
Abstract
Background:
Pleural effusion is one of the complications of human non-small cell lung cancer (NSCLC). High mobility group box-1 protein (HMGB1) correlates highly with invasion and metastasis in multiple tumors. The aim of this study was to explore the clinical value of HMGB1 in NSCLC patients, and to investigate the role of HMGB1 in the development of pleural effusion. In addition, we also investigated the regulatory role of HMGB1 in the sensitivity of NSCLC cells to cisplatin.
Methods:
46 NSCLC malignant pleural effusion (MPE) and 31 benign pleural effusion samples were quantitatively analyzed with Enzyme-Linked Immunosorbent Assay (ELISA) for cytokines, such as IL-1beta, IL-6, IL-8 and HMGB1. The HMGB1 expression in NSCLC tissues was examined with RT-qPCR and western blotting methods. Then the influence by HMGB1 on the chemosensitivity of lung cancer A549 cells was examined with MTT assay and colony forming assay for the A549 cells post the treatment with cisplatin or (and) HMGB1.
Results:
The results demonstrated that HMGB1 was up-regulated in the pleural effusion of NSCLC patients, along with the up-regulated levels of proinflammatory cytokines such as IL-6 and IL-8. And the up-regulation of HMGB1 was confirmed at both the mRNA and protein levels in the NSCLC tissues. Recombinant HMGB1 reduced the sensitivity of A549 cells to cisplatin in vitro.
Conclusions:
In conclusion, HMGB1 was up-regulated in the pleural effusion and tumor tissues of NSCLC patients. HMGB1 reduced the sensitivity of NSCLC A549 cells to cisplatin in vitro.
Keywords
Introduction
Lung cancer has been traditionally classified into 2 principal groups: small cell lung cancer and non-small cell lung cancer (NSCLC); the latter type is responsible for 85%-90% of lung cancer diagnoses (1). NSCLC can be divided into adenocarcinoma (ADC) and squamous cell carcinoma (SCC) based on histological types. In spite of multiple treatments such as surgery, chemotherapy, radiation and targeted therapies, the overall 5-year survival rate for NSCLC is only 18.2% (2). The high mortality rate of NSCLC is partially due to its resistance to chemotherapy (3).
High mobility group box-1 protein (HMGB1) is a 30-kDa structural transcription factor that contains 3 domains: 2 positively charged DNA-binding motifs (box A [residue 9-79] and B [residue 95-163]) and a C-terminal acidic tail (residue 186-215) (4, 5). Box B can cause inflammation and be antagonized by box A; the C-terminal acidic tail is believed to interact with boxes A and B and protect them from the nucleus during emigration (6-8). HMGB1 correlates highly with invasion and metastasis in multiple tumors (9, 10). It was reported that HMGB1 enhances tumor exogenous by improving the production ratio of matrix metalloproteinase-9 (MMP9) and optimizing MMP9 gene activity (11, 12).
Most studies have examined the relationship between HMGB1 expression and survival in patients with NSCLC, as well as the diagnostic and prognostic value of HMGB1. However, the relationship between the chemosensitivity of NSCLC and HMGB1 has not yet been explored. In this study, we investigated HMGB1 expression in NSCLC tissues and its accumulation in pleural effusion; then we determined the regulatory role of HMGB1 in the proliferation of NSCLC cells. Our research recognizes the deregulated HMGB1 expression in NSCLC tissues or in pleural effusions and suggests that HMGB1 might be a molecular target for developing novel chemotherapy methods against chemoresistant NSCLCs.
Materials and methods
Patients and specimens
A total of 46 NSCLC patients were involved in this study, with informed consent from each participant. None of these patients had received chemotherapy or radiotherapy before the collection of pleural effusion samples and lung tissue samples. There were 46 malignant pleural effusion (MPE) samples for quantitative analysis of cytokines, and 32 tissue biopsy samples were collected by surgery from 32 of the 46 above-mentioned NSCLC patients for the quantitative real-time polymerase chain reaction (PCR) analysis and Western blotting analysis of HMGB1. The para-cancer tissue in each NSCLC patient (N = 32) was taken as control.
In a control group, 31 benign pleural effusion (BPE) samples were collected from 12 alcoholic cirrhosis patients and 19 chronic cardiac insufficiency patients (without any malignancy). MPE and BPE samples and the tissue biopsy samples were rapidly frozen in liquid nitrogen and stored at -80°C post collection. Ethical approval was obtained from the hospital, and fully informed consent was given by all patients before sample collection.
