
Abstract
Objective
To evaluate the efficacy of Preoperative Aspects and Dimension Used for an Anatomical (PADUA) classification in the prediction of Warm Ischemia Time (WIT) during Laparoscopic Partial Nephrectomy (LPN).
Methods
Single centre retrospective study on 402 patients who underwent LPN between January 2011 and October 2013. WIT was correlated with each characteristics of the PADUA classification. Univariate and multivariate analysis were used to evaluated the independent predictive risk factors of WIT >20 minutes.
Results
The median WIT was 19.8 minutes (IQR 15-25). The PADUA risk groups (High vs Low: OR: 2.804; 95% CI 1.155-6.806; p-value <0.001; Intermediate vs Low: OR 0.971; 95% CI 0.185-5.092 p-value <0.001) and PADUA score as continuous variable (OR: 1.512; 95% CI 1.043-2.194; p-value <0.001) were the best independent risk factors of WIT >20 minutes. Another important factor related with WIT >20 minutes was a CKD stage 3 (p-value: 0.047; OR: 0.528; 95% CI:0.282-0.990).
Conclusions
This study reveal that tumor’ anatomical aspects may influence the WIT. The use of the nephrometry scoring systems should to be use by the surgeon in the planning of nephron sparing surgery (NSS) and should be considered for its inclusion in international guidelines.
Keywords
Introduction
International guidelines on Renal Cell Carcinoma (RCC), states that renal tumors ≤7cm are best managed by nephron sparing surgery (NSS) (1, 2). Open partial nephrectomy (OPN) represents the gold standard for renal tumors ≤7 cm, while laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RAPN) are the main alternatives. Beyond the clinical tumors size, other antomical aspects are routinely evaluated by the surgeon in the planning of conservative therapy. Warm Ischemia Time (WIT) is one of the most important predictive factors of kidney function after partial nephrectomy (PN) and every minutes counts when the renal hilum is clamped (3). Becker et al (4) reported that, in order to preserve the renal function, WIT should not exceed 20 minutes. In a recent metanalysis, Aboumarzouk et al (5) showed that LPN and RAPN have low complications rate, but RAPN was found to have less WIT. In centres with advanced laparoscopic experience, the WIT during LPN is consistently low (6). However, it's not entirely certain how WIT and other adverse intra-operative outcomes can be predicted before PN. Ficarra et al (7) recently proposed a new scoring system based on renal tumor anatomical aspects for patients candidated to NSS. The Preoperative Aspects and Dimensions Used for an Anatomical (PADUA) classification of renal tumors is based on several anatomical features: longitudinal polar location (superior/inferior = 1 pt; Middle = 2 pt), exophytic rate (≥50% = 1 pt; <50 = 2 pt; endophytic = 3 pt), renal rim (lateral = 1 pt; medial = 2 pt), renal sinus (not involved = 1 pt; involved = 2 pt), urinary collecting system (UCS) (not involved = 1 pt; dislocated/infiltrated = 2 pt), tumor size (≤4 = 1 pt; 4.1-7 = 2 pt; >7 = 3 pt) and face (anterior or posterior). After having assigned a score to each of this anatomical aspects we had three risk groups: low (PADUA Score 6-7), intermediate (PADUA Score 8-9) and high (PADUA score >10). This classification differs from the R.E.N.A.L nephrometry scoring system (8) especially for the definition of the sinus lines and the evaluation of the anatomical relationship between the tumor and the UCS. The aim of this study is to assess the efficacy of PADUA score system in the prediction of WIT during LPN.
