
Abstract
Clinical as well as radiologic diagnosis of infantile fibrosarcoma (IFS) is often a challenging problem due to similarities with tumors of vascular origin. Consequently, in the majority of cases, histological and immunohistochemical studies are considered gold standards for the final diagnosis. The two case reports and the review of literature discussed should increase the important features in the history and the presentation that increase the index of suspicion for IFS, as well as it highlights the important characteristics of imaging and laboratory studies that confirm its diagnosis.
Introduction
IFS is a mesenchymal malignant hypervascular tumor and the most common soft tissue sarcoma in children younger than 1 year of age [1, 2, 15, 19]. The incidence of IFS was found to be more common in the male gender [16]. It less commonly presents beyond the age of 2 years [5]. This tumor frequently gets misdiagnosed initially as a hemangioma or an arteriovenous malformation due to its vascularity and presentation [2, 19, 22]. Several literature reports discuss the similarities in differential diagnosis between vascular tumors and infantile fibrosarcoma (IFS). Boon et al. [2] and Requena et al. [19] presented cases of IFS that were initially misdiagnosed as congenital hemangiomas. On the other hand, Niekerk et al. [15] and Gulhan et al. [7] focused more on the unusual presentations of the tumor. Canale et al. [3] demonstrated magnetic resonance imaging (MRI) diagnostic features of IFS, while groups like Liu et al. [11] and Dubus et al. [6] targeted the molecular properties and their usefulness in the diagnosis of the tumor.
We present two cases that were misdiagnosed as vascular masses and managed as such until they were later diagnosed to be IFS. We also discuss the differences in history and presentation between IFS, hemangioma and arteriovenous malformations which allow the physician to identify the important features that increase the index of suspicion of IFS.
Case 1
A 2-month-old boy was transferred from another hospital to our emergency department with a lesion on the ulnar side of the dorsum of the right hand, associated with a bleeding ulcer on its apex. The tumor was round with a flat diameter of 10 cm and a rise from the skin surface about 5 cm with surrounding edema and decreased range of motion in the hand and fingers (Fig. 1). The patient received two units of packed RBCs transfusions before reaching our center.