Enzyme-Linked Immunosorbent Assay(ELISA)
The protein levels of IL-1β, IL-6, IL-8 and HMGB1 in pleural effusion were examined with the ELISA kit for each cytokine (Excellbio, Shanghai, China) according to the kit’s manual. 100 μL serially-diluted standard samples or pleural effusion samples were added in the microplate and was incubated at 37°C for one hours. Then 100 μL antibody against IL-1β, IL-6, IL-8 or HMGB1 was added in each well in the plate, which then was incubated 37°C for 45 minutes. Afterwards, 100 μL secondary antibody conjugated with horseradish peroxidase was added in the plate, which was incubated for 30 minutes at 37°C. Four time-washing of the plate with 100 μl phosphate buffered saline with Tween 20 (PBST) in each well was performed post the supernatant removal before each inoculation. Finally, the inoculation with 100 μL substrate at dark for 15 minutes was performed, and the specific binding optical density of each well was determined immediately at 450 nm with a spectrophotometer (Bio-Rad, Hercules, CA, USA).
Cell culture
The parental lung cancer A549 cell line was purchased from ATCC (American Type Culture Collection, Rockville, MD, USA). All cell lines were cultured in Dulbecco’s modified Eagle’s medium (DMEM) containing 10% fetal bovine serum (FBS; Gibco, USA) in humidified air with 5% CO2 at 37°C. Recombinant HMGB1 (Sigma-Aldrich, USA) was dissolved in DMEM and stored at -80°C before use. For cisplatin or HMGB1 treatment, A549 cells with approximate 85% confluence were updated with DMEM supplemented with 2% FBS, and were treated with 0, 2 or 4 mM cisplatin and/or with 0, 25 or 50 ng/mL HMGB1 for 0, 24 or 48 hours.
MTT assay
A549 cells (2 × 103) in the log growth phase were seeded in a 96-well plate. After overnight growth, the cells were treated with different doses of cisplatin or/and HMGB1 and incubated. Methylthiazolyl-diphenyltetrazolium bromide (MTT; 20 μL) to a final concentration of 5 mg/mL was added, and the cells were incubated for 4 hours at 37°C. Then the supernatant was carefully removed, and 200 μL of dimethyl sulfoxide (DMSO) was added to each well and mixed. The plate was put into a 37°C incubator to dissolve air bubbles, and the OD570 value of each well was measured at the 570-nm wavelength using a microplate reader (Thermo scientific, USA). The results were calculated as ([A570 of control wells] − [A570 of treated wells])/([A570 of control wells] − [A570 of blank wells]) × 100%.
Quantitative real-time PCR assay
Total cellular RNA was isolated using Trizol reagent (Life Tech, USA) according to the manufacturer’s instructions. Approximately 100 ng of total RNA was converted to cDNA using a First Strand cDNA Synthesis Kit (Life Tech, USA). Quantitative real-time PCR was then conducted using SYBR® Green Mastermix (Life Tech, USA) in a 7500 Fast PCR instrument (Applied Biosystems, USA) (13). Then quantitative PCR was performed using the corresponding primers for HMGB1 (14). The cycle threshold (Ct) values of the target gene were normalized to β-actin from the same sample as relative mRNA levels. All samples were run in triplicate in the 96-well reaction plates.
Western blot analysis
Human NSCLC tissues were collected after obtaining informed consent from the patients, and were lysed with lysis buffer (Invitrogen, USA) on ice for 20 minutes. The cell lysates were centrifuged at 15,000 g at 4°C for 30 minutes. The supernatant was collected as the total cellular protein extract. Protein concentration was determined using a BCA Protein Assay Kit (Kangwei Shiji Co., Beijing, China). The samples of total cellular protein were loaded onto 10% sodium dodecyl sulfate–polyacrylamide gel. The separated proteins were electrophoretically transferred to polyvinylidene difluoride (PVDF) membranes (Bio-Rad, USA). The membrane was blocked overnight in blocking buffer containing PBST and 5% non-fatty milk. Then the membrane was incubated with primary antibody against HMGB1 (Santa Cruz Biotechnology) separately for 1 hour and washed with PBST 4 times subsequently. Following incubation with the secondary horseradish peroxidase (HRP)-conjugated antibody for 1 hour, the PVDF membrane was washed 4 times, treated with ECL reagent and exposed on X-ray film. Each band was quantified using National Institutes of Health Image software.
Colony formation assay
Colony formation assay was performed as previously described (15). Briefly, for the colony formation assay, a total of 5 × 102 A549 cells were placed in a fresh 6-well plate and maintained in media containing 10% FBS. Then cells were treated with 50 ng/mL of HMGB1 and/or 4 mM of cisplatin. At 72 hours posttreatment, cells were fixed with methanol and stained with 0.1% crystal violet (Sigma, USA). Visible colonies were manually counted. Triplicate wells were measured in each treatment group.
