
Abstract
Double dislocations of the finger interphalangeal and/or metacarpophalangeal joints are a rare entity. Sixty-four cases of distal and proximal interphalangeal joint double dislocations have been previously reported. Five cases of metacarpophalangeal and interphalangeal double dislocations of the thumb have also been reported. Only one case has been reported in the English literature regarding simultaneous dislocations of the distal interphalangeal and metacarpophalangeal joints in the nonthumb digit. The directions of the dislocation were the same; both were dorsal. We report, to our knowledge, the first ever case of a double dislocation a non-thumb digit in opposing directions—volar at the metacarpophalangeal joint and dorsal at the distal interphalangeal joint.
Case Report
A 45-year-old man, right-hand dominant, sustained an injury to the long finger of his non-dominant hand after losing control of his bicycle and falling over his handles. He was seen in the emergency room at a local hospital, where X-rays obtained showed a dorsal dislocation of the distal interphalangeal (DIP) joint and a volar dislocation of the metacarpophalangeal (MCP) joint of the left long finger (Fig. 1a–c). Neurovascular examination of the digit was normal.
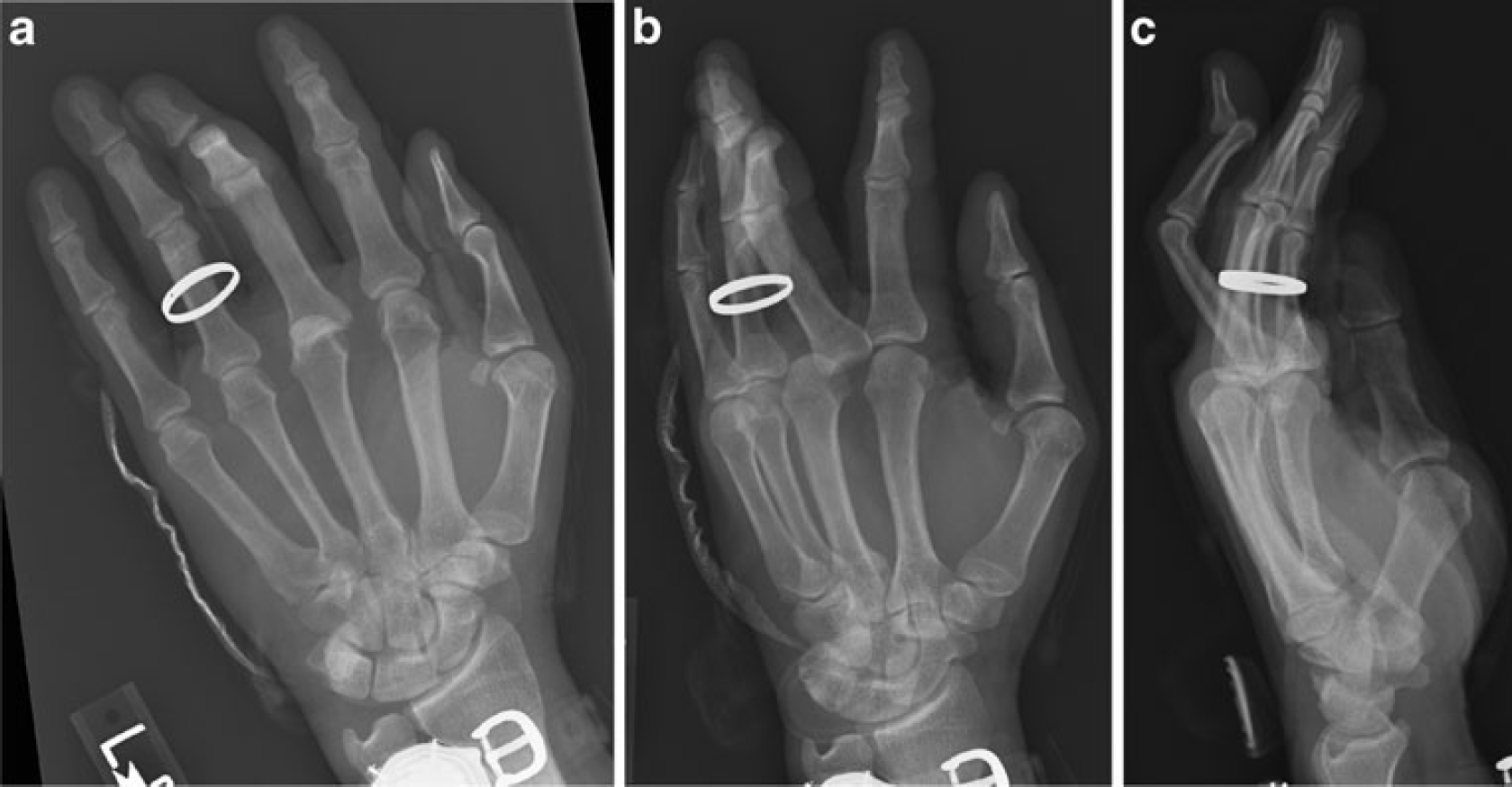
X-rays of the left hand:
A closed reduction of the double dislocation was performed in the emergency department utilizing a digital block. Post-reduction X-rays obtained in the emergency room showed restoration of articular congruity at both joints (Fig. 2a, b). Neurovascular exam after reduction was also normal. The patient was placed into a combined volar and dorsal splint with the digit in intrinsic plus.
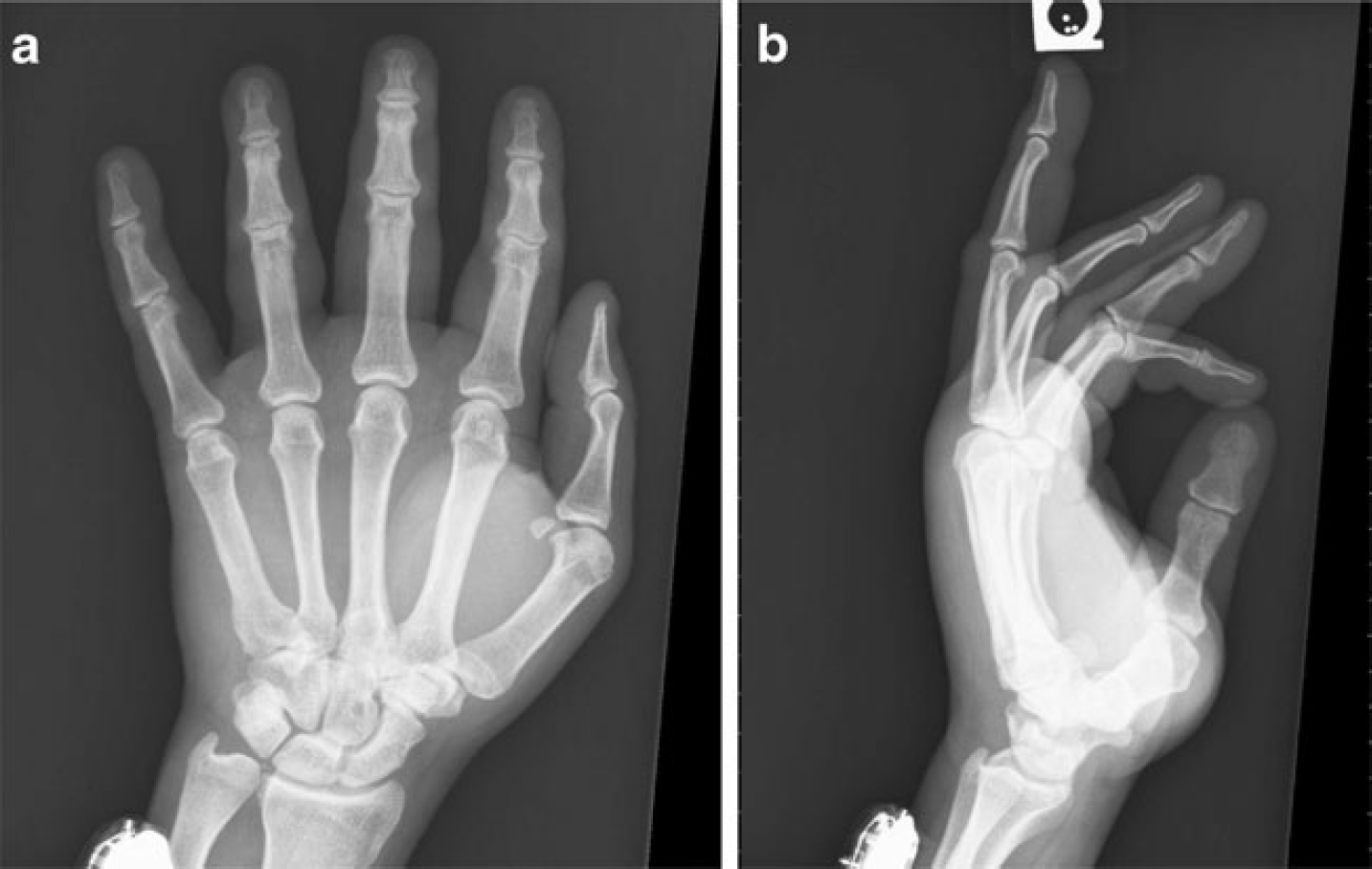
A/P and Lateral X-rays at 2 week follow-up showing articular congruity at the MCP and DIP joints of the long finger.
The splint was removed at 2 weeks, and gentle hand therapy was started. Interval examination was performed at 4 weeks, followed by a final follow-up at 12 weeks. At the final follow-up, the patient exhibited painless active range of motion of the MCP, PIP, and DIP joints of 0–90°, 0–95°, and 0–85°, respectively (Fig. 3a–d). Coronal plane testing of the MCP, PIP, and DIP joints in full extension and flexion showed no