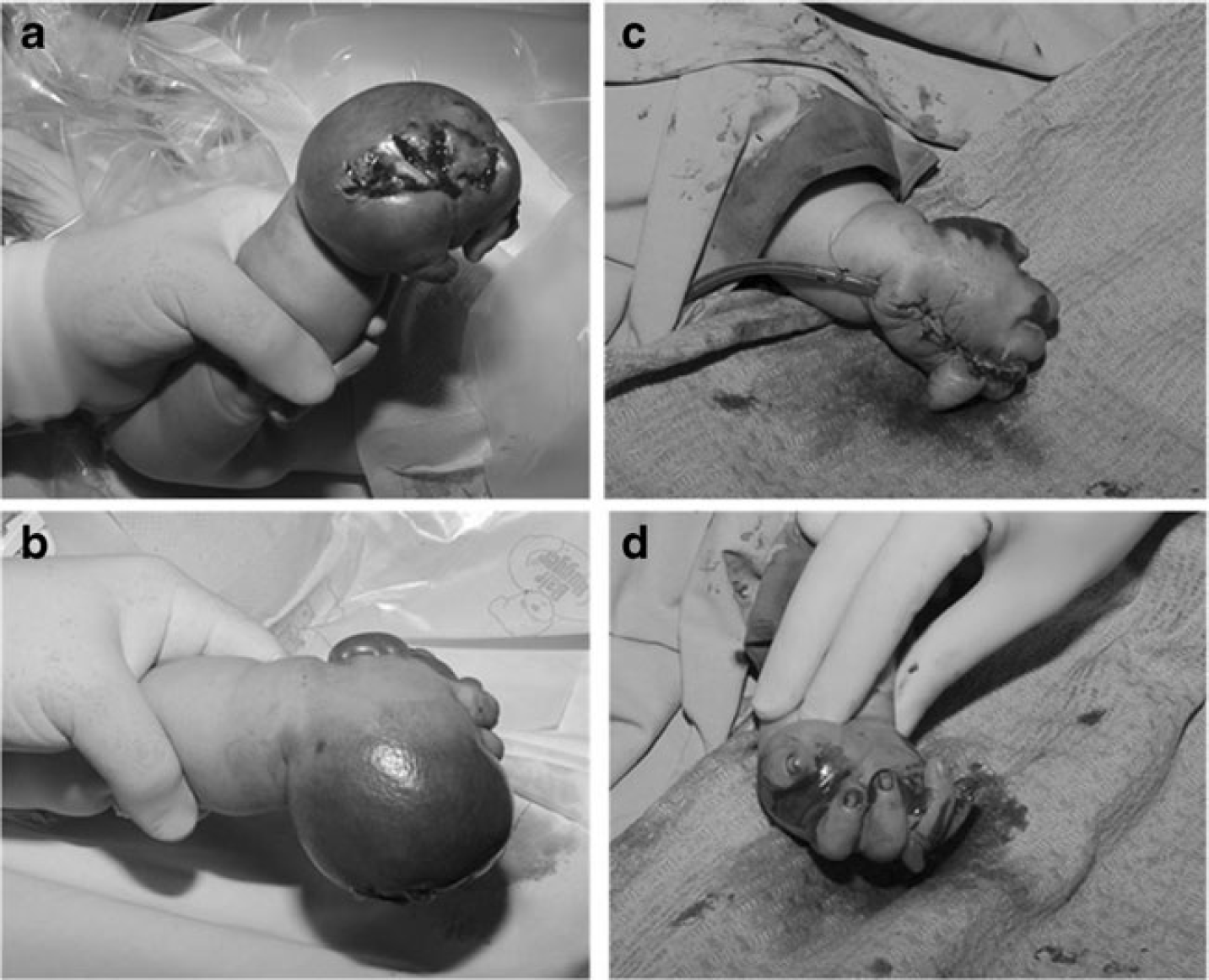
Patient 1.
However, upon presentation to the emergency room the patient was active and crying. Doppler examination of the mass revealed several enlarged arterial and venous structures. The laboratory tests showed disseminated intravascular coagulopathy (DIC) (PT patient/control = 14.2/12; PTT patient/control=47/31 and fibrinogen <1 g/l; platelets= 290,000 and D-DIMER <200 ng/ml; hemoglobin=9.7 g/dl). The lesion was thought to be an ulcerating arteriovenous malformation with external and sub-dermal bleeding. Because of the early DIC, the radiologist preferred to avoid any interventional angiography or embolization. The patient was taken to the operating room on an emergency basis. The mass was excised and the patient tolerated the procedure well (Fig. 1). The pathology examination reported a highly vascular and hemorrhagic lesion with monotonous population of oval to spindle cells growing in herringbone patterns. Numerous mitotic figures and focal hemangiopericytic-like patterns were noted. Immunohistochemistry studies were positive for vimentin, and BCL-2, and negative for myogenin, CD 31, and CD 34, which confirmed the diagnosis of IFS. The patient was then referred to the pediatric cancer center in our institution for further management. According to the parents the mass was present at birth. It appeared as a small, bluish lesion on the dorsum of the hand, which started growing rapidly at 2 weeks of age. A few days prior to presentation, the mass ulcerated and started to bleed. He had been followed up by his primary pediatrician for this mass who had done several ultrasound studies that were read as showing cavernous hemangioma.
Case 2
A 2-month-old boy who presented to the pediatric outpatient department with a left arm mass. The mass was present at birth as a 2 × 2 cm bluish elevation of the skin. It then started to grow rapidly in size until it ulcerated and started to bleed 4 days prior to presentation. Initial investigation and MRI were conducted at another hospital (Fig. 2), and the lesion was diagnosed as a vascular mass, with hemangioma and arteriovenous malformation in the differential diagnosis.