Statistical analysis
Student’s t-test was used to test the significance between 2 groups, 1-way ANOVA was used to evaluate the difference between several groups (multiple tests) and a p value less than 0.05 was considered statistically significant. Data analysis was performed using GraphPad Prism 4.0 (GraphPad Software, La Jolla, CA, USA).
Results
HMGB1 was up-regulated in the malignant pleural effusions of NSCLC
We checked the level of proinflammatory cytokines (IL-1β, IL-6, IL-8 and HMGB1) in the pleural effusions from NSCLC patients. Firstly, there was no significant difference in characteristics such as age, sex and smoking habits, between NSCLC patients and controls (Tab. I). There was no significant difference in the IL-1β level in the pleural effusion, between MPE and BPE groups (Fig. 1A). However, the pleural effusion levels of IL-6 and IL-8 were significantly higher in MPE patients (n = 46) than in BPE patients (n = 31) (p<0.05 and p<0.01; Fig. 1B and C). In addition, HMBG1 was also markedly higher in the malignant pleural effusion (n = 46) than in the benign pleural effusion (n = 31) (p<0.01; Fig. 1D). Therefore, HMGB1 was shown to be up-regulated in NSCLC pleural effusion, along with IL-6 and IL-8.
Characteristics of patients with pleural effusions
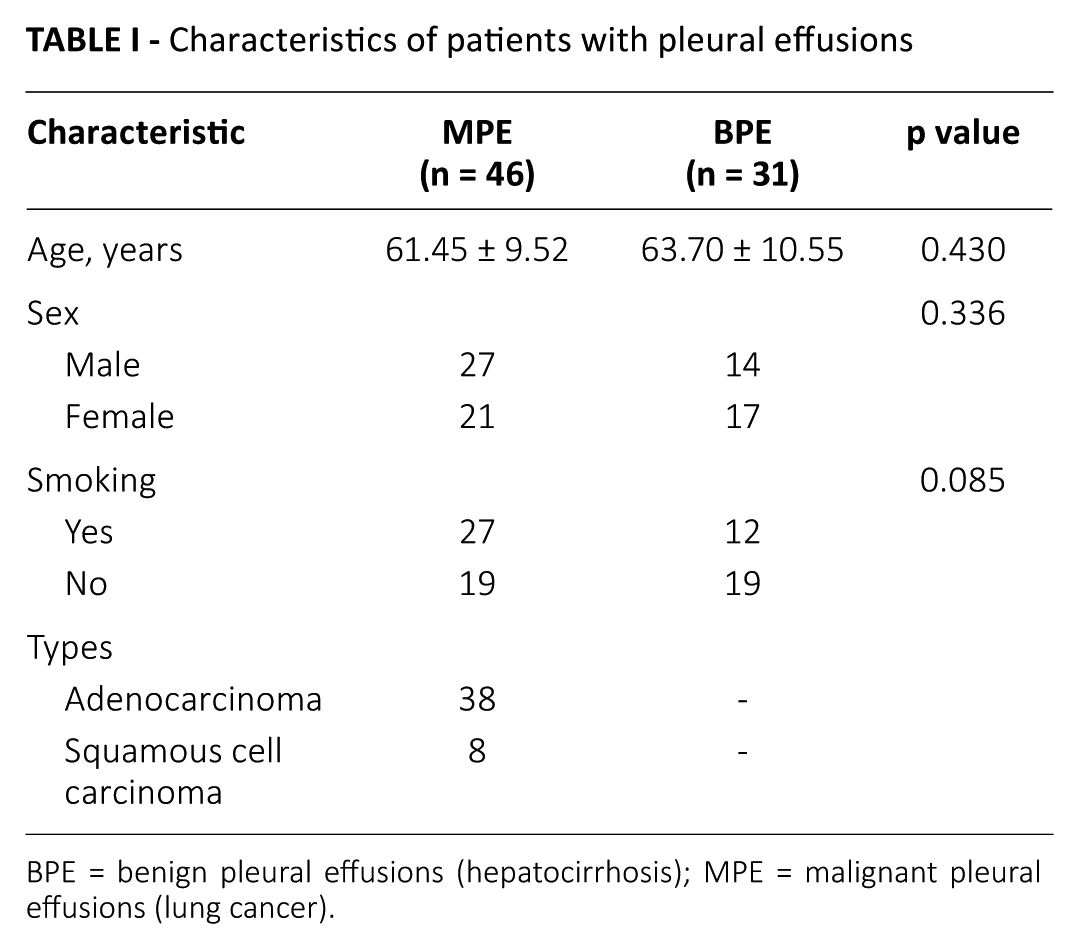
BPE = benign pleural effusions (hepatocirrhosis); MPE = malignant pleural effusions (lung cancer).
