; however, prophylactic use of antiandrogens in combination with an LHRH agonist to prevent “flare” was recommended. As goserelin and bicalutamide are the most widely used LHRH agonist and antiandrogen drug in China, we assumed goserelin plus bicalutamide as the standard ADT regimen in our analysis. The dosages of zoledronic acid, docetaxel and other drugs were consistent with the STAMPEDE trial. The dosages of the drugs in second-line treatment were based on previous publications (13-18). Furthermore, drug dosage adjustments were also considered in the analysis. To estimate the dosage of chemotherapy agents, we assumed the patients in this analysis weighed 65 kg and had a height of 1.64 m, resulting in a body surface area of 1.72 m2 (19).
Model design and structures
A decision-analytic model was conducted to compare the cost-effectiveness of these 4 treatment options as first-line treatment for newly diagnosed advanced prostate cancer or relapsed prostate cancer after previous regional therapy. The model included 3 distinct health states: (1) failure-free survival (FFS); (2) progressive disease (PD); (3) death. Once progression occurred, second-line treatments or best supportive care would be introduced according to the PS of the patient. The life span modeled in the analysis was 20 years, after which almost all hypothetical patients were expected to be dead. The cycle length in our model was assumed to be 1 month. During each cycle, the state of a patient would change according to the Markov model diagram presented in Figure 1. Transition probabilities between the stages were calculated based on what was described by previous studies and the discount rate in our analysis was set at 3% per year (20).
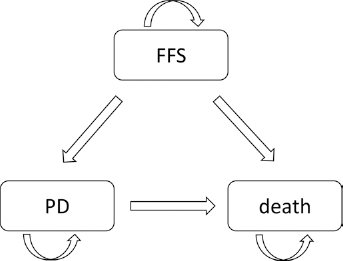
Markov model diagram for the treatment of hormone-naive prostate cancer. A decision-tree model was constructed to investigate the cost-effectiveness of 4 treatment options for hormone-naive prostate cancer. PD = progressive disease; FFS = failure-free survival.
Effectiveness
Restricted mean overall survival (OS) and restricted mean FFS were used in the model as the efficacy data (21). These data were derived from the first results of the STAMPEDE trial. Quality-adjusted life year (QALY), which was calculated by multiplying the life expectancies of each group by the utilities of different health states, was regarded as the gold standard measurement for effectiveness data. Thus, QALY was used to measure the effectiveness in each group in the analysis. Utility value ranges from 0 to 1 and the utility scores for health states in the model were from previously published literature (22).
Cost and resource data
The costs of drugs, surgery, radiotherapy, hospitalization, tests and treatment of grade 3-4 adverse events were included in this analysis. The requirement for hospitalization was modeled to reflect the frequency of drug administration and radiotherapy. The prices of drugs were derived from the national drug prices, while the unit costs of tests, radiotherapy and hospitalization were retrieved from West China Hospital, Sichuan University, China. All costs were converted into US dollars.
Cost-effectiveness
The incremental cost-effectiveness ratio (ICER) between 2 alternative treatment options was used as the primary endpoint in this analysis. The ICER was calculated using the formula: (cost of strategy A - cost of strategy B)/(effectiveness of strategy A - effectiveness of strategy B). The WHO had indicated that incremental cost was acceptable when the ICER was less than the 3 x GDP ceiling ratio (23). Thus, the willingness-to-pay (WTP) threshold was set at 3 times the per capita GDP of China ($20,301.00/QALY) in the analysis. TreeAge Pro 2011 (TreeAge) and SPSS Statistics (IBM) were used for model creation and data analysis.
Sensitivity analysis
To evaluate the impact of essential variables on the robustness of the analysis, we performed 1-way sensitivity analyses by varying the essential parameters within a range of ±30%, the results of which were expressed as tornado diagrams. Probabilistic sensitivity analysis (PSA) was also conducted using a Monte-Carlo simulation of 1,000 iterations. The PSA results were expressed as acceptability curves.
Results
Effectiveness and cost
The survival of each group and the utility values of FFS, PD and death are presented in Table I. Over a 20-year life horizon, the number of QALYs of SOC, SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel were 2.65, 2.69, 2.85 and 2.78, respectively. The economic outcomes of alternative strategies are presented in Table II. The SOC group resulted in an average cost of $20,969.23. Compared with SOC, SOC plus zoledronic acid increased the cost by $4,032.11, while SOC plus docetaxel and SOC plus zoledronic acid/docetaxel increased the cost by $7,795.43 and $11,671.72, respectively.