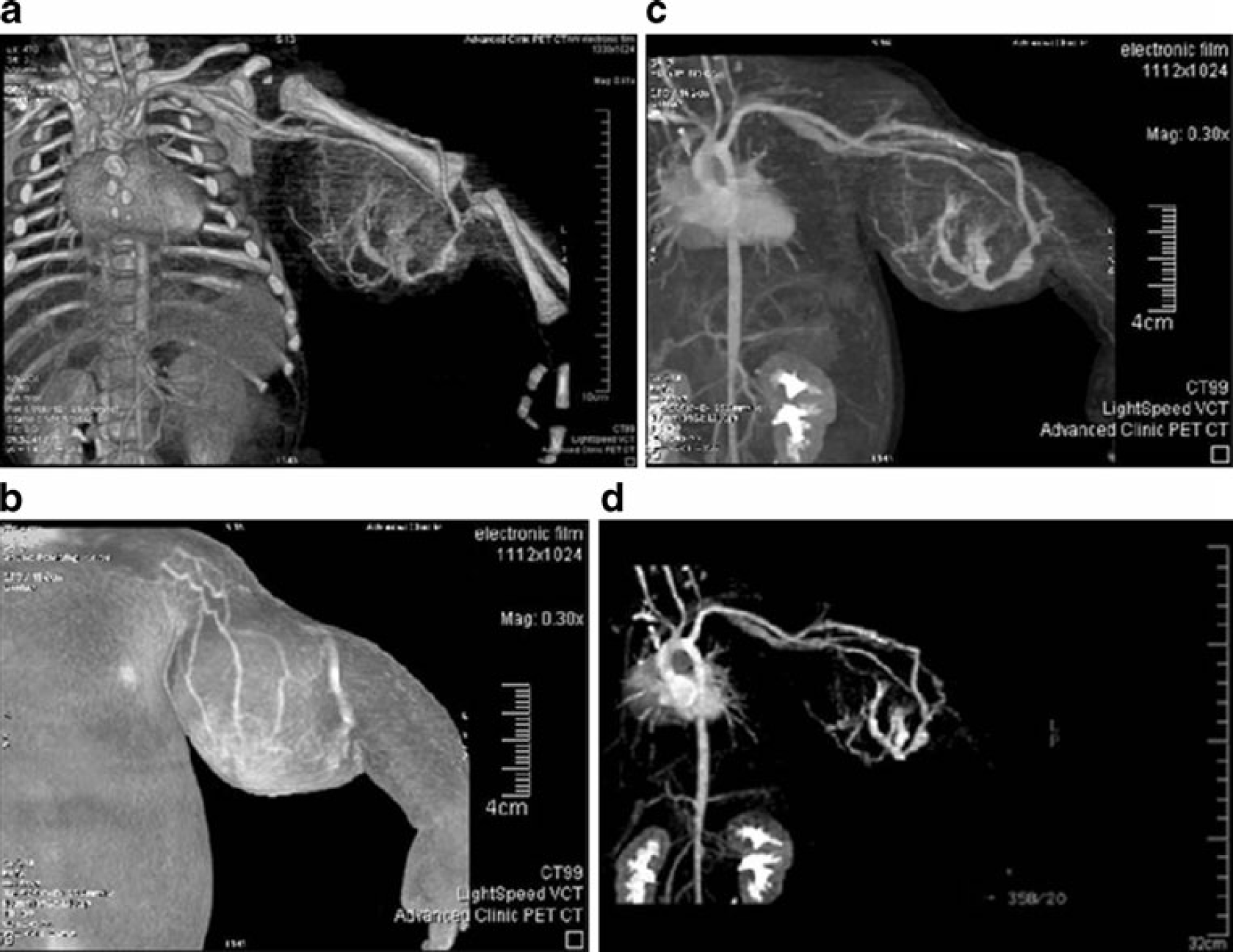
3D CT angiography.
When the mass started to ulcerate, he was referred to our center for further management. Upon presentation to our hospital, the patient was pale and hypoactive. Blood tests showed severe anemia due to the bleeding (Hgb=6.3 g/dl and Hct=19.0 %). Patient was admitted for blood transfusion and an incisional biopsy was done (Fig. 3a). Pathology reported oval to spindle cells with hypochromatic nuclei and scant cytoplasm, as well as increase in mitotic activity. Immunohistochemistry studies were positive for vimentin and negative for myogenin, CD99 and desmin, confirming the diagnosis of IFS. Chemotherapy was initiated to shrink the tumor, and later tumor excision was done (Figs. 3 and 4).