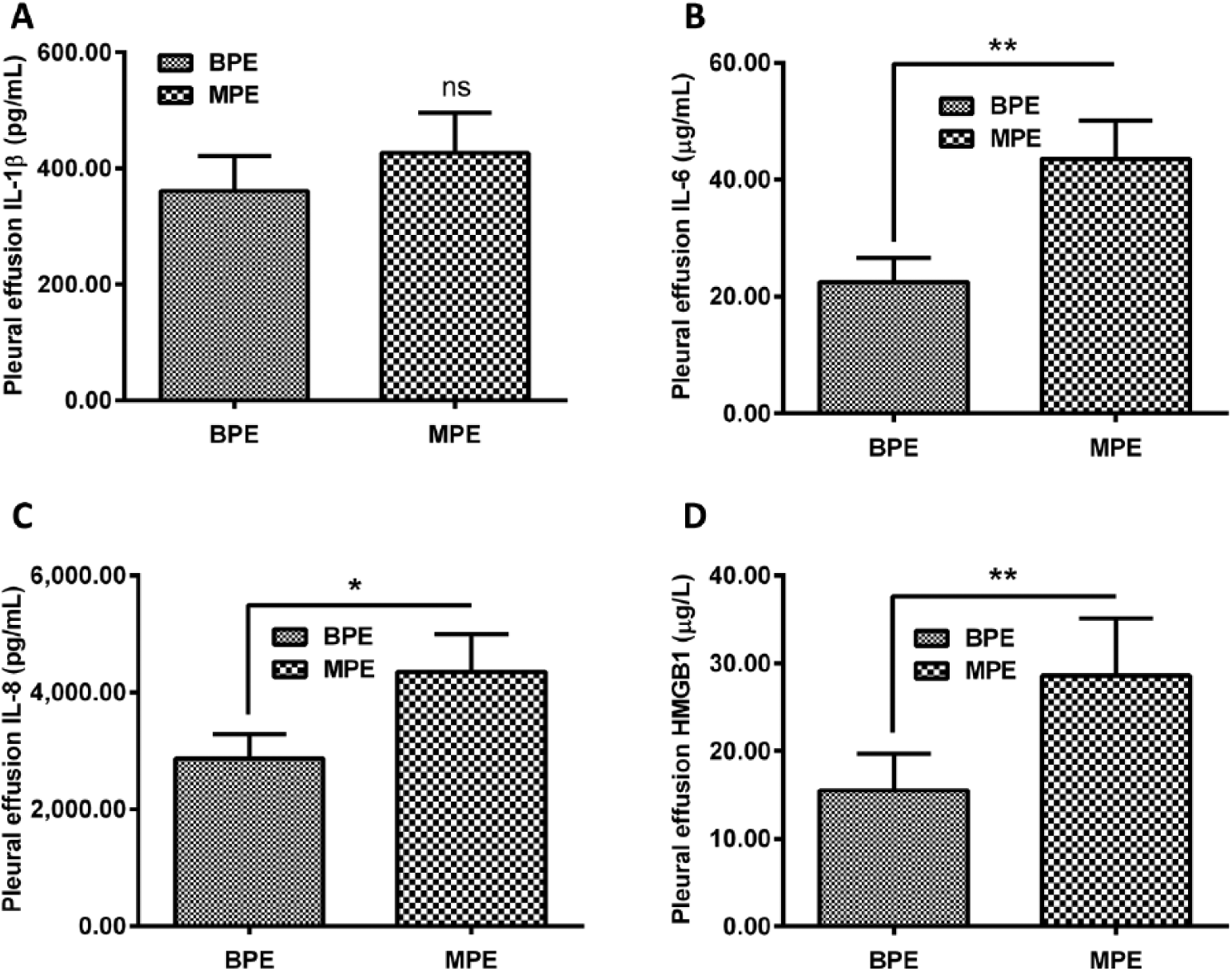
Proinflammatory cytokines in pleural effusions from lung cancer patients. Levels of IL-1β (
Increased HMGB1 expression in human NSCLC tissues
Next, we measured HMGB1 at both the mRNA and protein levels in human NSCLC tissues. As indicated in Figure 2A, the relative HMGB1 mRNA level of NSCLC tissue (n = 32) was up-regulated by 50% when compared with that of peritumor tissues (n = 32), with a statistically significant difference (p<0.0001). The protein levels of the HMGB1 and control groups were also quantified (Fig. 2B and C); in comparison with the control peritumor group (n = 32), the relative HMGB1 (/β-actin) level was up-regulated by 2 times in the NSCLC tissues (n = 32), with a statistically significant difference (p<0.0001). In addition, we examined whether there was an association of the pleural HMGB1 level with characteristics such as age, sex and smoking habits in the NSCLC patients. Our results demonstrated that there was no such association between the pleural HMGB1 levels and any of the above-mentioned characteristic in the NSCLC group (Tab. II). Taken together, the results showed that HMGB1 was up-regulated in both NSCLC tissues and NSCLC pleural effusion.
