
Abstract
Objective—
To compare the efficacy of 2 strategies that use nystatin to prevent thrush and Candida esophagitis in kidney transplant recipients.
Methods—
A retrospective chart review was conducted of adult kidney transplant recipients at our center, where the protocol for prophylaxis against fungal infection was changed in March 2013. Before the protocol change, kidney transplant recipients received nystatin for 1 month (before group) and after the change they received nystatin for the duration of admission (after group). The primary outcome measure was the incidence of thrush and Candida esophagitis within 3 months after transplant. Analyses were conducted on all kidney transplant recipients (intention to treat) and on only those kidney transplant recipients who received at least 1 dose of nystatin (modified intention to treat). Additional data collected included the duration of nystatin and immunosuppression regimens. The Student t test and Fisher exact test were used to calculate P values for continuous and categorical data.
Results—
A total of 84 kidney transplant recipients, 42 in each cohort, were included in the analysis. The groups did not differ significantly at baseline. Nystatin was administered for a mean of 29 days in the before group and 5.74 days in the after group. Overall, 3 kidney transplant recipients (4%), all from the after group, experienced an episode of thrush and no patients experienced Candida esophagitis. Two recipients who experienced thrush did not receive any nystatin.
Conclusions—
Limiting the administration of nystatin to the duration of admission after transplant may be sufficient for prophylaxis of fungal infections in kidney transplant recipients.
The risk of infection by a variety of pathogens is increased in solid-organ transplant recipients because of the immunosuppression necessary to maintain their allografts. This risk is a product of the dynamics between a spectrum of different factors, including past and current exposure to pathogens, disruption of mucocutaneous barriers, underlying immunodeficient and metabolic conditions, neutropenia, and intensity of immunosuppressive antirejection medications. During the posttransplant period, the effects of potent induction immunosuppressive medications as well as the intensity of maintenance immunosuppressive medications are attenuated, thus gradually lessening the risk of infection. As such, transplant centers typically give their solid-organ transplant recipients antibacterial, antiviral, and antifungal medications in order to protect against infection while they are most at risk.1,2
The risk of fungal infections differs with the type of organ transplanted, with a reduced risk in kidney transplant recipients as compared with other transplant recipients.1–3 The reported incidence of fungal infections in the kidney transplant population varies greatly, with candidiasis accounting for the majority of cases. The most common source of these infections is colonization of the oral mucosa with Candida, one of the organisms that comprise the microbiota of the oropharyngeal and gastrointestinal tracts. Oropharyngeal infection with this opportunistic organism is typically localized to the superficial mucosa; however, it can predispose patients to esophageal candidiasis, which is associated with significant morbidity and a higher risk for disseminated infection, can be a cause of significant pain, and can interfere with medication administration. It has been reported that oropharyngeal candidiasis has preceded approximately 80% of episodes of Candida esophagitis in kidney transplant recipients.4–7
Owens and colleagues 8 have demonstrated the development of oral thrush in up to 50% of kidney transplant recipients not receiving prophylaxis for fungal infections. Despite this prevalence, the risk of advancement to more invasive disease, and the clinically significant morbidities of oropharyngeal candidiasis, no consensus has been reached on the best agent and duration of prophylaxis against fungal infections in kidney transplant recipients.2–4,6,9–11
On March 12, 2013, the protocol for preventive treatment of thrush and esophageal candidiasis in kidney transplant recipients at our institution was changed. Therefore we conducted a retrospective chart review in order to compare the effectiveness of 2 strategies for use of nystatin suspension to prevent thrush and esophageal candidiasis in kidney transplant recipients.
Methods
Study Design and Population
This single-center retrospective chart review, which was approved by the institutional review board, was conducted for adult patients who received a kidney transplant at Yale-New Haven Transplantation Center between October 2012 and October 2013. Patients were identified by using the Yale-New Haven Transplantation Center's database of past kidney transplant recipients and were selected for enrollment in the study in chronological and reverse chronological order from immediately before and after the protocol for preventing fungal infection in kidney transplant recipients was changed on March 12, 2013. Before this change, kidney transplant recipients were prescribed nystatin suspension 500 000 units to orally swish and swallow 4 times daily for 1 month after transplant. After the change, the duration of prophylaxis against fungal infection with nystatin was decreased from 1 month to the duration of hospital admission after transplant. Only those patients within 3 months of transplant were excluded from the study.
