
Abstract
Background
Transurethral intracorporeal lithotripsy is the modality of choice for the endoscopic disintegration of large, long-standing, radiolucent or high-density stones. Despite several advantages and proven benefits of contact ureterolithotripsy/ureterolithoextraction (CULT), the application of irrigation carries significant risks of untoward perioperative events including retrograde stone migration and postoperative pyelonephritis.
Methods
We describe a new technique – endoscopic intracorporeal lithotripsy in the gas (СО2) medium. It is a prospective randomized, single blinded pilot study that included total of (n = 60) patients with urolithiasis who were allocated to either experimental or control group. Out of the total pool of patients, 30 underwent treatment with the new approach (experimental group) and other 30 (control group) had contact ureterolithotripsy in a standard of care 0.9% NaCL medium. We included patients >18 years old, with known symptomatic renal calculi disease who were eligible and scheduled for CULT and free from significant coexisting pathologies of urinary tract.
Results
No retrograde migration of the stone fragments into the kidney was reported in the experimental group [complications rate 0%, confidence interval (CI): 0-11.6%]. In the control group, complications were observed in eight cases (complications rate 26.7%, CI: 14.7-42.3%); retrograde migration was in five patients (16.6%), and acute pyelonephritis/exacerbation of chronic pyelonephritis was seen in three (10%) patients. There was not any acute pyelonephritis in the experimental group. Reliability of frequency differences – p = 0.0023 (χ2).
Conclusions
The novel method of contact ureterolithotripsy is a safe and promising alternative to the conventional contact ureterolithotripsy in a fluid medium in a carefully selected patient population.
Introduction
Urolithiasis accounts for approximately 3% of all the pathologies in population and is also the most prevalent disease of the urinary tract. It is estimated that urolithiasis holds for 34.2% amongst the scope of all urological diagnoses (1). Furthermore, roughly 50% of all the manifestations of urolithiasis are secondary to ureterolithiasis (2).
Open surgical approach was used to serve as a gold standard of treatment of urolithiasis and was predominately utilized until minimally invasive endourologic techniques revolutionized the treatment of renal and ureteral calculi. Most frequent complications of the open surgery include injuries to the adjacent organs (9.8%), haemorrhage (≥500 ml) (9.1%), acute pyelonephritis (13.3%), urine extravasation (1.8%), surgical site infection (2.1%), postsurgical strictures (2.5%). Advances in intracorporeal/extracorporeal modalities lead to improved outcomes, patient satisfaction and contributed to decreased morbidity and mortality that altogether resulted in a rapid reduction of the number of open surgeries performed in the recent years (the up-to-date total proportion of open procedures does not exceed 5%) (3). According to the recommendations of European Association of Urologists, extracorporeal shock wave lithotripsy (ESWL) and contact endoscopic lithotripsy are safe and effective procedures and should be considered methods of choice in the treatment of urolithiasis in eligible patients. Data from several studies revealed ESWL success rate of 65-81%, that is for the calculi less than 1 cm after one session. However, it would exponentially decrease to less than 50% for larger stones (≥1 cm in diameter). Moreover, ESWL success rate also inversely correlates to the duration of calculus deposition and a subsequent degree of inflammatory and proliferative changes and negatively affected by alterations in kidney function (4, 5). Hence, not all stones are amenable to extracorporeal destruction.
Intracorporeal lithotripsy also referred as transurethral contact ureterolithotripsy/ureterolithoextraction (CULT) is deemed appropriate for the treatment of larger, long-standing, radiolucent stones as well as high-density calculi. Despite several advantages of CULT, the following pitfalls of the method are well recognized, and, somewhat, limit its use:
Retrograde migration of the calculus or its remnants into the renal cavity: Migration results from increased stone motility that has to do with the fluid medium properties. It is known to promote passage of the stone into the renal cavity. This may lead to preterm termination of the procedure in seek for alternative manipulations including need for long-term urethral stent placement and further extracorporeal lithotripsy predisposing patient to multiple procedures and thus increasing the risk of morbidity, prolonging hospital stay and increasing overall cost.
Poor visualization is a known limitation of the technique. Irrigation solution usually becomes mixed with blood and debris, thus creating challenges to the operator.
Increased risk of infectious complications including acute pyelonephritis or exacerbation of chronic pyelonephritis in the perioperative period. This may be explained in the light of utilizations of high pressure/flow irrigation during the procedure that leads to calico-venous reflux.
As for our experience, total of 474 extracorporeal ureterolithotripsies have been performed till date at our facility. The most frequent intraoperative complication was retrograde calculi migration to the renal cavity (6.3%) and postoperative infection (2.3%), including acute pyelonephritis or exacerbation of chronic pyelonephritis. The rate of stone migration was higher after procedures were performed in the upper region of the ureter, while lithotripter type had no impact on migration frequency. A well described manoeuvre that is known to decrease the rate of calculus migration is applying pressure on the ureter wall; however, controversial results are reported in the literature. Reduction of fluid flow was also reported to be beneficial. However, despite utilization of these and other techniques, stone migration during CULT is still a challenging problem and remains the most frequent intraoperative complication. Our data generally correlate well with the results reported by other authors (6).
