
Abstract
Transitional cell carcinoma (TCC) has been well described for its propensity to metastasize to distant sites. Metastases to the soft tissues of the oral cavity from a bladder cancer are extremely rare. We present the case of a 65-year-old man who presented with history of hematuria for 1 month and was found to have high-grade TCC of the bladder. He developed a cheek lesion after 3 weeks, which was diagnosed as metastatic nodule along with pulmonary metastases from high-grade bladder TCC. The patient received chemotherapy followed by the radiotherapy of the cheek lesion, but he succumbed after 3 months due widespread metastatic disease. We also presented a review of the literature regarding this rare presentation.
Introduction
Transitional cell carcinoma (TCC) is the most common histological type of bladder cancer, constituting 95% to 97% of bladder tumors in North America and Europe. Highgrade urothelial carcinoma is known for its propensity for distant metastases. The common sites of metastases from bladder TCC are lung, liver, brain and bone. Metastases to the oral cavity are very rare and only a few cases of TCC of the urinary bladder metastatic to the oral cavity have been reported (1-4). Most of these cases have occurred in the jawbones, and metastases to soft tissue of oral cavity are extremely rare, with only four cases being described in literature (5, 6). We report a case of high-grade TCC of the urinary bladder presenting with a metastatic tumor confined to the soft tissues of the cheek, which is the first case to be reported. The patient had widespread disease at diagnosis and a poor prognosis.
Case Report
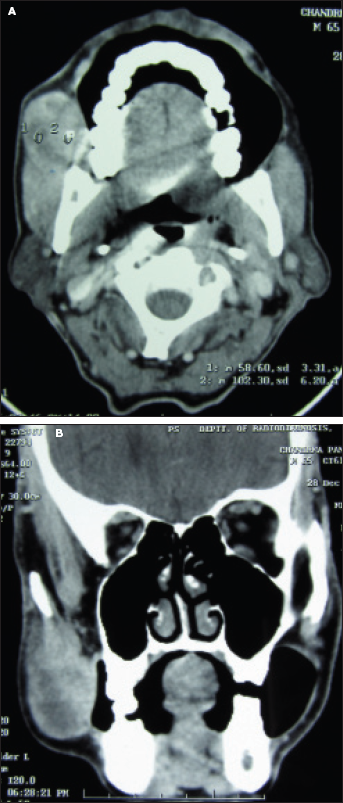
A 65-year-old man presented with a small painless nodule over the right cheek (Fig. 1). Three weeks before, he had presented with irritative voiding symptoms and painless gross hematuria of 1-month duration and was diagnosed to have a bladder mass. Abdominopelvic computed tomography (CT) showed an enhancing solid bladder tumor with enlarged pelvic lymph nodes (Fig. 2A) and multiple pulmonary metastases that were evident on chest x-ray (Fig. 2B). Biopsy of the transurethral resection specimen showed high-grade TCC (Fig. 3A). This time he had a small cheek lesion which was firm to hard in consistency with normal overlying skin and mucosa. Tru-Cut biopsy confirmed metastases from transitional cell carcinoma (Fig. 3B). A head CT showed a metastatic nodule 3.6 × 3.6 × 2.8 cm in the right cheek soft tissues, with involvement of masseter muscle medially and buccinators muscle posteriorly (Fig. 4). He was started on Gemcitabine- and Cisplatin-based chemotherapy, but the cheek metastasis progressed rapidly until limiting the mouth opening; for this reason, palliative external beam radiotherapy was given. The oral lesion was initially reduced after radiation, but the movement of mandible was still restricted. Three months after the diagnosis, the patient succumbed due to widely metastatic disease.
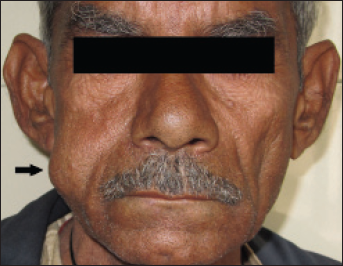
Metastatic nodule at right cheek (solid arrow) with normal overlying skin.
