
Abstract
Background
We desired information from the recent, current, and future matched hand surgery fellows regarding their residency training, number of interviews, position matched, cost of interviewing, influences, opinions on future hand training models, and post-fellowship job information.
Method
Institutional review board approval was obtained from our institution to submit an online survey. An email was sent to the coordinators of all US Hand Fellowships to be forwarded to their fellows with graduation years 2011, 2012, and 2013, as well as directly to the fellows if their email addresses were provided. Data on the application process, relative importance of program attributes, and opinions regarding optimal training of a hand surgeon were collected. Statistical analysis was performed with respect to the training background and graduation year of the respondent.
Results
The survey was completed by 137 hand surgery fellows. Seventy-one percent of the survey responders were from an orthopedic residency background, 20 % from plastic, and 7 % from general surgery. Forty-four percent of all of the respondents matched into their first choice. The type of operative cases performed by the current fellows was most often selected as very important when making their rank list. Seventy-seven percent of the respondents reflected their personal preference in fellowship model to be a 1-year fellowship program.
Conclusions
The field of hand surgery is unique in that it has residents from multiple training backgrounds who all apply to one fellowship. The current fellowship model allows for diversity of training and the possibility of obtaining a second fellowship if desired.
Introduction
Hand surgery fellowship training is unique in that programs may accept applicants from three different residency backgrounds: orthopedic, plastic, and general surgery. In 1986, the Residency Review Committees from the three primary boards agreed to identical special requirements in hand surgery to attain a Certificate of Added Qualifications in Surgery of the Hand. The qualification has historically been defined for patient disorders distal to the elbow requiring subspecialty care. Currently, there is debate among the hand surgery community as to what extent of the upper extremity should be included in hand surgery fellowship training and how long should this process take.
Dr. Robert Szabo, in his 2010 American Society for Surgery of the Hand (ASSH) presidential address, discussed surveying hand surgery fellowship program directors regarding shortcomings of our current training programs, reflecting a sense that the current training model might be insufficient. He remarked the training could be more comprehensive and the development of a new curriculum may be needed to train our future hand surgeons [7]. Potential ideas have included extending the length of the fellowship to 2 years, extending the scope of the fellowship to include the entire upper extremity, and the develoment of an upper extremity residency to be matched directly out of medical school.
While the hand surgery community has formed committees and the article by Sears surveyed the opinions of the program directors [6], noticeably absent is the opinion of the current hand surgery trainees. Essential to understanding how any changes to the current training model will influence the candidate field, is studying what factors influence residents in the selection of their hand surgery fellowship [1–5]. By understanding these influences, the fellowship training committees and hand surgery fellowship programs may desire to change their interview process and or training models.