In the current study, we attempted to demonstrate the efficacy and safety of a novel technique – transurethral contact ureterolithotripsy in a gas (СО2) medium – by comparing it to conventionally performed procedure in the fluid medium.
Materials and Methods
Thirty patients in the experimental cohort underwent contact ureterolithotripsy in gas medium at the RI UroNephrology, Sechenov FMSMU in the period from 2013 to 2014. Thirty interventions were performed in the control group wherein patient underwent contact ureterolithotripsy in a conventional fluid medium (0.9% NaCl solution) during the same timeframe. Subjects over 18 years old with symptomatic ureterolithiasis who were eligible for contact lithotripsy were included in the study. Those with radiographic measurements of the calculus that exceeded 1 cm were excluded as well as patients with other known abnormalities of the urinary tract. Twenty-four (40%) patients were females, while 36 (60%) were males. Moreover, we allocated patients to both groups based on anatomical localization of the stones to further eliminate the possibility of confounding bias. So, first 10 patients in each group had a stone lodged in the upper region of the ureter, while next 10 had a stone in the middle region and the last 10 in the lower region, respectively.
All patients enrolled in the study underwent full work up prior to instrumentation, including focused physical exam, pertinent lab testing, ultrasound, KUB, CT and MRI of the urinary tract, endoscopic, urodynamic and morphological studies to confirm the diagnosis and rule out other comorbidities. Pneumatic (Lithoclast-Master) and laser lithotripters were utilized intraoperatively for calculi destruction.
Procedure Description
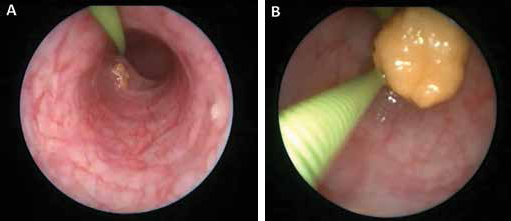
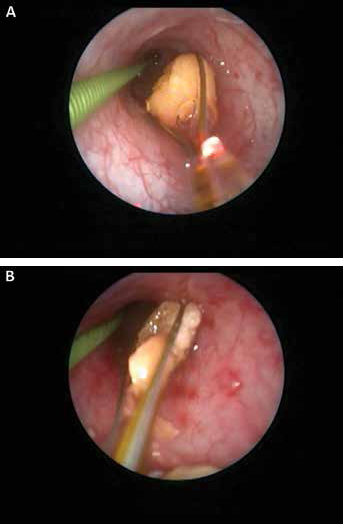
After the informed consent was obtained, standardized patient preparation, anaesthesia, positioning and draping techniques were accomplished in both groups that were compliant with the institutional policies without any deviation from standard of care regulations. Urethrocystoscopy was then performed in the routine fashion. After exploring the bladder, the guidewire was then introduced and advanced into the ureter with simultaneous inflation of the ipsilateral ureter with gas (CO2) until the expanding pressure (13 mmHg) was reached and confirmed on manometry. Ureteroscopy was then performed in a gas (СО2) medium; the probe of the ureteroscope was then advanced until it reached the calculus (Fig. 1A B). Finally, the stone was either directly extracted if possible (Fig. 2) or broken down (Fig. 3A B) with subsequent evacuation of the fragments.
(

Ureterolithoextraction in a gas (СО2) medium.
(
On average, 1.7 1 [confidence interval (CI) -0.5 to 3] of carbon dioxide was required per procedure. The pressure of the CO2 insufflation was 13-16 mmHg that allowed for adequate visibility and good working conditions. This pressure was deemed safe, as similar pressures are routinely used in laparoscopic and other endoscopic surgeries. Moreover, it is 10 times less than fluid pressure that is traditionally used during ureterolithotripsy in a fluid medium. The technique was also patented after the completion of the study (“The Way of Prevention of Calculus Migration to the Kidney during Contact Ureterolithotripsy”).
Collected data included frequency of intraoperative and postoperative complications (retrograde calculus migration to the kidney, acute pyelonephritis or exacerbation of chronic pyelonephritis), quality of operative field visualization and degree of stone motility.
As safety was our outmost priority, all the interventions were performed in compliance with current guidelines for laparoscopic procedures. At this time, there are certain requirements regarding gas properties used for laparoscopic procedures. Carbon dioxide remains the gold standard gas for insufflation of the body cavities. It is colourless, chemically inactive, nonflammable, plasma-soluble, readily available and low-cost substance. In our case, it provided the operator with an unobstructed and clear view of the operative field (7-9). CO2 is water-soluble, hence in the used concentrations and quantities poses a minimal risk of gaseous embolism. Nevertheless, all the necessary precautions were undertaken and anaesthesiology team notified during gas insufflation. Even though the ureter mucous membrane has negligible absorption capacity (10), several blood gas sampling analyses were performed before and after insufflation to rule out absorption of the large quantities of gas into the blood stream potentially causing acute respiratory acidosis. [pH remained within the normal physiologic range (7.35-7.45). Testing was performed in both groups in a similar fashion regardless of the type of ureterolithotripsy]. No other blood gas disturbances were noted. End-tidal CO2 was monitored and remained unchanged in all cases.