Methods
This study was approved by the local ethic committee. All patients were counselled about the risks, benefits and alternative treatments for the condition; individual informed consent was obtained. We analyzed, from the medical database, 402 consecutive LPN between January 2010 and October 2013. Patients who undergone RAPN or OPN don't entered in this study. All operations were performed by the same surgeon with high experience in laparoscopic, robotic and open surgery. All surgery was performed with retroperitoneal approach as described in previously reports (9-10) with renal artery clamping. Before surgery, all patients underwent computed tomography (CT) scan or magnetic resonance imaging (MRI) to evaluate the clinical stage and the anatomical characteristics. The WIT and the estimated blood loss (EBL) were assessed by an anesthesiologist. Early postoperative complications, occurred during hospitalization, were classified according to the Dindo modification of the Clavien system (11-12) and defined as minor (grade 1-2) and major (grade 3-4). Based on image of CT scan or MRI, a PADUA score (7) was assigned to each patients by two different examiners. Tumors were stratified into low-risk (score 6-7), intermediate-risk (score 8-9), and high-risk (score ≥10) (7). From the medical database, for each patients were also extracted the following informations: age, BMI, ASA, Charlson comorbidity index (CCI), gender, clinical tumor size, WIT, surgery duration, EBL, conversion to open, intra-operative complications and early postoperative complications. Renal function was calculated by estimating the glomerular filtration rate (GFR) through the Modification of Diet in Renal Disease study (MDRD) (13) formula preoperatively and postoperatively using preoperative and latest postoperative (median 60 days after surgery) serum creatinine (sCr). Renal function was staged according to the National Kidney Foundation Disease Outcome Quality Initiative classification. Pathological tumor size, histological subtypes according with the World Health Organization (WHO) classification (14), tumor extension according with the TNM classification (15), nuclear grade according to the Fuhrman classification (16) and positive surgical margin (PSM) rate were also extracted. PSM were definited as the extension of the tumor over the inked parenchymal surface. Descriptive statistics was performed. Parametric continuous variables were reported as median plus or minus standard deviation; non parametric continuous variables were reported as median and interquartile range (IQR); categorical variables were reported as number of cases (no) and percent (%). Mann-Whitney-U test was used to compare two groups with non parametric continuous variables; Kruskal-Wallis test was used to compare three groups with non parametric continuous variables. Wilcoxon signed rank test was used to assess the differences and upstaging in preoperative and postoperative chronic kidney disease (CKD) stage. Univariable was performed to evaluated factors related with a WIT >20 minutes. Based on the univariable analysis results a binary logistic regression analysis was performed in order to evaluate which factors were independently associated with WIT >20. A two side p value of <0.05 was definited as statistically significant. All data were analyzed using SPSS v. 20 (IBM Corp., Armonk, NY, USA).
Results