We desired information from the recent, current, and future matched hand surgery fellows regarding their residency training, number of interviews, position matched, cost of interviewing, priorities in selecting a program, opinions on future hand fellowship training models, and post-fellowship job information. In ascertaining this data, we sought to analyze it for any differences the respondents had regarding their answers selected based upon their residency background and the year of graduation from hand fellowship.
Methods
Institutional Review Board approval was obtained from our institution to submit an online survey. An email with a survey cover letter and a link to our electronic survey was distributed to our respondent panel. The panel of email addresses was formed from the 77 programs listed on the ASSH website, representing 150 total possible hand surgery fellows per year, for a potential total of 450 respondents. The email was sent to the hand surgery fellowship coordinators to be forwarded to their hand surgery fellows who have or will graduate in the years 2011, 2012, and 2013, as well as directly to the hand surgery fellows, if their email addresses were provided by the coordinators. A total of 143 email addresses comprised our distribution list. The survey was 26 questions and was designed to take 5–10 min to fill out. The survey was analyzed for the responses given, regarding the mean, minimum, maximum, and standard deviation. The online survey tool, Qualtrics.com (Qualtrics Labs, Inc. Provo, UT, USA) was used to design the survey and collect the data. Statistical analysis, including the mean and standard deviation of the data, was performed to analyze the responses based upon the residency type and year of graduation from hand surgery fellowship.
Results
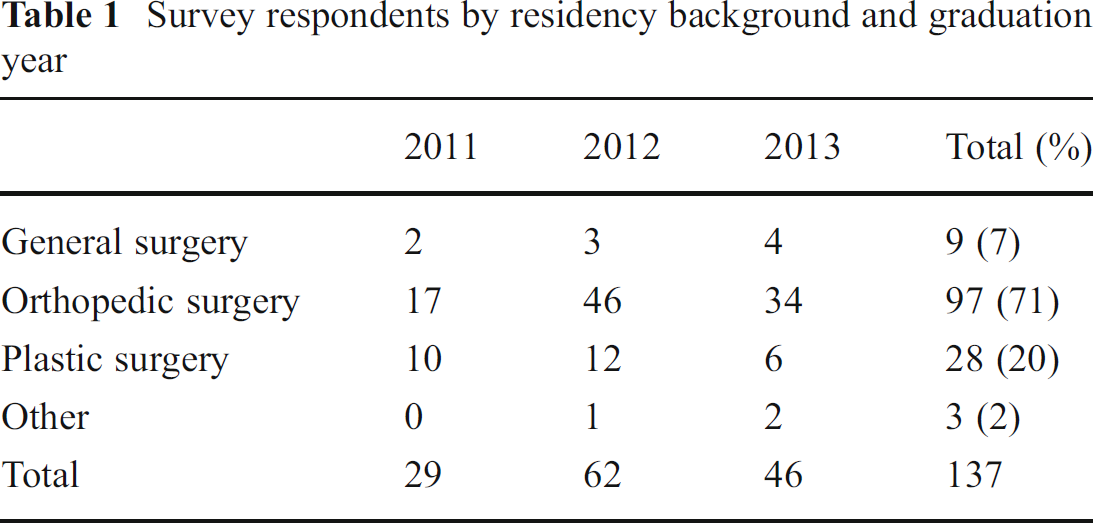
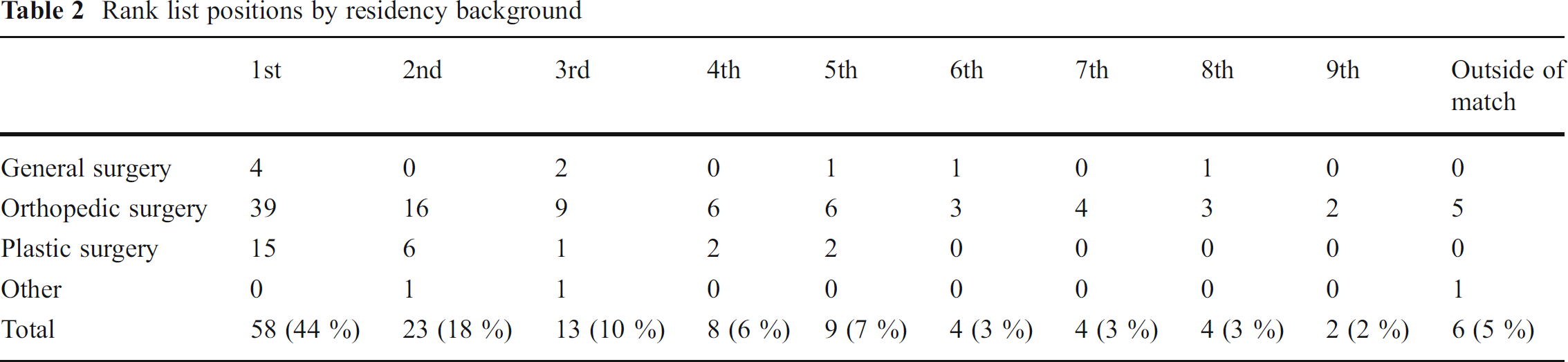
The survey was completed by 137 hand surgery fellows. Seventy-one percent of the survey responders were from an orthopedic residency background, 20 % from plastic, and 7 % from general surgery (Table 1). Forty-four percent of all of the respondents matched into their first choice, 18 % matched into their second choice, and 10 % matched into their third choice. Two percent matched into their ninth or greater choice and 5 % scrambled into their position outside of the match (Table 2).
Survey respondents by residency background and graduation year
Rank list positions by residency background
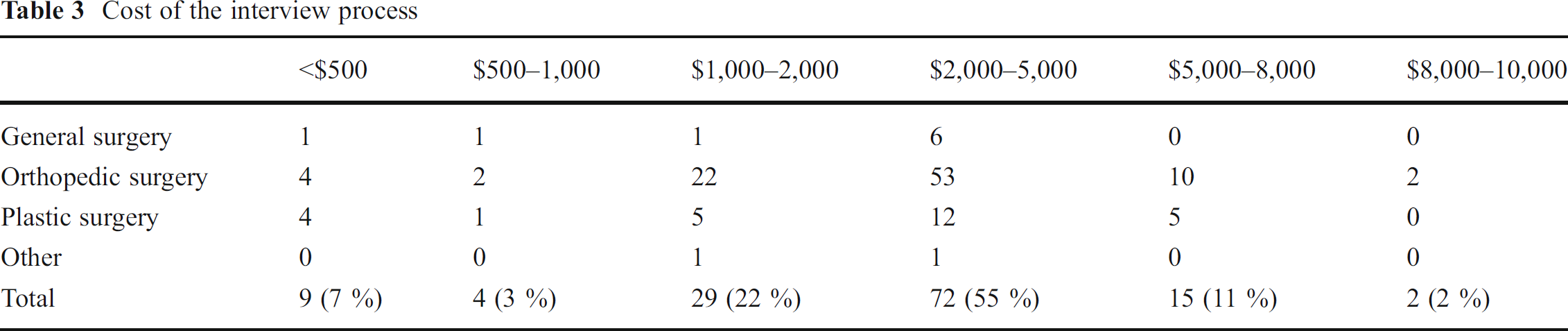
Fifty-five percent of the respondents stated they spent between $2,000–5,000 on the interview process, 22 % spent between $1,000–2,000, 11 % spent between $5,000–8,000, 10 % spent less than $1,000, and 2 % spent more than $8,000 (Table 3), Forty-five percent of the respondents went to 6–10 interviews, 27 % went to 11–15 interviews, 25 % went to 2–5 interviews, 7 % went to 1 interview, and 2 % went to 16 or more interviews (Table 4).
Cost of the interview process
Number of hand fellowship interviews by residency background

When applicants were deciding which programs to apply to, “the variety of cases performed fit my desires for training” was rated the highest of 8.2 (standard deviation (SD)=1.8) on a scale of 1–10 with a 10 equaling very important. Prestige (7.0; SD=2.2), recommendations from mentors (6.9; SD=2.5), and locations (6.8; SD 2.7) were the next most important factors cited when the applicants were applying to specific fellowship programs (Table 5).