Results
No episodes of retrograde calculi migration were documented in the experimental group (complications rate 0%, CI: 0-11.6%). In the control group, complications were observed in eight cases (complications rate 26.7%, CI: 14.7-42.3%); retrograde migration was in five patients (16.6%), acute pyelonephritis/exacerbation of chronic pyelonephritis was seen in three (10%) patients. There was not any acute pyelonephritis in the experimental group (Fig. 4). Reliability of frequency differences – p = 0.0023 (χ2).
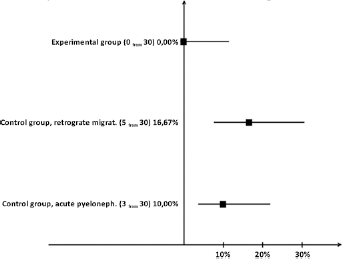
Comparative analysis of CULT complications in control and experimental groups of patients.
In addition, no calculus migration was observed during ureterolithotripsy in a СО2 medium and no significant haemorrhage was reported. Overall, less haemorrhage somewhat facilitates visibility adding to surgeon's satisfaction and precision of the manipulations. Mean irrigation flow was similar in both groups (around 1.7 l).
Discussion
This study is the first to our knowledge to compare results of performing ureteroscopy in the gas medium compared with conventional fluid medium. This is a pilot study and thus further research is required. From our experience, absence of retrograde migration and absence of documented complications provide promising prerequisite for further analysis. These benefits of gaseous medium can be explained in the light of its physical properties. Water density is significantly higher than that of carbon dioxide: 998.2 versus 1.97 kg/m³, respectively. Thus, the driving force of water is likely to accelerate stone migration by increasing its kinetic energy. The latter can be appreciated from the formula: FA = rgV, where r — fluid (gas) density, g — free fall acceleration, and V — immersed object volume. The resultant calculus motility in water is higher than in СО2. Any extrinsic impulse, particularly applied by the lithotripter, can act synergistically with the fluid driving force and further increase the likelihood of the stone migration.
It is also apparent that the object embedded in fluid is lighter, as it is less subjected to gravity forces as opposed to gaseous environment. This is explained by the fact that in water, Archimedes’ buoyant forces oppose the gravity much greater than in gas. Furthermore, in the gas medium, calculus also adheres more firmly to the ureter wall, as the friction forces are increased, which also contribute to decreased motility.
Another aspect of frequent calculus migration in fluid can be explained by physical properties of irrigation fluid and its flow velocity (6): calculus is following the pressure gradient and pushed proximally towards the renal pelvis. NaCl pressure during ureteroscopy may reach 150 cmH2O that is over 110.25 mmHg; On the contrary, if carbon dioxide is used, pressure does not exceed 13-16 mmHg (17.66 cmH2O); although this is enough pressure to dilate the ureter distally to the stone, it remains relatively collapsed proximally to the stone thus creating additional anatomical barrier to stone migration.
According to several studies, normal pressure in upper urinary tract varies from 10 to 15 cmH2O depending on the phase (systolic or diastolic), while in pathologic conditions as seen in the scenario of acute outflow obstruction also known as renal colic, intrapelvic pressure may reach 100 cmH2O (11). Thus, pressure created in the ureter during СО2 insufflation (17.66 cmH2O) is within physiological boundaries and hence does not increase the risk of calico-venous reflux. This hypothesis might rationalize the absence of infectious complications (acute pyelonephritis) in immediate postoperative period.
Conclusion
Results obtained in this pilot study allowed us to arrive at a conclusion that the suggested method is safe and might be superior to conventional contact ureterolithotripsy. The proposed advantages of the method include but not limited to
Absence of retrograde calculus migration into renal cavity due to unique gas properties. The clinical significance includes decreased duration of surgery by two to threefold and the need for repeat and more complicated interventions is less likely to arise.
Improved visualization of the field secondary to better optical properties of the gas. Interestingly, less haemorrhage was subjectively reported by the operating surgeon that further enhanced the operating conditions, thus increasing overall surgeon's satisfaction. The limitations include the fact that the actual blood loss was not directly measured and compared between groups.
Absence of calico-venous reflux due to reduced pressure in the system minimizes the risks of postoperative infectious complications (acute pyelonephritis or exacerbation of chronic pyelonephritis).
Total cost per 1 L of CO2 is approximately 0.003$, while total cost per 1 L of physiologic saline is around 0.8$ (in Russia), which is essential in the environment of supply and cost constraint in healthcare.
Footnotes
Financial support: The authors received no financial support for the research.
Conflicts of interest: The authors declare that there are no conflicts of interest.