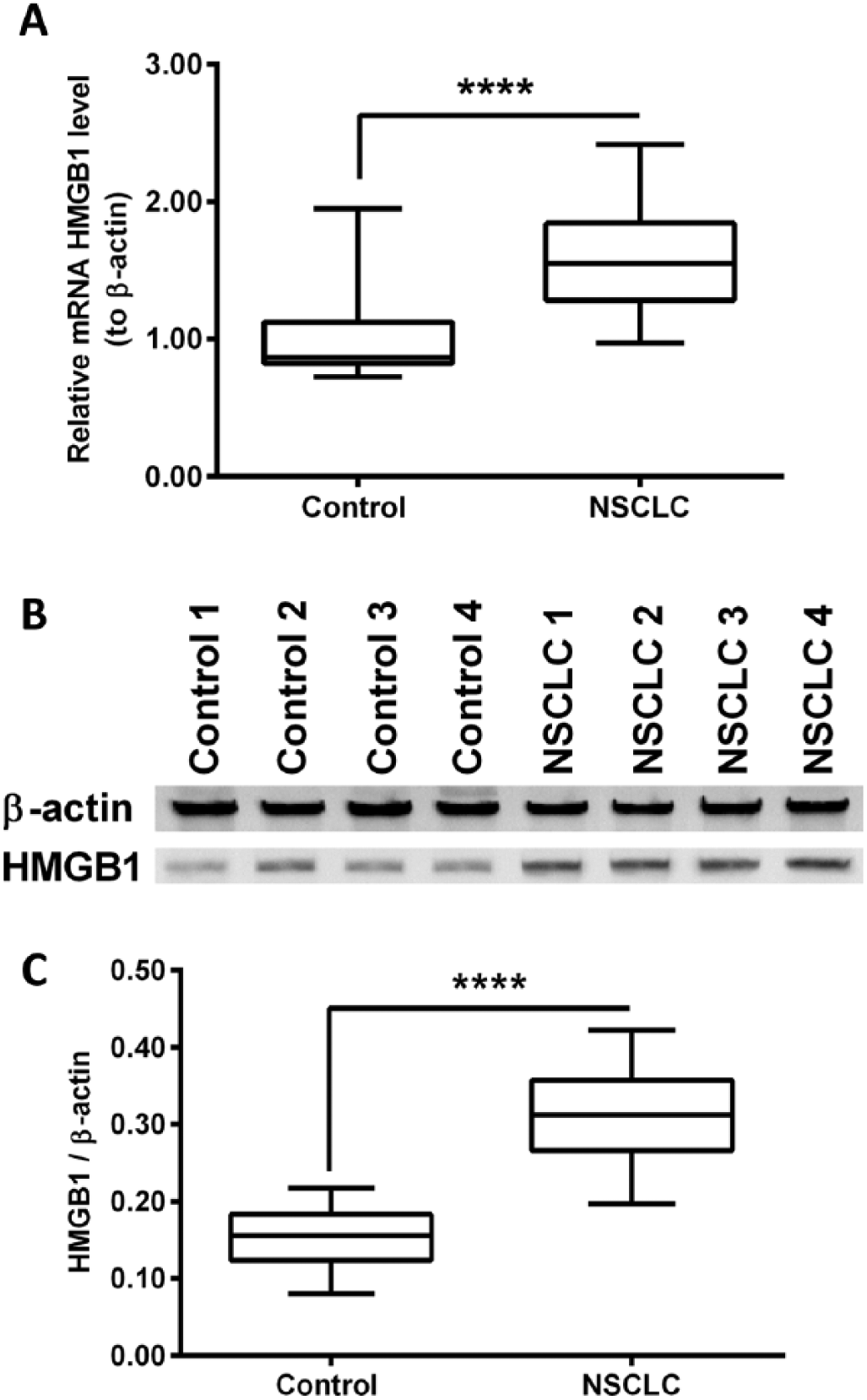
Increased high mobility group box-1 protein (HMGB1) at both mRNA and protein levels in human non-small cell lung cancer (NSCLC) tissues. (
Correlation of MPE HMGB1 with characteristics of lung cancer patients
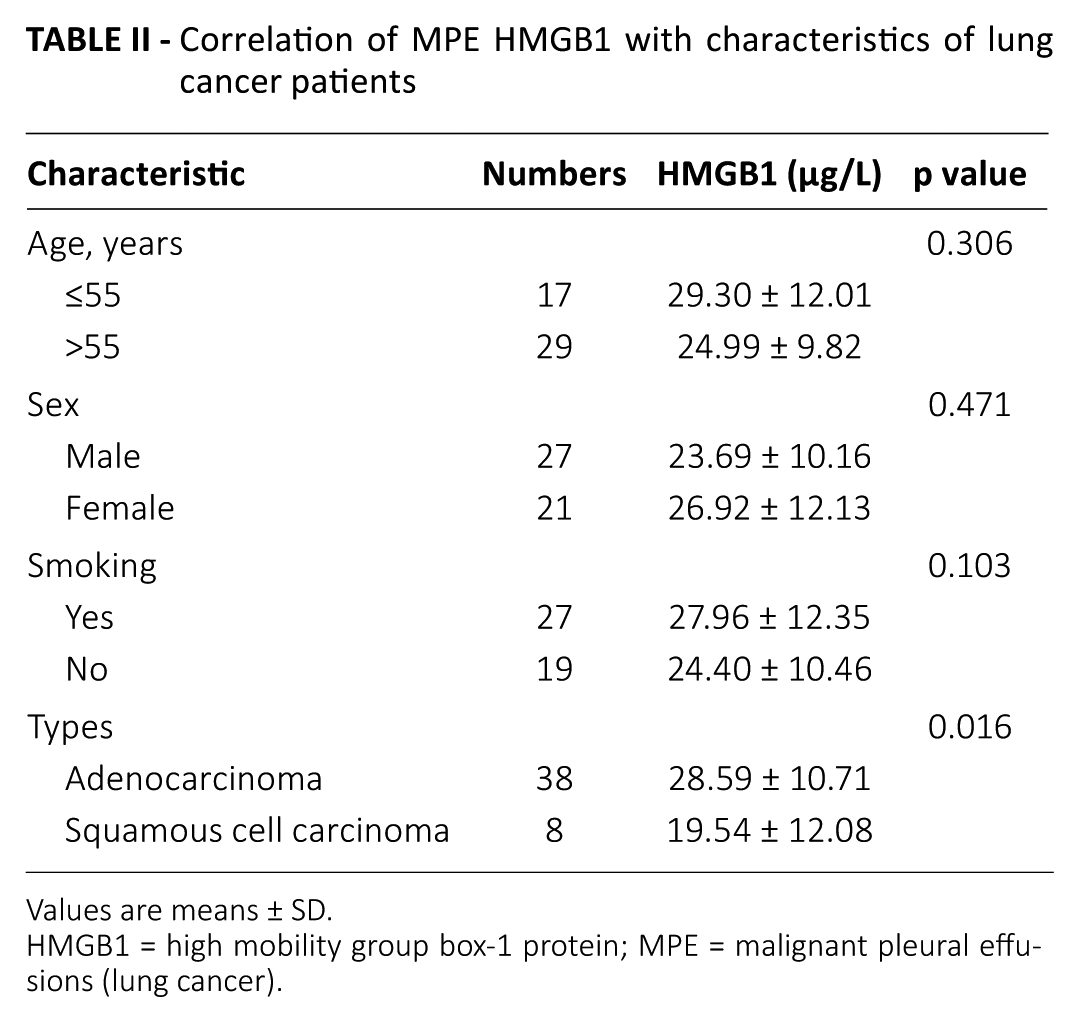
Values are means ± SD.
HMGB1 = high mobility group box-1 protein; MPE = malignant pleural effusions (lung cancer).
HMGB1 reduced the sensitivity of NSCLC to cisplatin in vitro
To explore the influence of HMGB1 on the chemosensitivity of lung cancer cells to cisplatin, the lung cancer A549 cells were treated with different dosages of HMGB1 and/or cisplatin. Then cellular viability was measured at different time points. As indicated in Figure 3A, no statistical difference was found between groups treated by different concentrations of HMGB1 (0, 25 or 50 ng/mL) at 24 or 48 hours. As for cisplatin, cisplatin treatment clearly suppressed cellular viability at 24 and 48 hours post treatment with statistically significant differences, whether at 2 or 4 mM (p<0.05, p<0.01 or p<0.001; Fig. 3B). A cisplatin dose-dependent decrease of cellular viability was also observed.