Factors for applying to programs
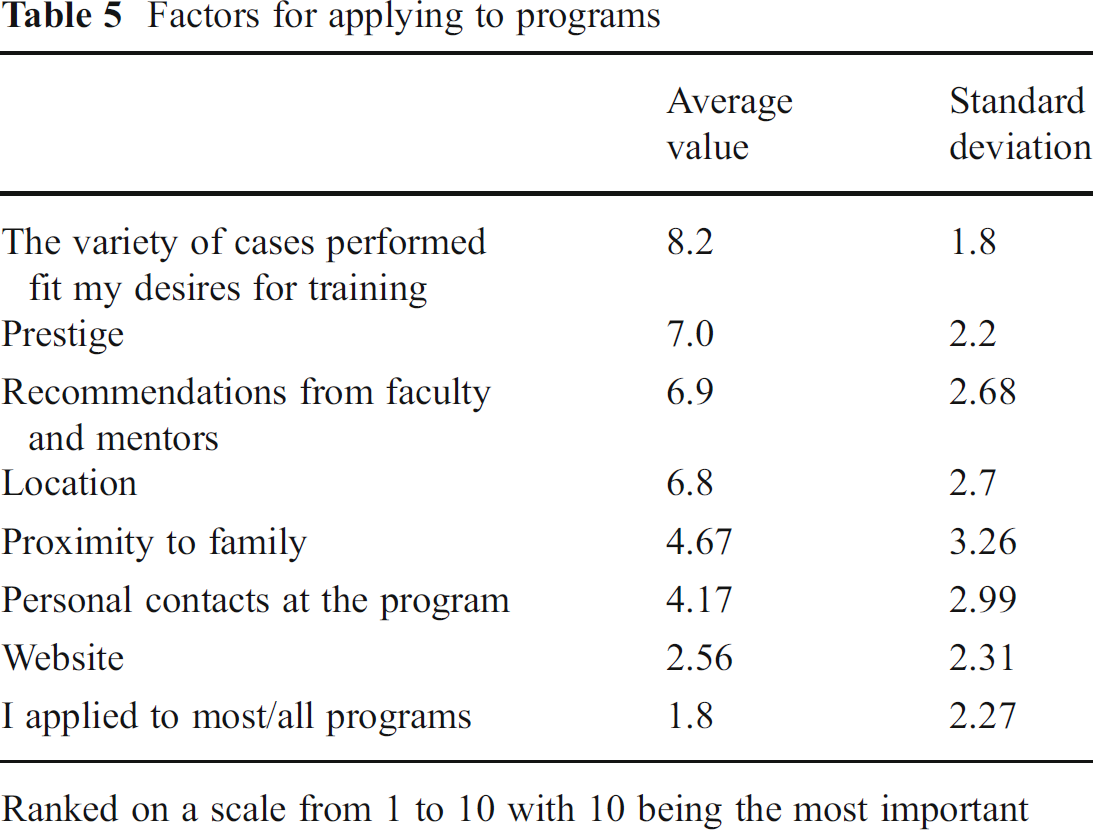
Ranked on a scale from 1 to 10 with 10 being the most important
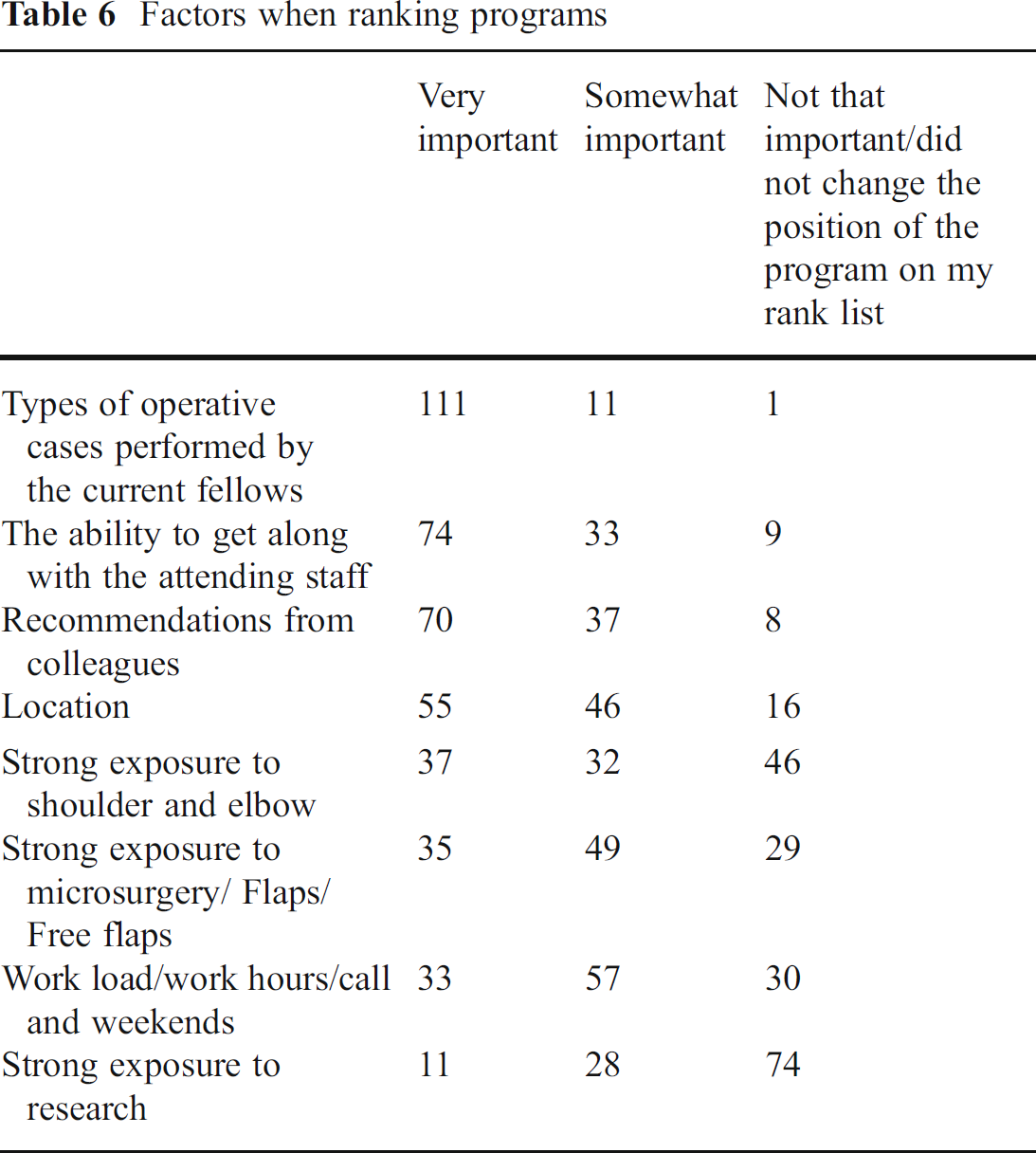
“The type of operative cases performed by the current fellows” was most often selected as very important when making their rank list. “The ability to get along with the attending staff and program director” was the second most often selected as very important, and “recommendations from colleagues and or mentors” was the third most often selected as very important. “Strong exposure to research” was most often as cited as not important when making their rank list (Table 6).