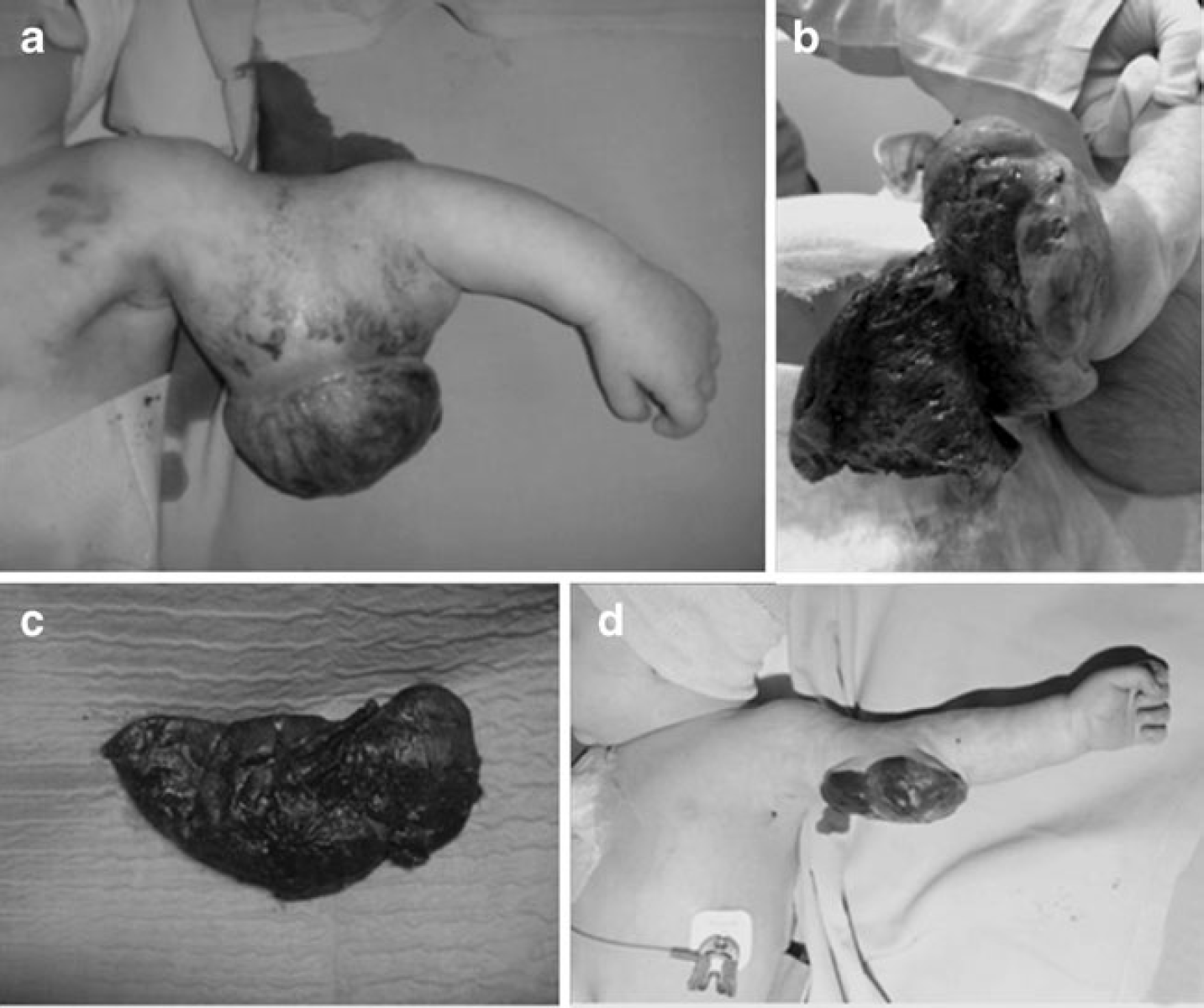
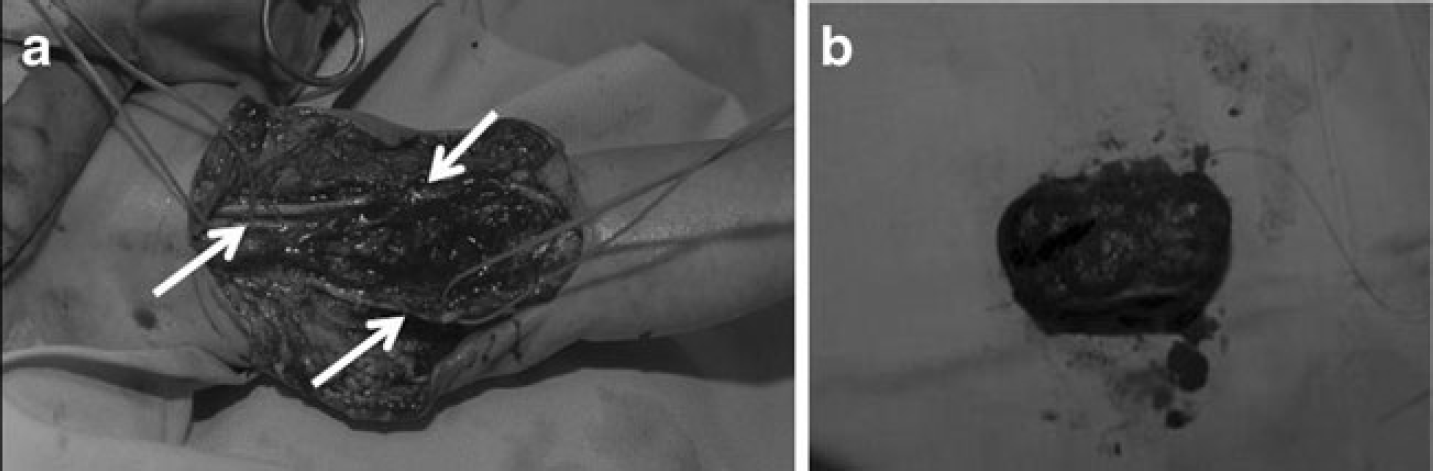
Surgical excision.