Survival data for hormone-naive prostate cancer in different groups and utilities for 3 health states

DOC = docetaxel; FFS = failure-free survival; OS = overall survival; PD = progressive disease; SOC = standard of care; ZA = zoledronic acid.
Costs per month and transition probabilities for hormone-naive prostate cancer in different groups
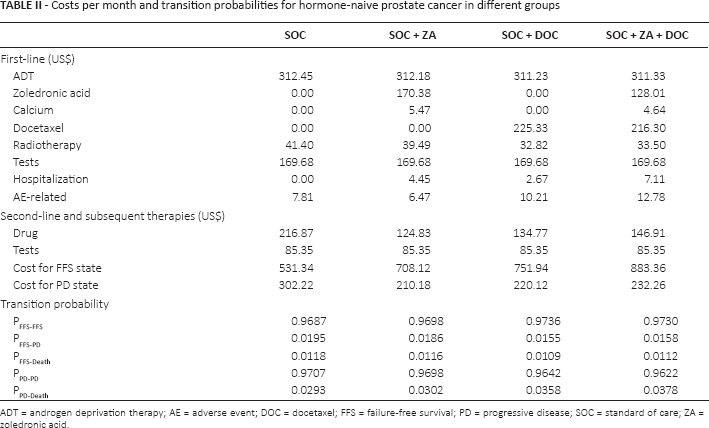
ADT = androgen deprivation therapy; AE = adverse event; DOC = docetaxel; FFS = failure-free survival; PD = progressive disease; SOC = standard of care; ZA = zoledronic acid.
Cost-effectiveness analysis
The ICERs of SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel compared to SOC alone were $100,802.75/QALY, $38,977.15/QALY and $89,782.46/QALY, suggesting that none of these 3 treatment options were cost-effective based on a generally accepted WTP threshold of $20,301.00 when compared with SOC alone (Tab. III).
Results of the cost-effectiveness analysis
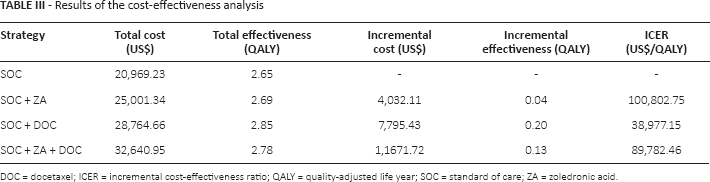
DOC = docetaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life year; SOC = standard of care; ZA = zoledronlc acid.
Sensitivity analysis
One-way sensitivity analyses were used in our model to investigate the impact of variables on the cost-effectiveness analysis. The results of the analyses are shown in tornado diagrams (Fig. 2). The results of the model were mostly influenced by the duration of the failure-free survival (FFS) state, cost of ADT, and utility of FFS state. Other sensitive variables in our model included cost of PD state, cost of tests, cost of docetaxel, cost of radiotherapy, cost of zoledronic acid, and utility of PD state. Variables such as cost of adverse events, cost of calcium, and cost of hospitalization had weak impacts on the robustness of our analysis. Meanwhile, we also conducted a probabilistic sensitivity analysis to confirm the results of the cost-effectiveness analysis based on a Monte-Carlo simulation of 1,000 sampled iterations. The acceptability curve from the probabilistic sensitivity analysis showed that with a WTP threshold of $20,301.00, none of the combined treatments were cost-effective when compared with SOC alone (Fig. 3).