Factors when ranking programs
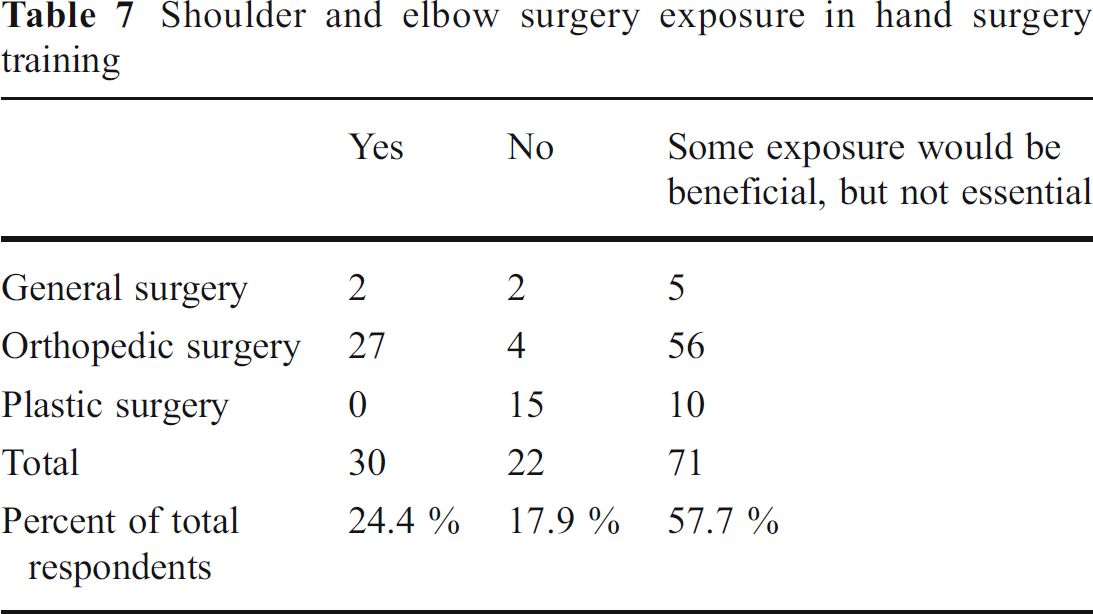
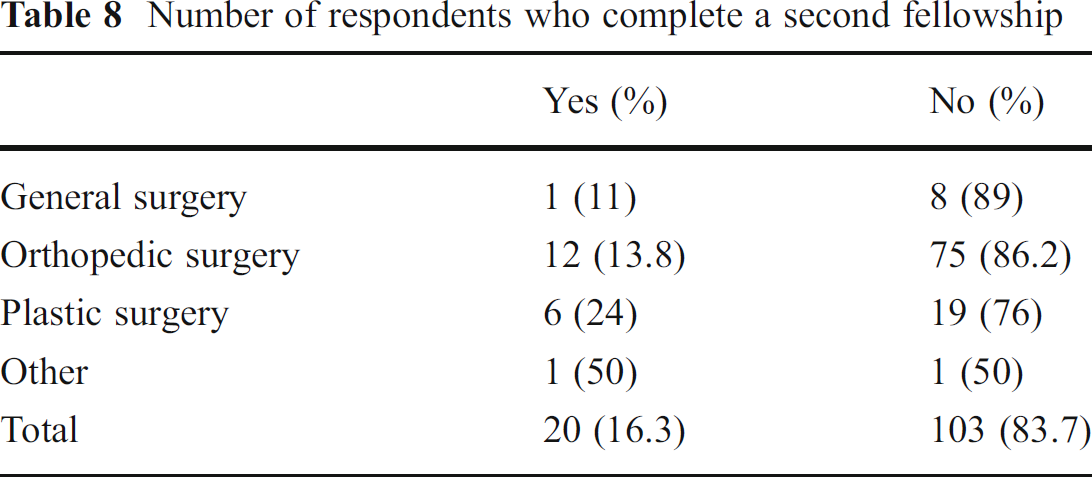
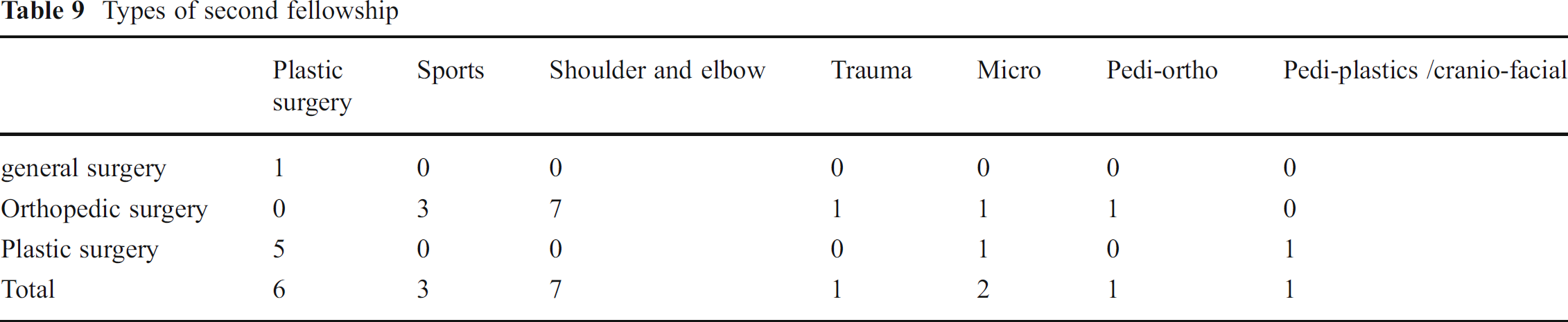
When asked about the composition of the ideal hand surgery fellowship, 58 % reported some exposure to shoulder and elbow surgery is beneficial, but not essential for completion of a hand fellowship, 24 % reported that shoulder and elbow surgery should be included in hand fellowship (of these respondents, 90 % were orthopedically trained), and 18 % felt it unnecessary to include shoulder and elbow surgery in a hand fellowship (of these, 70 % were from plastic, 20 % orthopedic, and 10 % general surgery; Table 7). This sentiment is mirrored in the results we found when asking if the respondent will be pursuing a second fellowship in shoulder and elbow surgery. Eighty-four percent of the respondent stated that Hand Surgery Fellowship will be the only one fellowship they will complete and the remaining 16 % of the respondents noted they have or will be pursuing a second fellowship (Table 8). Of these, shoulder and elbow, sports, plastic surgery, microsurgery, and pediatric orthopedic surgery fellowships will be completed. Only 5 % of the total number of respondents had chosen to complete a second fellowship in shoulder and elbow surgery (Table 9).