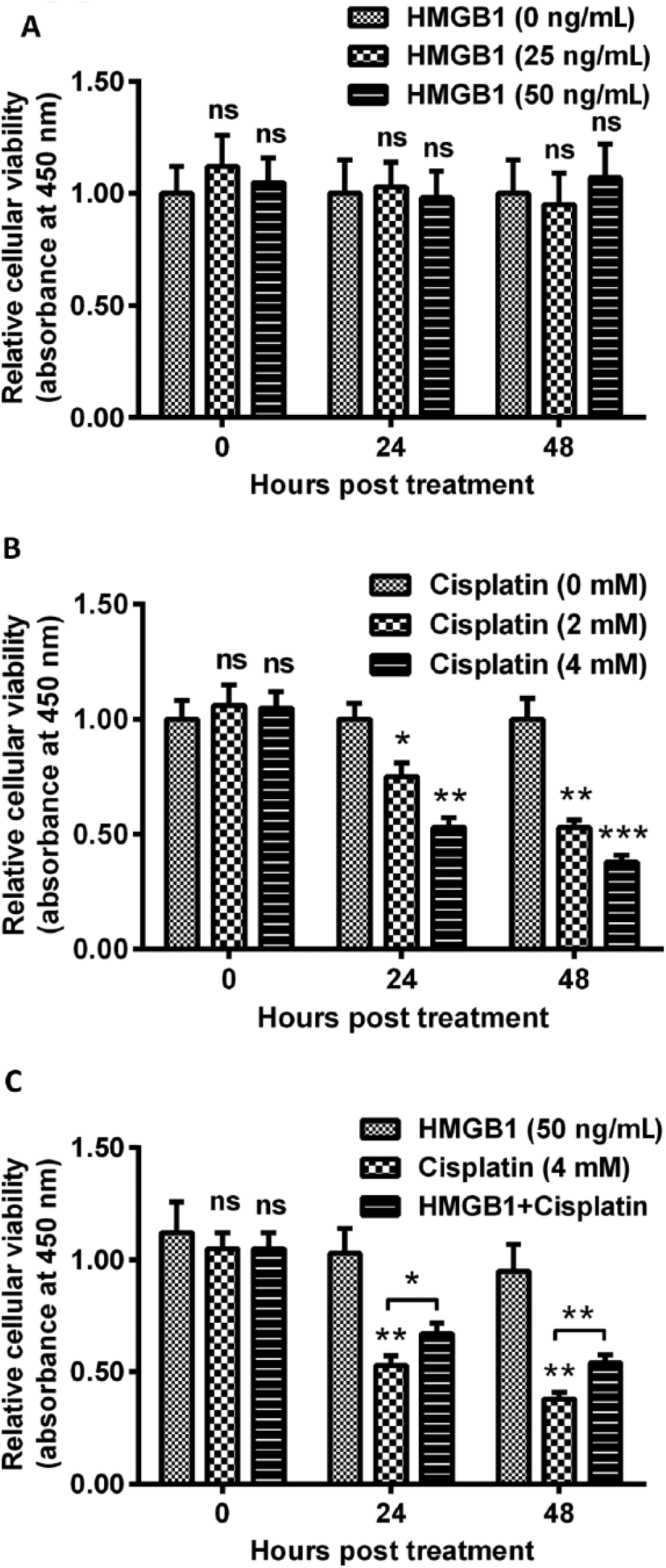
Cellular viability of lung cancer A549 cells which were subject to high mobility group box-1 protein (HMGB1) and/or cisplatin treatment. (
In the next step, we checked the effect of HMGB1 treatment combined with cisplatin on the viability of lung cancer cells. As shown in Figure 3C, cisplatin treatment (4 mM) alone decreased cellular viabilities by 45% at 24 hours (p<0.01), and by 60% at 48 hours (p<0.01) post treatment. The interesting thing was that the cisplatin-mediated viability reduction was ameliorated by HMGB1; cellular viabilities were up-regulated by 50 ng/mL HMGB1 by 25% and 42% at 24 and 48 hours, respectively, when compared with cisplatin treatment alone (p<0.05; Fig. 3C).
Similar results were also observed in the colony formation test. Figure 4A indicates that HMGB1 imposed no regulation on colony forming, both for number and size. However, markedly reduced colonies were formed by A549 cells post cisplatin treatment (4 mM) (p<0.01; Fig. 4A and B). HMGB1 at a dose of 50 ng/mL significantly inhibited the cisplatin-medicated reduction (p<0.05; Fig. 4A and B). In addition, cisplatin (4 mM) efficiently down-regulated the colony size compared with the control (p<0.001; Fig. 4A and C). However, the additional treatment with HMGB1 (50 ng/mL) inhibited the cisplatin-mediated (4 mM) reduction of colony size (p<0.001; Fig. 4A and C). HMGB1 treatment (50 ng/mL) alone did not regulate the colony size (p>0.05). These results indicated that HMGB1 reduced the sensitivity of A549 cells to cisplatin in vitro.