Table I reports the preoperative patients characteristics. 402 patients (65.2% male and 34.8% female) with median age of 49.8 years (IQR 42-58) and a median BMI of 25.4 (IQR 22-27) were included in this study. 97% (390 of 402) had an incidental diagnosis of RCC. The median PADUA score was 8 (IQR 7-10) and the median tumor size, based on the best diameters on CT scan or MRI, was 3.02 cm (IQR 2-3.6). The median preoperative sCr and eGFR were 75 µmol/L and 95.4 ml/min per 1.73 m2, respectively. In this patients cohort we report a preoperative CKD stage 1 in 55.5% (223 of 402), stage 2 in 37.8% (152 of 402) and stage 3 6.7% (27 of 402). Table II show intra, postoperative characteristics and pathological results. Median operative time was 112.9 minutes (IQR 90-140). Median WIT was 19.8 minutes (IQR 15-25). Median EBL 65.8 ml (20-67). We reported an intra-operative complications rate of 15.5%. Peritoneum, renal vein and diaphragm injury were the most common complications occured during the intra-operative time, all of them treated with intra-operative repair. According to the Clavien-Dindo classification (11) were evaluated complications occurred during hospitalization. We reported 16.6% of minor grade and 1.5% of major grade. Pathological results showed that 16.3 % (65 of 402) had a benign lesion, 83.7 (337 of 402) an RCC. The Fuhrmarn nuclear grade was avaible only for 304 patients. PSM occurred in 1.8% (7 of 402). The Wilcoxon rank test, described significative difference between pre and postoperative eGFR (95.5 vs 83.5 ml/min per 1.73 m2) and pre and postoperative CKD stage (CKD 1 = 55.5% vs 38.3%; CKD 2 = 37.8% vs 47.5%; CKD 3 = 6.7% vs 14.2%) (p value = <0.001) with a CKD upstaging in 130 patients. Table III described the relationship between anatomical features and PADUA risk groups with WIT. The WIT was significantly lower when the tumor polar location was superior/inferior (p value 0.002), the exophytic rate was ≥50% (p value <0.001), when tumor occured lateral to renal rim (p value <0.001), renal sinus and UCS was not involved (p value <0.001) and the tumor size was ≤4 cm (p value <0.001). No difference between anterior and posterior face was observed (p value 0.306). The low-risk group presented a median WIT of 16 minutes (13-20), intermediate 21.4 minutes (16-27) and high 22.47 minutes (17-28). The univariate analysis (tab. IV) described that all anatomical features and PADUA risk groups were related with a WIT >20 minutes. When every anatomical features change, increase the WIT. We find that a postoperative CKD stage 3 was related with a WIT >20 minutes. Logistic regression analysis (tab. V) described that the PADUA risk groups (High vs Low: Odds Ratio [OR]: 2.804; 95% Confidence Interval [CI]: 1.155-6.806; p value <0.001; Intermediate vs Low: OR 0.971; 95% CI: 0.185-5.092 p value <0.001) and PADUA score as continuous variable (OR: 1.512; 95% CI: 1.043-2.194; p value <0.001) were the best independent predictive risk factors of WIT. Tumor size codificated as categorical variable (>7 vs ≤4: p value 0.334; 4.1-7 vs44: p value 0.791) and tumor size as continuous variable (p value 0.088) were not independent risk factors of WIT. Another important factor related with WIT >20 minutes was a CKD stage 3 (p value: 0.047; OR: 0.528; 95% CI: 0.282-0.990). This aspect confirm in our study that a WIT >20 minutes is related with an increase risk of renal function reduction.
Patients preoperative characteristics
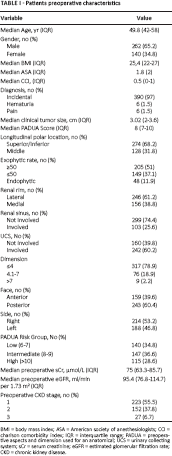
BMI = body mass index; ASA = American society of anesthesiologists; CCI = charlson comorbidity index; IQR = interquartile range; PADUA = preoperative aspects and dimension used for an anatomical; UCS = urinary collecting system; sCr = serum creatinine; eGFR = estimated glomerular filtration rate; CKD = chronic kidney disease.
Patients intra and postoperative characteristics
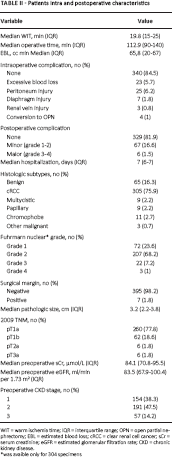
WIT = warm ischemia time; IQR = interquartile range; OPN = open partial nephrectomy; EBL = estimated blood loss; cRCC = clear renal cell cancer; sCr = serum creatinine; eGFR = estimated glomerular filtration rate; CKD = chronic kidney disease.
was avaible only for 304 specimens
Correlation between PADUA anatomical features and WIT
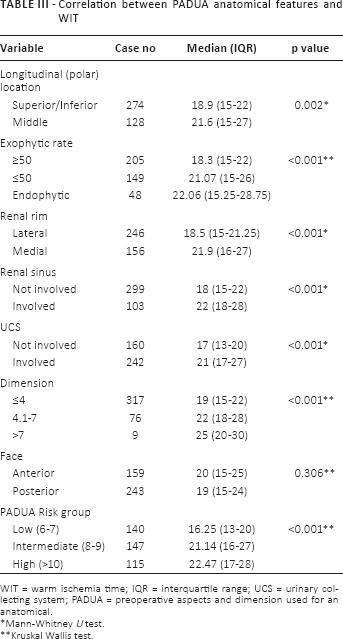
WIT = warm ischemia time; IQR = interquartile range; UCS = urinary collecting system; PADUA = preoperative aspects and dimension used for an anatomical.