Shoulder and elbow surgery exposure in hand surgery training
Number of respondents who complete a second fellowship
Types of second fellowship
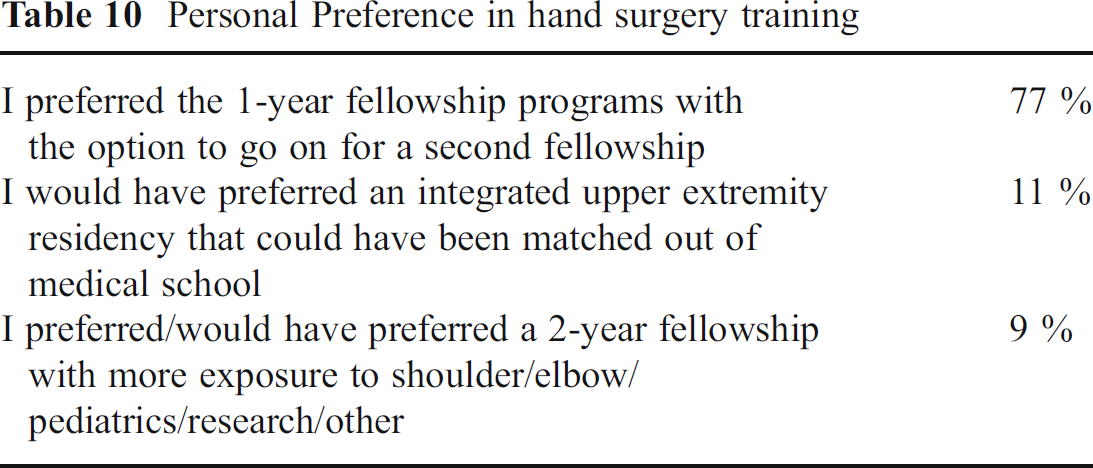
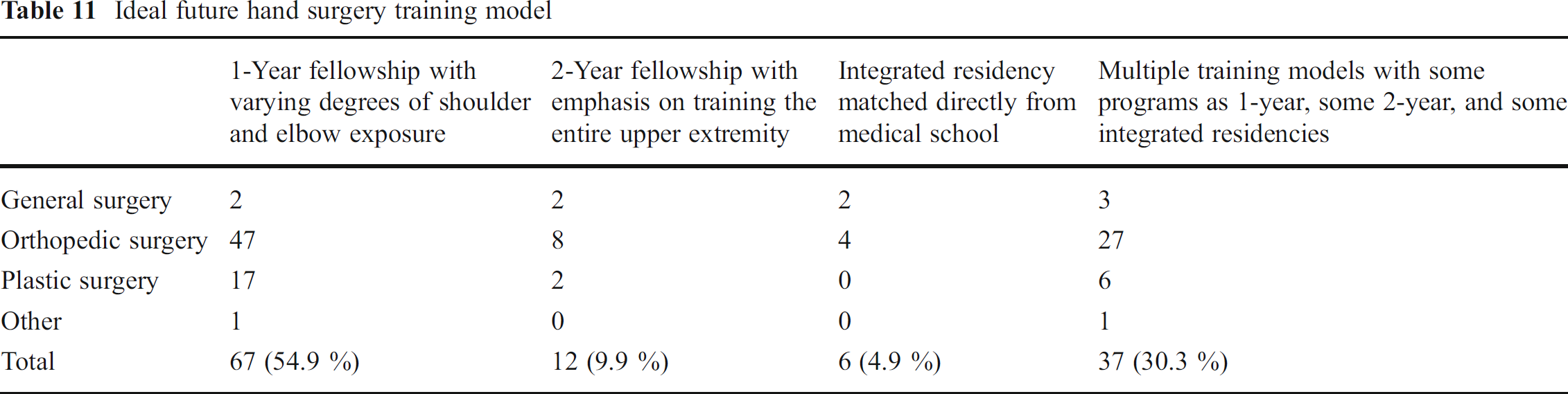
When asked “Which option would best reflect your personal preference in fellowship?”, 77 % selected “I preferred the 1 year fellowship programs with the option to go on for a second fellowship,” 11 % selected “I would have preferred an integrated upper extremity residency that could have been matched out of medical school,” and 9 % selected “I preferred/would have preferred a two year fellowship with more exposure to shoulder/elbow/pediatrics/research/other” (Table 10). Though more than three quarters of the respondents preferred a 1-year program for training, only 55 % thought that it should be the only model for training. Thirty percent thought that multiple training models would be optimal, having some 1-year programs, some 2-year programs, and some integrated residency programs. Ten percent felt hand surgery should be taught as a 2-year fellowship with an emphasis on training the entire upper extremity, and 5 % felt that hand surgery should be taught as an integrated residency, matched directly out of medical school (Table 11).