instability. Grip strength at the 12-week follow-up was 48 kg in the injured hand and 56 kg in the contralateral dominant hand (Jamar Dynamometer, Smith & Nephew). He complained of no feelings of instability at the affected joints and reported no loss of function.
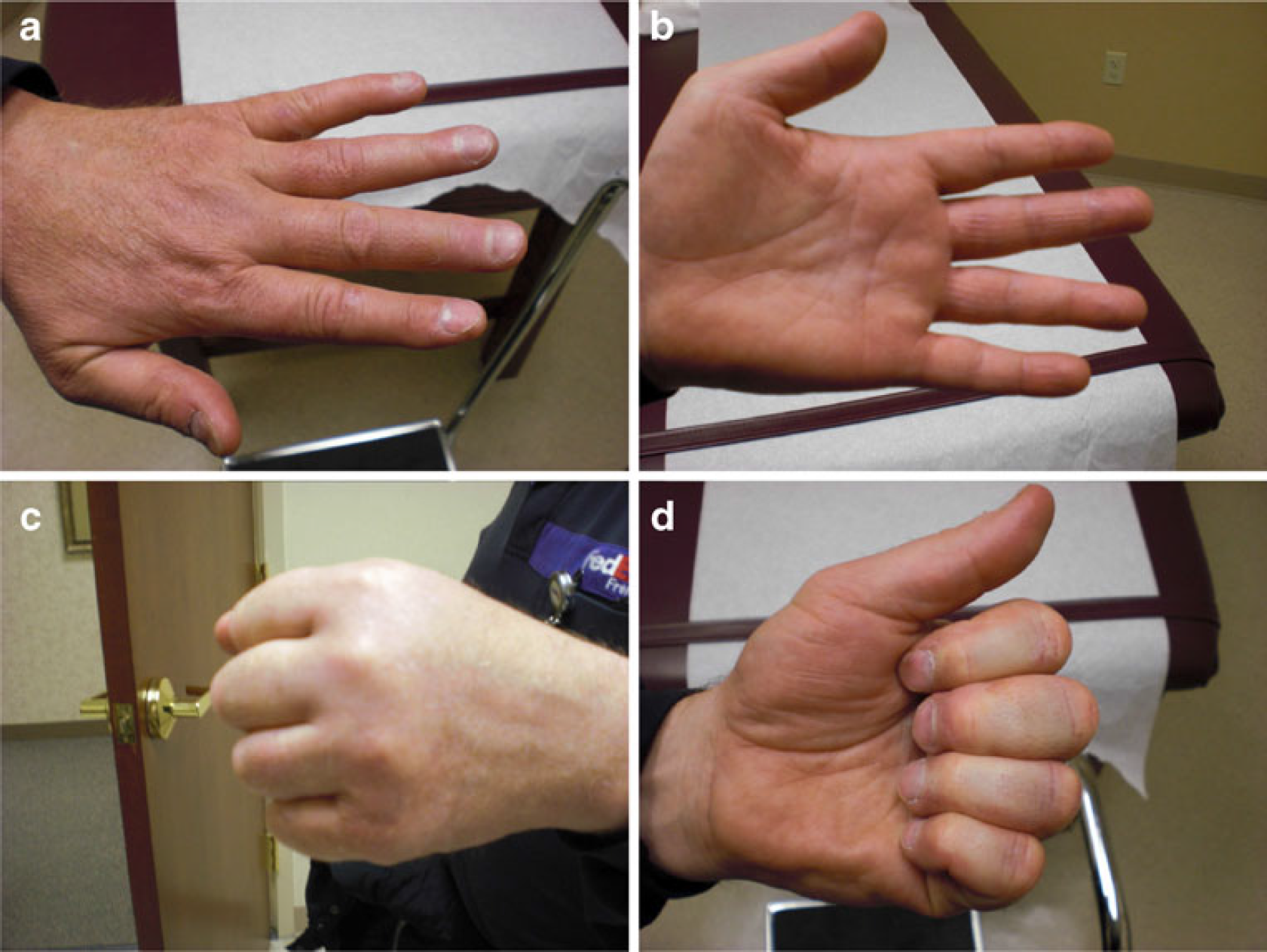
At 12 weeks follow-up the patient exhibited full active range of motion in flexion and extension at the MCP, PIP, and DIP joints of the long finger.
Discussion
The first case of a double dislocation of a digit was reported in 1874 by Bartels [3]. Since then, numerous cases of distal and proximal interphalangeal (PIP) joint double dislocations have been recorded [1]. Additionally, several cases of double dislocations have been reported in the thumb [4,5,7–9]. The first case of a double dislocation whereby the PIP joint was bypassed was reported by Anderson in 1995 [2]. Our case differed from theirs in that the dislocations occurred in different directions versus the same direction in Anderson's.
A dorsal dislocation at the DIP joint occurring concurrently with a volar dislocation of the MCP joint has not previously been reported in the orthopedic literature. The unique nature of this injury—digital dislocations in non-consecutive joints and in opposite directions—can be difficult to analyze from a mechanistic standpoint. It has been shown that some combination of an axial and hyperextension load applied to a digit, specifically at the distal phalanx, can cause a dorsal dislocation at the distal joint [1,2,6].
Theoretically, the continued force on the hyperextended digit would then disrupt the proximal volar structures, such as the PIP joint volar plate and collateral ligaments, resulting in a dorsal dislocation at this joint. However, in our case, this joint was bypassed and possibly became a post by which the continuing energy manifested as a volar dislocation at the MCP joint. Once again, we can only surmise from the injury X-rays and the patient's narrative as to the exact biomechanics causing the injury.
Closed reduction of this “divergent double dislocation,” not previously reported in the orthopedic literature, was successful. The patient's outcome after a short period of splinting, followed by hand therapy, resulted in a fully functioning hand and long finger.