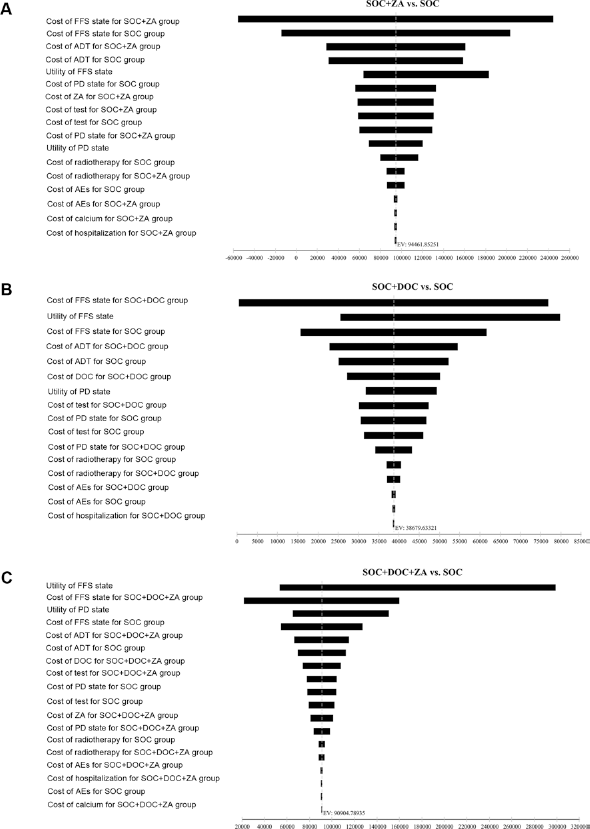
Tornado diagrams of 1-way sensitivity analyses for ICER. Tornado diagrams of univariate analyses for hormone-naive prostate cancer. A) SOC plus zoledronic acid versus SOC alone. B) SOC plus docetaxel versus SOC alone. C) SOC plus zoledronic acid/docetaxel versus SOC alone. These diagrams present the results of 1-way analyses of the parameters for 4 different strategies. The width of the bars represents the range of results of our analysis when the parameters are changed. ADT = androgen deprivation therapy; AEs = adverse events; DOC = docetaxel; PD = progressive disease; FFS = failure-free survival; SOC = standard of care; ZA = zoledronic acid.
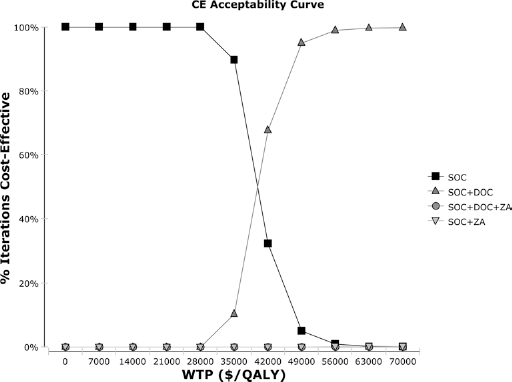
Cost-effectiveness acceptability curves for the 4 first-line strategies in hormone-naive prostate cancer. Cost-effectiveness probabilistic acceptability curves showing the probabilities of acceptability of each strategy for different WTP thresholds. The horizontal axes represent WTP thresholds to gain 1 additional QALY. Four curves are presented: SOC group, SOC plus zoledronic acid group, SOC plus docetaxel group, and SOC plus zoledronic acid/docetaxel group. CE=cost-effectiveness; DOC = docetaxel; QALY = quality-adjusted life year; SOC = standard of care; WTP = willingness to pay; ZA = zoledronic acid.
Discussion
In this study, we developed a cost-effectiveness simulation using a Markov model to evaluate the cost-effectiveness of 4 treatment strategies for men with advanced hormone-naive prostate cancer based on the STAMPEDE trial. The ICER of SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel were $100,802.75/QALY, $38,977.15/QALY, and $89,782.46/QALY, respectively, compared with SOC alone, indicating that SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel are unlikely to be cost-effective compared with SOC alone based on a WTP threshold of $20,301.00/QALY.
Although a significant OS improvement for ADT plus docetaxel versus ADT alone was seen in the STAMPEDE trial, which was consistent with the result of the CHAARTED-E3805 trial (24), the addition of docetaxel to ADT did not show a significant OS benefit versus ADT alone in the GETUG-AFU 15 trial (25). Discrepancies between the GETUG-AFU15 trial and the CHAARTED-E3805 or STAMPEDE trials could be explained by the following hypotheses: first, the CHAARTED-E3805 and STAMPEDE trials included more patients than the GETUG-AFU 15 trial, and the benefit of chemotherapy might be weakened as a result of an insufficient study population; second, in these 3 trials, FFS was significantly improved in the ADT plus docetaxel arm. Thus, unimproved OS might have a correlation with the treatments administered beyond progression. The GETUG-AFU15 trial was launched in 2004 and stopped in 2008, which was earlier than the time of the STAMPEDE trial and the CHAARTED-E3805 trial. In the CHAARTED-E3805 and STAMPEDE trials, new drugs such as abiraterone, enzalutamide, cabazitaxel et cetera were used more frequently in patients in the ADT plus docetaxel arm beyond progression than patients in the ADT alone arm, which may have improved OS in these patients. Meanwhile, 2 recently published meta-analyses (26, 27) also showed a significant OS benefit from concomitant administration of docetaxel and ADT in patients with metastatic hormone-sensitive prostate cancer. Based on the results of these studies, we believe the combination of chemotherapy and hormonal treatment to be an effective treatment option for metastatic hormone-sensitive prostate cancer.