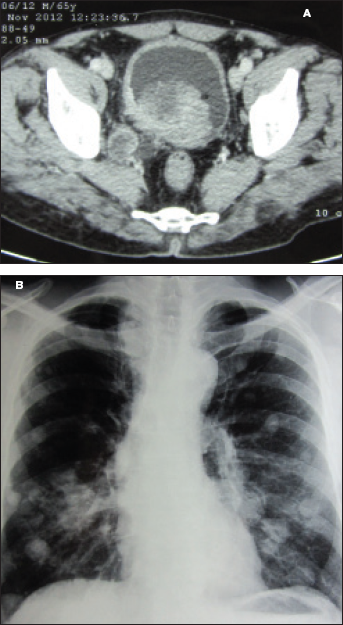
Contrast-enhanced computed tomography demonstrating a large heterogeneously enhancing bladder mass, arising from posterior and right lateral wall with enlarged metastatic iliac lymph nodes
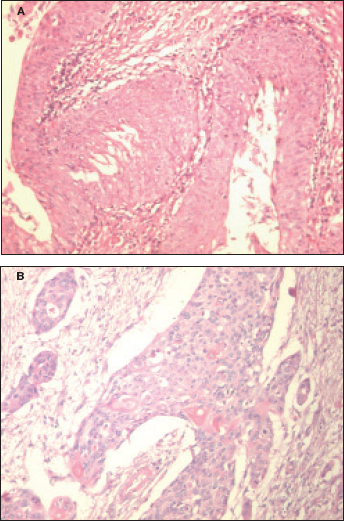
Histopathology microphotographs of the primary bladder tumor
Discussion
Metastatic tumors to the oral and maxillofacial region are rare, accounting for approximately 1% of all oral malignant tumors (6). The most commonly reported primary sites for oral cavity metastases are the breast, lung, kidney, bone and colon (6, 7). Most of these cases are reported to occur in molar and premolar regions of jawbones rather than soft tissues of the maxillofacial region because of abundant bone marrow and peculiar vascularization at these sites (8-10). Like other primary sites, metastatic tumors in the oral cavity from urinary bladder are uncommon and occur mostly in the jawbones (5). Metastases to the oral soft tissues without bony involvement are extremely rare. On extensive literature search using pubmed/medline/scopus/ embase search engines, since 1970 we have been able to find only four cases of metastases to oral cavity soft tissues without any bony involvement, which were arising from TCC of urinary bladder (1-4), and are summarized in Table 1. The current case is the fifth case of bladder TCC to metastasize to oral cavity soft tissues and the first one to cheek with normal overlying skin and buccal mucosa. Oral metastases are potentially misdiagnosed as other primary oral lesions owing to their low incidence; therefore a histological diagnosis is always necessary (10). Differential diagnoses include primary malignancies of the oral cavity, the commonest being squamous cell carcinoma (>90%). Other malignancies of the oral cavity include minor salivary gland tumors, lymphomas, and rare mesenchymal tumors including those showing differentiation to fibroblasts, lipo-blasts, blood vessels, muscle and nerve (11, 12). Benign lesions that should be considered in differential diagnosis are pyogenic granuloma, keratoacanthoma, follicular lym-phoid hyperplasia, granular cell tumor and tuberculosis. In the present patient, a painless nodule over the right cheek was noticed with normal overlying skin and mucosa, having a potential to misdiagnosis. However, as the patient was recently diagnosed to have metastatic bladder cancer, oral metastasis was considered as a first possible diagnosis and a histopathological diagnosis was sought, which confirmed it to be a metastatic lesion. Subsequent CT scan outlined metastatic lesion.
Literature Review Summarizing the Previously Reported Cases of Oral Cavity Soft Tissue Metastases from Tcc of Urinary Bladder
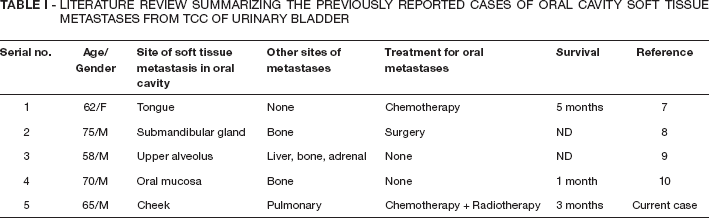
Metastases to the oral cavity from genitourinary malignancies are manifestations of widespread metastatic disease, so it is difficult to offer curative treatment (13). However, to control the local symptoms of pain, bleeding and improve the quality of life, the palliative treatment in the form of radiotherapy is offered (4). The prognosis for patients with oral metastases is poor and most patients die within several months to 1 year after diagnosis (1, 4). TCC is a relatively chemosensitive tumor; therefore chemotherapy is a viable therapeutic option for metastatic disease.
We also want to emphasize the frequent oral and gingival infective complications that might occur during cancer chemotherapy, particularly in patients with poor general conditions. Chemotherapy leads to opportunistic infections contributing to morbidity and mortality in cancer patients. The antimeta-bolic effects of chemotherapy cause a breakdown of host defenses, leading to ulceration and invasion by commensal aerobic and anaerobic bacteria. Mouth ulcerations afflict most patients receiving chemotherapy and have been associated with viridans streptococcal bacteremia (14). Noma (cancrum oris), common in malnourished children, is a penetrating disease of the soft and hard tissues of the oral cavity, with resulting necrosis. It's counter-part seen in patients on chemotherapy, is caused by tissues invasion by Bacteroides, Fusobacterium, and other normal inhabitants of the mouth. Candida albicans and related fungi are also normal commensals inhabiting the oral cavity that invade under conditions of altered host defenses. The prevalence of oral fungal infection in cancer patients during chemotherapy or head and neck radiotherapy has been reported to be 40% during treatment compared to 7.5% before treatment. Pseudomembranous candidiasis (thrush), erythematous candidiasis, and angular chelitis are the common clinical presentations, whereas chronic hyperplastic candidiasis is rare. Oral infections can cause fatal fungal sepsis, especially with non-albicans species such as Candida tropicalis (15). Oral viral infections during cancer chemotherapy include herpes simplex, varicella zoster, Epstein-Barr virus, and cytomegalovirus infections. Severe infections may lead to dehydration, malnutrition due to decreased oral intake, and even life-threatening complications including encephalitis and disseminated infection (14). Other infections during cancer chemotherapy include dental infections, caries, and abscesses in approximately 6% of patients (16).
The disease progressed rapidly in the index patient, while on chemotherapy. Radiotherapy was offered to control local tumor growth and symptoms. Growth subsided initially, but did not respond well to chemotherapy and radiotherapy. The patient succumbed within 3 months due to the highly aggressive behavior of disease. The present case highlights that clinicians should be aware that a highgrade bladder tumor may also present with cheek metastases and this may provide a clue towards widespread disease and poor prognosis.
Footnotes
Financial support: The authors did not receive any financial support for this study.
Conflict of Interest: No conflict of interest was identified.
Informed consent was obtained by all participants. The study was in adherence with the Declaration of Helsinki. The manuscript does not report the results of an experimental investigation on human subjects.