Mann-Whitney U test.
Kruskal Wallis test.
Univariate analysis on potential risk factors of WIT >20 minutes
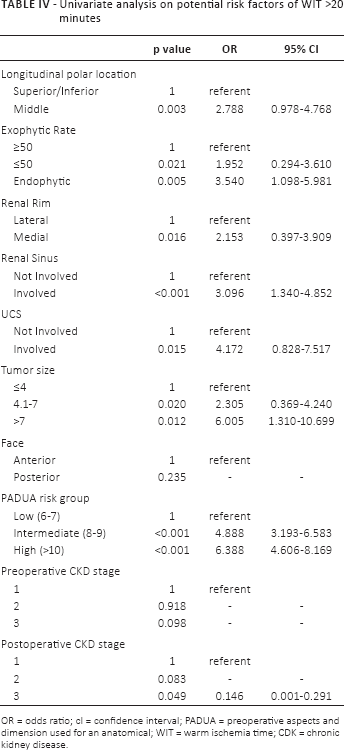
OR = odds ratio; cI = confidence interval; PADUA = preoperative aspects and dimension used for an anatomical; WIT = warm ischemia time; CDK = chronic kidney disease.
Multivariate analysis predicting the risk of WIT >20 minutes
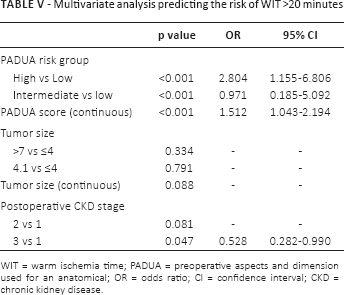
WIT = warm ischemia time; PADUA = preoperative aspects and dimension used for an anatomical; OR = odds ratio; CI = confidence interval; CKD = chronic kidney disease.
Discussion
The findings from this study show that the PADUA classification is a good tool that can help the surgeon in assessing the intraoperative outcomes in LPN. WIT represent the most important factor to evaluate before surgery; only the tumor size cannot estimated it. Routinaly surgeons evualate each anatomical tumor characteristics, but actually the international guidelines (1, 2) reported only tumor size ≤7 cm as cut-off for PN. Evidence efforts that a WIT of 30 minutes is associated with kidney injury (17, 18). Several studies recently demostrated that the optimal cut-off of WIT is 20 minutes (3, 4). In this study we used this end-point to evaluate WIT. In this report the median WIT during LPN was 19.8 minutes with an increase in every aspects of PADUA classification. 65% (260 of 402) had a WIT ≤20 minutes, 30% (118 of 402) between 21-30 minutes and only 5% (24 of 402) a WIT >30 minutes. Porpiglia et al (6) reported that the WIT is consistently higher in LPN comparated with OPN altough it tends to decrease after a long learning curve in high volume centers and Gill et al (19) confirmed this finding. Interestingly, the present study shows how only one change in anatomical features of PADUA classification, can increase WIT. Recently Ficarra et al (20) compared the PADUA classification with WIT and post-opertive complications in RAPN. In that study the surgical experience, the PADUA risk group, the PADUA score system continuosly coded and UCS repair were independed predictive risk factors of WIT. Comparated with our study, we have some limitations. We reported 402 LPN taken by the same surgeon with retroperitoneal approach. To eliminate all the bias that can influence changing in WIT during NSS we selected only laparoscopic procedures performed in a recent period (2010-2013), after a long learning curve (>1000 laparoscopic procedures before the study period), by a single surgeon. This study want to prove that the PADUA score is associated with WIT and to consider only this aspect, from our opinion, should be eliminated all the bias related to technique (OPN, LPN and RAPN) and surgical experience. Obviously, the surgical technique is an important related factor with WIT, specially in the robotic era. A recent meta-analysis (5) showed that RAPN has less WIT than LPN. LPN is a challenging procedure with a long learning curve and is not the real referent for RAPN (21). However LPN is not expansive and it can considered the real competitor of RAPN in highly skilled laparoscopic centers. A recent study (22) showed that there was no significant difference in terms of WIT between RAPN and LPN in complex tumours (median renal score 8). A likely explanation for this findings might rely in the high experience in laparoscopic and robotic surgery in high volume centres; as reported by the authors (22) LPN did not show longer WIT than RAPN if it is performed in centres with laparoscopic experience. In high volume centres, is not the surgical approach (RAPN or LPN) the main factor influencing the WIT, but the complexity of the