Data Collection
Data collection included examination of both inpatient and outpatient electronic medical records for patient demographics as well as information regarding the patient's cause of renal disease, date of transplant, date of hospital discharge after transplant, and rejection episodes, if any. In order to assess the burden of immunosuppression, data on the medications used for induction therapy, as well as the maintenance immunosuppressive medications and their corresponding doses or levels also were collected. Finally, the timing, dosing, and duration of prophylaxis with nystatin suspension, any changes in this regimen, and concomitant antifungal medications were recorded for each patient. Additionally, if a patient had a fungal infection develop, data on the cause of the infection, date of diagnosis, treatment, and need for hospitalization were retrieved. The primary outcome measure in this study was the incidence of thrush and Candida esophagitis within 3 months after transplant.
Statistical Analysis
Analyses were conducted both on all kidney transplant recipients (intention to treat) and on only those kidney transplant recipients who received at least 1 dose of prophylaxis with nystatin suspension (modified intention to treat). Data were analyzed by using descriptive statistics, as well as the Student t test and Fisher exact test, which were used to calculate P values for continuous and categorical data.
Results
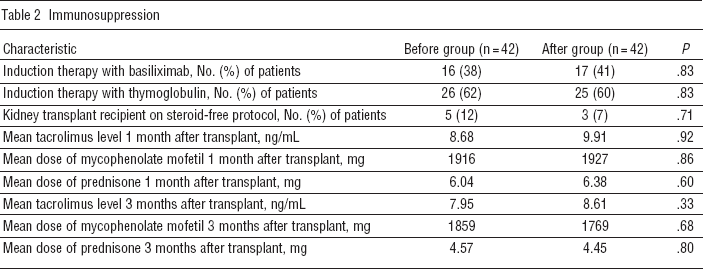
A total of 84 kidney transplant recipients, 42 patients who received a transplant before the protocol change (before group) and 42 patients who received a transplant after the protocol change (after group), were included in the analysis. Baseline characteristics are presented in Table 1. Of the total patients included, 65% were male and 60% were white. Nearly half of the transplants were from a deceased donor, and 88% were the patient's first kidney transplant. Hypertension and diabetes mellitus were the 2 comorbid conditions to which the cause of kidney disease was most commonly attributed. The 2 groups did not differ significantly in terms of baseline characteristics. Additionally, the 2 groups were similar with respect to immunosuppression (Table 2). Approximately 60% of patients in each group received rabbit antithymocyte immune globulin for induction immunosuppression, and all patients were maintained on tacrolimus, mycophenolate mofetil, and prednisone, excluding 5 patients in the before group and 3 patients in the after group who were maintained without steroids beyond postoperative day 4. Mean doses of mycophenolate mofetil and prednisone, as well as tacrolimus trough levels, at 1 and 3 months after transplant were similar between groups.
Baseline characteristics of patients in the study a
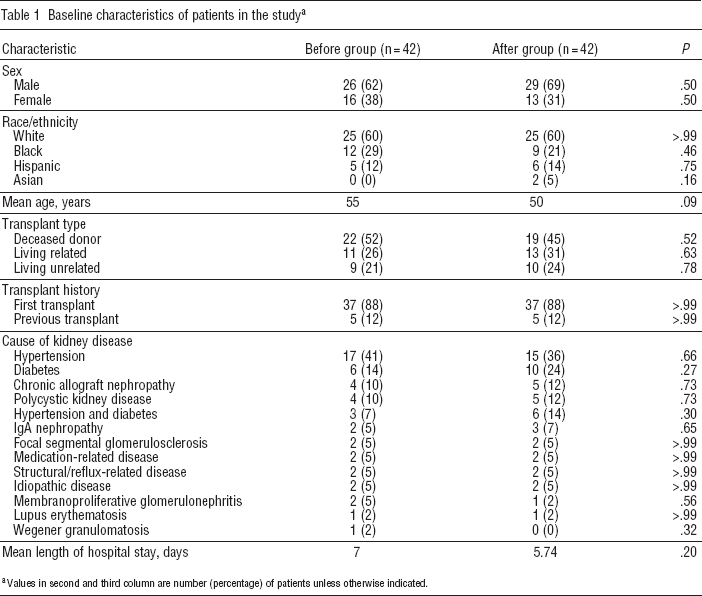
Values in second and third column are number (percentage) of patients unless otherwise indicated.
Immunosuppression
The mean duration of prophylaxis with nystatin was 29 days in the group of patients who received a kidney transplant before the change in protocol (Figure 1). In contrast, after the protocol was changed to include nystatin suspension for a duration equivalent to that of the patient's hospital stay, patients received prophylaxis with nystatin suspension for a mean duration of 5.7 days (P< .05). Furthermore, although all of the patients in the before group received prophylaxis against fungal infection with nystatin, 7 patients (17%) in the after group did not receive any nystatin suspension. Overall, 3 kidney transplant recipients (4%), all of whom were from the after group, experienced an episode of thrush and none of the patients experienced Candida esophagitis (Figure 2). Two of the kidney transplant recipients experiencing thrush did not receive any prophylaxis with nystatin suspension. The mean lengths of hospital stay in the before and after groups were similar at 7 and 5.4 days, respectively (P = .20). None of the kidney transplant recipients with thrush required hospital readmission.