Personal Preference in hand surgery training
Ideal future hand surgery training model
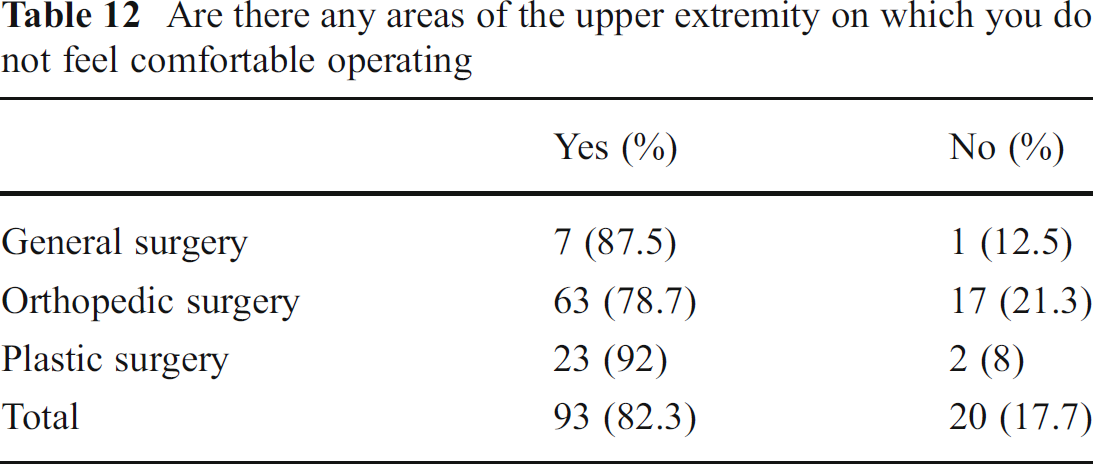
Though few respondents desired mandatory exposure to the entire upper limb, 82 % of the respondents stated there was some area of upper extremity surgery that they did not feel comfortable performing (Table 12). Of these, 59 % selected the “brachial plexus,” 42 % selected “shoulder,” 42 % selected “free flaps,” 24 % selected “elbow,” 23 % selected “pediatric hand surgery,” 4 % selected “wrist arthroscopy,” and 10 % selected “other” stating they have not started their hand surgery fellowship yet (Table 13).
Are there any areas of the upper extremity on which you do not feel comfortable operating
Area/types of surgery on which the respondents do not feel comfortable operating

When asked if they would have preferred a central application company to retrieve and distribute the applications, 84 % selected “yes,” 12 % selected “no,” and 4 % selected “other.” When asked “Would you have considered/gone into hand surgery directly out of medical school if it was offered?” 52 % stated “no,” 27 % stated “maybe,” and 21 % stated “yes.”
Eighty-three percent of the respondents chose to go into hand surgery during residency, 11 % during medical school, and 6 % stated they knew they wanted to go into hand surgery before medical school. Thirty-two percent decided they would go into hand surgery during their post graduate year (PGY) 4, 32 % in PGY 3, 18 % in PGY 2, 8 % in PGY 5, 3 % in PGY 1, and 3 % in PGY 7 or greater year.
When asked to rate the reason they chose to go into hand surgery on a Likert scale with a 0 being “not important” and a 10 being “very important”, the respondents rated “interesting anatomy” the highest with a rating of 8.4, “variety of cases (rare and challenging cases)” rated 8.2, the types of cases performed on a “routine basis (‘bread and butter’ hand surgery)” rated 7.1, “lifestyle” rated 6.2, “I like the office/clinical aspect of hand surgery” rated 6.1, “I like to sit down to operate, ergonomics” rated 5.1, and “money” rated 4.5 (Table 14).
Reasons for choosing hand surgery
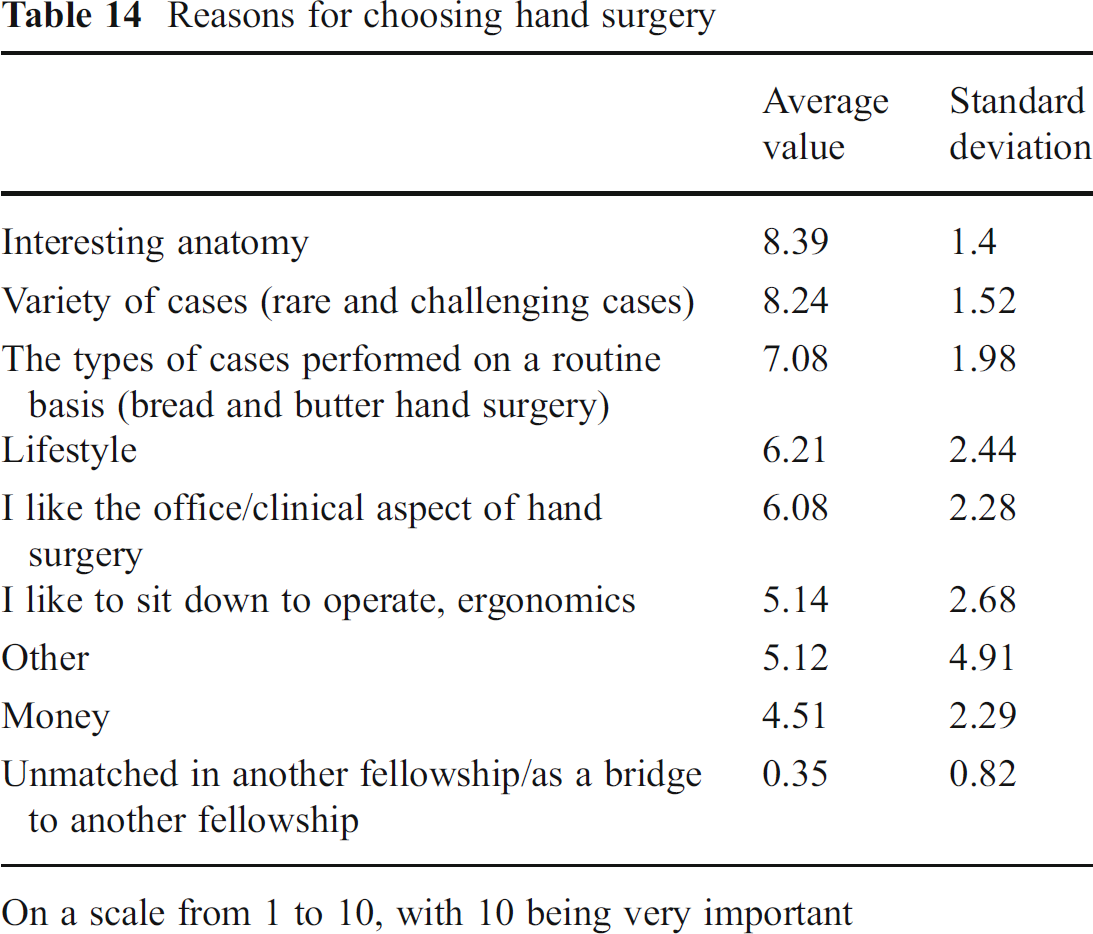
On a scale from 1 to 10, with 10 being very important
Thirty-five percent of the respondents started inter viewing for postfellowship jobs before they had started their hand surgery fellowship, 28 % had not started interviewing for jobs at the time the survey was filled out, and 16 % began interviewing in their 3–4 months of fellowship (Table 15). A broad range of initial base salary was noted and the majority of the respondents noted they had not received a job contract at the time of the survey. Fifty-seven percent stated they had not secured a job at the time of their response to the survey (Table 16). Eleven percent stated their initial base salary was 200,000–250,000, 6 % selected 300,000–350,000, and 5 % selected 250,000–300,000 (Table 17).