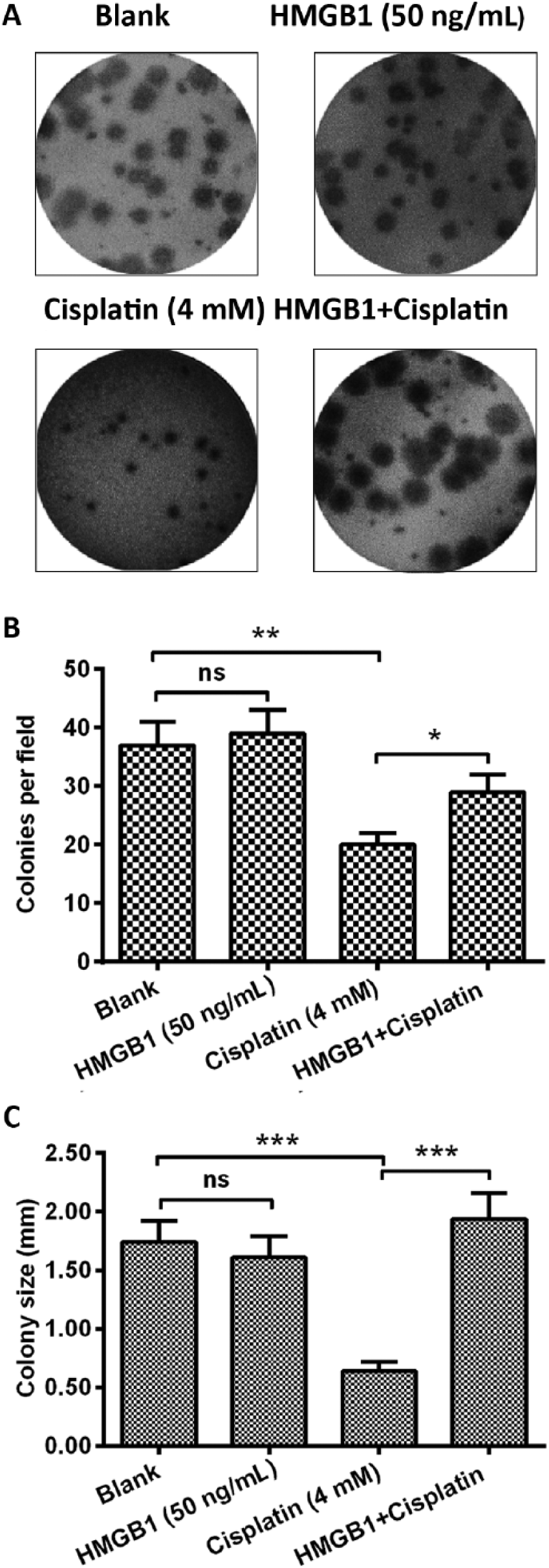
Colony forming of A549 cells which were subject to high mobility group box-1 protein (HMGB1) and/or cisplatin treatment. (
Discussion
HMGB1 has recently been reported to be overexpressed in the tissues or serum of patients with NSCLC, in several studies (16-18). However, some results remain inconsistent. Our results also confirmed the up-regulation of HMGB1 at both mRNA and protein levels in lung tissues of NSCLC patients. Particularly, we first found that HMGB1 was up-regulated in the pleural effusion of NSCLC patients, along with up-regulated levels of proinflammatory cytokines. The pathogenesis of the HMGB1 in NSCLC is unfolding. It has been suggested that HMGB1 activates integrin αvβ3/FAK through the TLR4/NF-κB signaling pathway, and thus enhances tumor cell migration ability (19). HMGB1 also affects the prognosis and development of lung adenocarcinoma, via regulation of the mitogen-activated protein kinases (MAPK) (20), apoptosis and the cell cycle signaling pathway (21, 22). However, little is known about the therapeutic potential of HMGB1 in NSCLC.
Cisplatin (DDP)-based chemotherapy is the first-line therapy for lung cancer (23), yet its efficacy is often limited by the existence or development of chemoresistance (3, 24). Our results indicated that HMGB1 had an inhibitory effect on the sensitivity of NSCLC A549 cells to cisplatin in vitro. In other words, any cisplatin-mediated viability reduction was ameliorated, by HMGB1. Similar results were also observed in the colony formation test. HMGB1 markedly ameliorated, the cisplatin-mediated colony forming of A549 cells in both number and size. These results indicated that HMGB1 reduced the sensitivity of A549 cells to cisplatin in vitro. However, it is not clear what kind of molecular mechanisms are involved in the inhibition of the chemosensitivity of A549 cells to cisplatin. The mechanism behind the phenomenon needs to be further investigated.
Conclusion
In conclusion, HMGB1 expression was found to be up-regulated in both pleural effusion and tumor tissues of NSCLC patients. HMGB1 reduced the sensitivity of NSCLC cells to cisplatin in vitro. Our research also suggests HMGB1 might be a molecular target for developing novel chemotherapy methods against chemoresistant NSCLCs.
Footnotes
Disclosures
Financial support: No financial support was received for this study.
Conflict of interest: No conflict of interests are declared regarding the publication of this article.