Discussion
Determination of the optimal duration of prophylaxis against fungal infection in kidney transplant recipients is necessary in order to prevent the notable morbidity caused by such infections. Different transplant centers use different antifungal medications for prophylaxis; minimizing the duration of administration of each of these agents as much as possible without increasing the risk for fungal infections is advantageous. Both topical medications, such as nystatin oral suspension and clotrimazole troches, as well as systemic medications, such as fluconazole, have been used for prophylaxis against fungal infection at different transplant centers. Each strategy, however, has disadvantages. Nystatin and clotrimazole are known to be unpalatable, must be administered several times a day, and often are associated with poor patient adherence. Clotrimazole also interacts with calcineurin inhibitors, which are used as maintenance immunosuppressive medications in transplant patients. Fluconazole, while well-tolerated and more convenient for patients, is associated with a number of significant adverse effects and also alters serum levels of calcineurin inhibitors.3,6,8–14
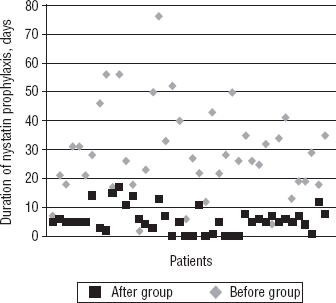
Duration of prophylaxis with nystatin suspension.
In addition to a lack of community standard regarding the agent of choice, little has been published about the optimal duration of prophylaxis against fungal infection in kidney transplant recipients.9–12 The Kidney Disease Improving Global Outcomes guidelines do suggest oral and esophageal Candida prophylaxis for 1 to 3 months after transplant. Conversely, in a review article published in 2013, the American Society of Transplantation Infectious Diseases Community of Practice comments that, because of the low risk of infection, fungal prophylaxis is not warranted after kidney transplant. However, these 2 sets of recommendations appear to be primarily based on a low level of evidence and expert opinion.9,10
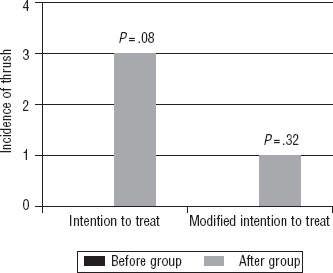
Incidence of thrush.
The results of this retrospective analysis suggest that limiting the administration of nystatin suspension to the duration of admission after transplant may be sufficient for prophylaxis of fungal infections in kidney transplant recipients. The incidence of thrush or esophagitis did not increase significantly in the patient group following our center's change in protocol to a shorter duration of prophylaxis with nystatin. Unexpectedly, as shown in Figure 1, the before group received prophylaxis against fungal infection for a wide variety of durations, with approximately 40% of patients receiving prophylaxis for longer than 30 days. This variability, however, did not alter the results of the study because there were still not significantly more episodes of thrush or esophagitis in the after group.
This study had several limitations. The study is limited because of its retrospective, observational, and single-center design. The development of thrush can be affected by numerous variables, such as a lack of glycemic control and exposure to organisms that were not accounted for and may have influenced the results. Because the 2 groups of patients received their transplants at different periods in time, the ubiquity of organisms in the environment to which each group of patients were exposed could have differed. Additionally, because of the limited number of patients included in the study, no power analysis could be conducted, and thus the study may have lacked the power to detect a difference in thrush episodes between the 2 treatment arms. An additional limiting factor of the study was that patients in the before group received prophylaxis for a wide variety of durations, thus possibly clouding analysis of the results.
Despite these limitations, this study is the first attempt to determine the optimal duration of prophylaxis against fungal infection in kidney transplant recipients. The number of episodes of thrush or esophagitis did not differ significantly between the 2 groups of patients, demonstrating that limiting the duration of nystatin suspension to the duration of hospital admission after transplant may be sufficient for prophylaxis against fungal infections in kidney transplant recipients. Additionally, despite the opinion of some experts that kidney transplant recipients do not require prophylaxis against fungal infection, this study confirmed the necessity of such prophylaxis in kidney transplant recipients, as approximately 30% of patients inadvertently not receiving prophylaxis did experience an episode of thrush. However, owing to the restricted population and time frame of this study, additional prospective studies are essential in order to determine the optimal duration of prophylaxis against fungal infection for kidney transplant recipients.
Footnotes
None reported.