When the respondents began job interviews
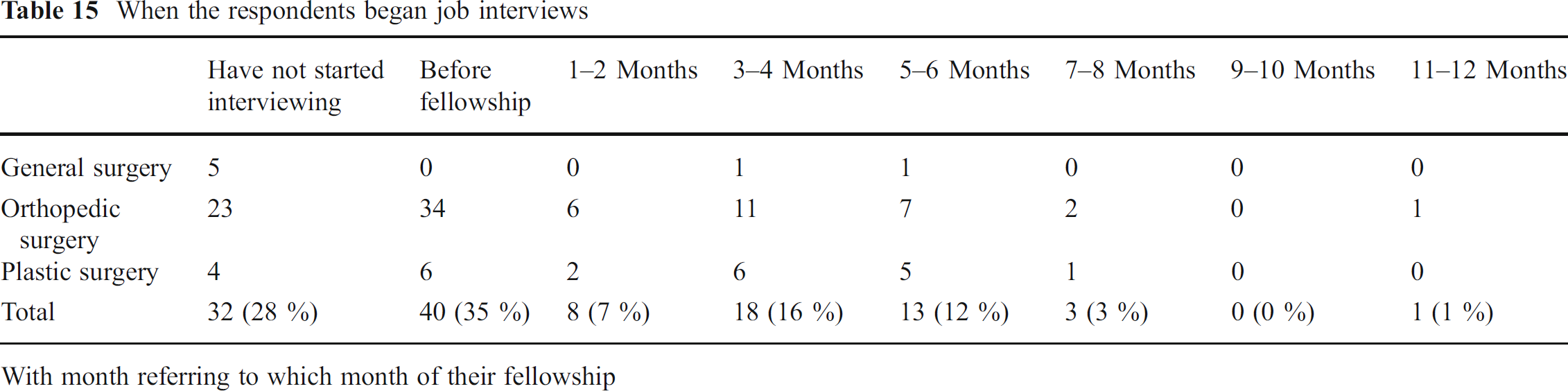
With month referring to which month of their fellowship
When the respondents secured a job contract
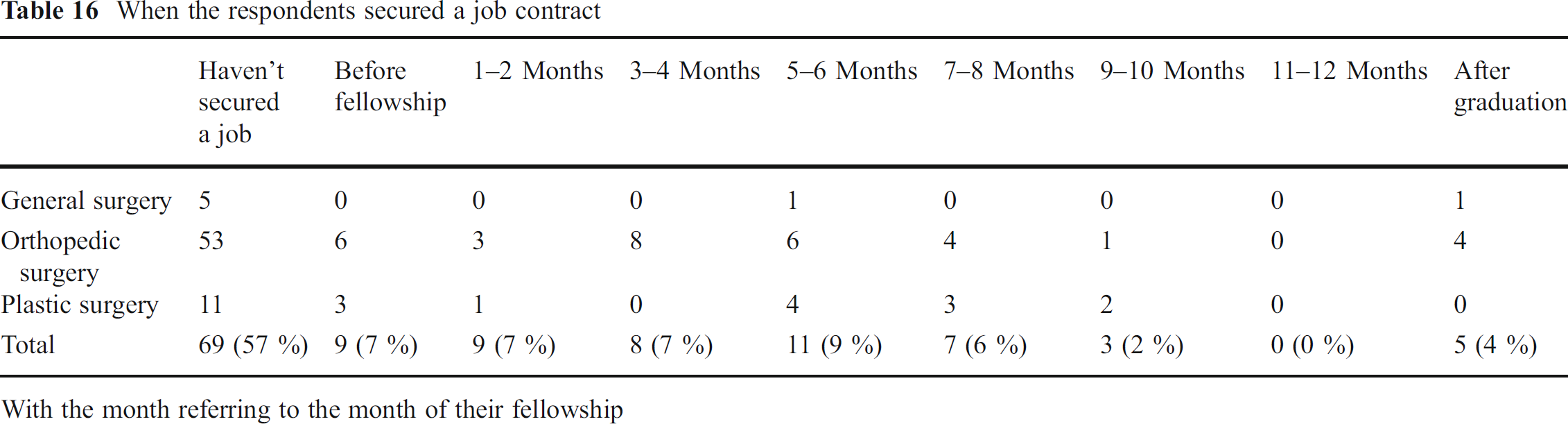
With the month referring to the month of their fellowship
Initial base salary
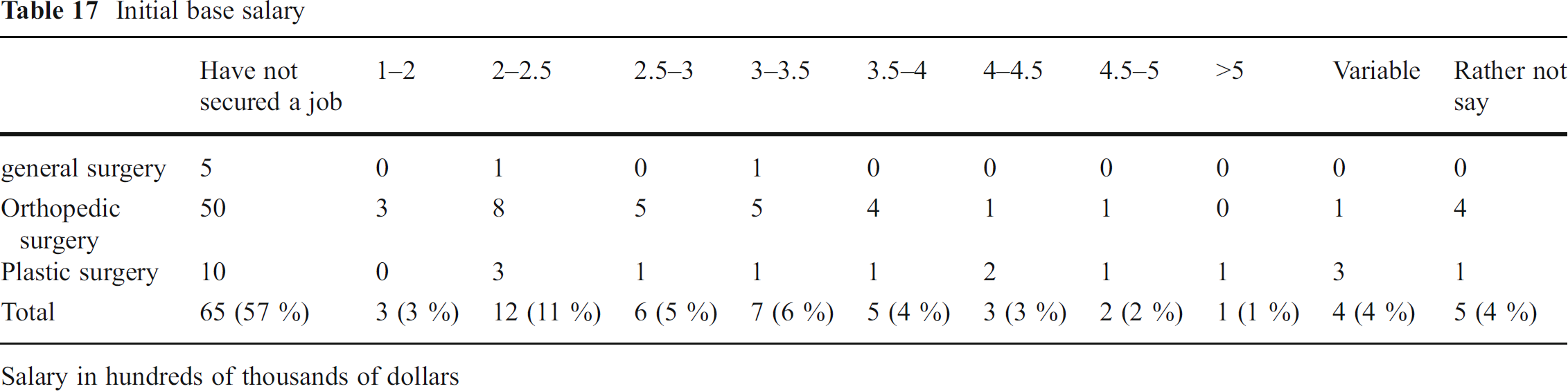
Salary in hundreds of thousands of dollars
Discussion
There is much debate about the current training model for hand surgery and whether or not to include shoulder and elbow surgery within the fellowship. While many of the respondents to our survey feel that shoulder and elbow surgery is beneficial to have exposure to during fellowship, few felt that it should be mandatory for all training models. The broadening interest in shoulder and elbow surgery most likely is fueled by the fact that the majority of the current hand surgery fellows are from orthopedic surgery and their desire to continue performing these operations once they are in practice. However, fewer than 10 % preferred a 2-year integrated fellowship that incorporates the entire upper extremity including shoulder and elbow surgery. Similarly, only 5 % of the respondents had electively chosen to pursue a second fellowship in shoulder and elbow surgery before or after attaining a hand surgery fellowship. Sixteen percent of the hand surgery fellows pursued a second fellowship including sports, shoulder, plastic, trauma, pediatric, and microsurgery thus allowing for an education tailored to the desires of the applicant and their future careers goals.
If hand surgery fellowships change from a 1-year fellowship to a mandatory 2-year upper extremity fellowship, demographics of the applicants would likely also change. This would be the first and only fellowship out of orthopedic and plastic surgery that would be a mandatory 2 years. Moreover, each year of additional training after completion of residency has a financial impact. Gaskill et al. calculated the opportunity cost to equal the average starting salary of a general orthopedist minus the average stipend for a year of fellowship in his JBJS article “The Financial Impact of Orthopaedic Fellowship Training” [3]. The opportunity cost of each year of fellowship training can be calculated by subtracting the average annual stipend for a year of fellowship from the average starting salary of a general orthopedist. The authors determined that it would require 8 years for a hand surgeon to overcome the opportunity cost of a 1-year fellowship. The number of years to overcome a 2-year fellowship was not calculated, however it might take twice as many years to make up for the lost potential earnings.