Health expenditures are a major issue for many countries, especially those with limited health-care resources (28). Despite the improvements in survival achieved with the new regimens, our study suggested that the addition of docetaxel and/or zoledronic acid to SOC is unlikely to be cost-effective compared with SOC alone. Zheng et al (29) also performed a Markov model to investigate the cost-effectiveness of ADT plus docetaxel compared with ADT alone based on the E3805 study. The ICER of ADT plus docetaxel versus ADT alone was $26,701.94/QALY, which was lower than that in our study (ICER of SOC plus docetaxel versus SOC alone: $38,977.15/QALY), and the incremental effectiveness in the 2 groups in Zheng's study was higher than that in our study (0.26 QALY versus 0.20 QALY). This might be explained by the survival data in the Zheng et al study being based on the E3805 study. Despite these discrepancies, the results of our study were consistent with those of Zheng et al, suggesting that the addition of docetaxel was not cost-effective compared with ADT alone. However, Zheng et al merely investigated the cost-effectiveness of 2 regimens while our study focused on 4 treatment options, which suggests our findings could be of greater significance.
In the STAMPEDE trial, patients with newly diagnosed local advanced or metastatic prostate cancer as well as relapsed prostate cancer after previous local therapies were all included. Subgroup analyses of the STAMPEDE trial, however, suggested that combined regimens may be more effective in patients with metastatic disease. For example, patients with metastatic prostate cancer treated with SOC plus docetaxel showed a restricted mean OS of 56.1 months, while those treated with SOC alone showed a restricted mean OS of only 49.3 months. SOC plus docetaxel therefore prolonged OS by 6.8 months in patients with metastatic prostate cancer. However, when all patients were considered, the incremental survival of SOC plus docetaxel versus SOC alone was only 4.6 months. The data were similar in the SOC plus zoledronic acid group and SOC plus zoledronic acid/docetaxel group. Based on these results, we suggest that patients with metastatic prostate cancer may gain more significant prolongation of survival when treated with combined regimens. The discrepancy of survival in different subgroups may also have an impact on the results of the cost-effectiveness analysis. The ICER of SOC plus docetaxel versus SOC alone was $38,977.15 in the analysis, which was close to the WTP threshold set in our model ($20,301.00/QALY). As patients with metastatic prostate cancer obtained longer survival, we suggest that SOC plus docetaxel may be more cost-effective for these patients.
It is important to mention that our model had several limitations. First, we conducted our cost-effectiveness analysis based on the efficacy data of the STAMPEDE trial. The patients in this trial were from the United Kingdom and Switzerland, which may impair the application of our results. Similar clinical trials based on Asian-Pacific populations are needed. Second, we took goserelin plus bicalutamide as the standard ADT regimen in our analysis because they were the most widely used LHRH agonist and antiandrogen in China. Given the limited usage of other regimens in China, our assumption seemed to be reasonable; on the other hand, the utility data for each health state were obtained from previously published studies based on patients in other countries, which may not reflect the situation in China and may also decrease the robustness of the analysis.
Conclusions
The results of our analysis showed that SOC plus zoledronic acid, SOC plus docetaxel, and SOC plus zoledronic acid/docetaxel are unlikely to be cost-effective treatment regimens compared with SOC alone in China. Our analysis calls into question the widespread use of aggressive treatment strategies for men with advanced hormone-naive prostate cancer. This analysis provides cost-effectiveness evidence for the use of combined treatments in patients with advanced hormone-naive prostate cancer other than the efficacy data provided by clinical trials. Our results may also make for better decision-making on the part of governments and health-care financial structures.
Abbreviations
androgen deprivation therapy
Eastern Cooperative Oncology Group
failure-free survival
gross domestic product
incremental cost-effectiveness ratio
luteinizing hormone-releasing hormone
overall survival
progressive disease
performance status
probabilistic sensitivity analysis
quality-adjusted life year
standard of care
willingness to pay
Footnotes
Acknowledgment
The authors gratefully acknowledge the anonymous referees for their valuable suggestions.
Financial support: None.
Conflict of interest: The authors declare that they have no conflict of interest.