tumour. Our results on WIT efforts this theory. If we do not considerate the technique and the surgical experience, our study reported similar results to Ficarra et al (20) study. Our report reinforced the validity of PADUA score system in the prediction of WIT. In the current study, we did not reported the time for UCS repair. We use, routinaly, for each kind of tumor, two or three running suture (3-0 Vicryl CT needle; 2-0 Vicryl RB needle, Ethicon, Cincinnati, OH, USA) secured with medium Weck Hem-o-lok clip (Teleflex Medical, Research Triangle Park, NC, USA) and in our opinion the suture time is correlated with the preoperative tumor's characteristic. Based on the letast eGFR (median follow-up 60 days), we found that WIT was related with a CDK stage 3. As reported by literature (3, 4, 18) WIT is an important predictor of kidney function after PN. In a large laparoscopic series (19) Gill demostrated that patients with a WIT <20 minutes had less decrease of postoperative eGFR comparated with patients with WIT >20 minutes. Our study support this finding. An increase risk of CDK stage 3 is related with WIT >20 minutes. The short follow-up for evaluating kidney function (median 60 days) assessed only by eGFR present some limitations. MDRD equation has limitations for eGFR evaluation. sCr is the best predictor of eGFR in MDRD equation, but his levels are impacted by BMI, gender, ethnicity, age and hydratation status. No patients present a pre or post-operaive CKD 4-5 stage in this cohort. We found significative differences between pre and postoperative kidney function, with results similar to other laparoscopic series (19, 23, 25). In the current report we used only the PADUA score system. For our practice, this classification is more simple, fast and intuitive than R.E.N.A.L nephrometry score (8) in the daily clinical practice. This study shows that the PADUA score is associated with WIT. When planning the NNS the surgeon should evaluate several tumor's aspects, not only the tumor size, in order to plan the best strategy for the patients. As reported by Ficarra (7, 20) the nephrometry score systems, like PADUA and R.E.N.A.L score (7, 8) are valid for the preoperative tumor classification and should be included in the international guidelines as a selective criteria for NSS. Furthermore, this study shows that LPN is a valid alternative to OPN and RAPN in high volume centers with high experience in laparoscopic surgery. The main limitation of this study is the retrospective design. Several postoperative oncological outcomes are not evaluated in this study. We select only patients treated by LPN in the last three years. Oncological data, such as recurrence rate and cancer specific survival, were not suitable to evaluate in a short follow-up. As reported by literature, the 10-year risk of recurrence (local and distant) and cancer specific survival are similar between the first 5 year and the last 5 years after surgery and experts suggest to never stop follow-up in this patients (19, 23-24-25). Evaluating several oncological outcomes in a short follow-up present more bias. For this reason in this report was focused only on WIT. This aspects, however, can open a way for future studies. The findings from this retrospective single center study reveal that several anatomical aspects can influence the WIT. The patients class risk stratification can help the surgeon in the planning of NSS. The use of nephrometry system should be considered for its inclusion in international guidelines.
Footnotes
Financial support: None.
Conflict of interest: The authors declare that they have no conflict of interest.