An advantage of a 2-year upper extremity fellowship is that it provides a single interview process and location for the candidates who know they want to provide the entire upper extremity scope of clinical practice after fellowship. A 2-year fellowship might offer more opportunities for elective months to allow for further specialization of training within the upper extremity. Total upper extremity training offers the clinical advantage for patients to see one physician for problems from their shoulder to their fingers. However, it is not certain that non-orthopedic residency trained fellows who complete a 2-year upper extremity fellowship would be given hospital privileges, take emergency room call, or perform such cases as reverse shoulder arthroplasty, and complex fractures of the shoulder even after completing an upper extremity fellowship when they start clinical practice. Therefore, would this additional training in shoulder and elbow surgery and an additional year of fellowship be ineffectual for plastic and general surgery trained fellows? By the same token, even with the additional year of training, would fellows whose primary residency is orthopedic or general surgery include free flaps to the upper extremity as a significant portion of their practice after only a few months of exposure in fellowship? Certainly, we cannot make such predictions based on our findings, but these questions should be addressed before considering a switch to a mandatory 2-year fellowship. Evaluation of the current hand surgery fellowships may reveal that not every program has a shoulder and elbow fellowship counterpart to be merged with, may not have adequate exposure to and numbers of cases such as brachial plexus, shoulder arthroplasty, humerus fractures, microsurgery, and congenital deformities to be considered a “complete” upper extremity fellowship program.
The total number of fellows who received the email is unclear as we had to rely on a secondary source (program coordinators) to forward many of the emails. Some programs may not have filled every position every year. Some of the email addresses the program coordinators had may not have been up to date, as we asked the program coordinators to forward the email to the 2011 and 2013 graduates who are not currently within their program. If the program coordinators emailed the survey to only their current fellows, only then the total number of respondents would be 137 out of 150 possible current fellows for a response rate of 91 %. If all of the program coordinators forwarded the email to their previous fellows, their current fellows, and their fellows matched for the upcoming year, then the response rate would be 137 out of a potential 450 responders for a 30 % response rate. Understandably, some of the program coordinators did not want to give out the personal email addresses; therefore, the exact denominator of the number of hand fellows to receive the survey is unknown. Having 137 responders makes this the largest survey of hand surgery fellows and a response rate between 30 and 91 %.
The field of hand surgery is unique in that it has residents from multiple training programs who all apply to a 1-year fellowship. The career goals of these trainees are as diverse as the field itself. The current model allows for diversity of training and the possibility of obtaining a second fellowship if desired. While additional programs providing a comprehensive 2-year upper extremity fellowships would serve to enhance current training options, this model should not be mandatory for completion of a hand surgery fellowship.