Discussion and Literature Review
IFS is also known and described in the literature in many synonyms such as congenital fibrosarcoma, juvenile fibrosarcoma, medullary fibromatosis of infancy, aggressive infantile fibromatosis, desmoplastic fibrosarcoma of infancy [5]. It is histologically indistinguishable from the adult fibrosarcoma. However, for unknown reasons, IFS has a much better prognosis, a lower rate of metastasis, and a high 10-year survival rate (89–90 %) [16] as compared to the adult patients whose 5-year survival does not exceed 50 % [16]. Fibrosarcoma is less common in infants than in adults, where it tends to present in a more central distribution [20].
IFS incidence is very low and is estimated to be five per million infants [12, 16]. It is a mesenchymal malignant hypervascular tumor and the most common soft tissue sarcoma in children younger than 1 year of age [1, 2, 15, 19] with slight male predominance [9].
Presentation after the age of 2 years is much less common [5]. It presents in about 70 % of cases in the extremities with higher predilection for the upper limbs, followed by the trunk, with the lowest incidence in the head and neck region [5, 7, 8, 10, 14, 16, 21].
The differential diagnosis of IFS includes vascular tumors like hemangiomas particularly the rapidly involuting type, lymphatic malformations, kaposiform hemangioendothelioma, hemangiopericytoma, rhabdomyosarcoma, or certain fibromatoses [3, 7, 14, 16, 19].
IFS is classified by some investigators as low-grade non-rhabdomyosarcoma with indolent behavior [10, 18]. Although this tumor is very rare, being less than 1 % of all malignancies, it makes up about 10 % of tissue sarcomas in children [1, 4, 8], and 50 % of malignant soft tissue tumors in infancy [8].
IFS can be distinguished from benign vascular tumors, such as arteriovenous malformation or hemangioma, although both can present at birth as a bluish mass or skin lesion [1, 2, 13, 16, 22]. However, certain characteristics help the clinician develop a suspicion to proceed further with investigation [2]. For example, a hemangioma is not usually present at birth [2, 13, 22]. Rather, it appears about 2 weeks postnatally, and is sometimes associated with a halo sign (whitish discoloration surrounding the bluish/reddish discoloration of the skin) [13]. Hemangiomas tend to grow rapidly within the first 1–2 years of life after which they gradually involute [13, 22]. It's estimated that 50 % of hemangiomas involute by the age of 5 years and 90 % by the age of 9 years [13]. On the other hand, an arteriovenous malformation, would be present at birth and is usually described as a bluish discoloration or small mass that grows gradually over time in a manner commensurate with the child's growth [13]. They are rarely symptomatic before puberty [13]. Because of their slow growth, arteriovenous malformations are rarely associated with ulceration or bleeding, especially without precedent trauma [13].
As noted from both our patients, IFS is usually present at birth as a bluish discoloration or small mass like an arteriovenous malformation. However, they experience a rapid growth within the first few months of life like a hemangioma. This would lead to ulceration, bleeding, and the need for frequent transfusions. There are very few reports of IFS presenting with a consumptive coagulopathy [2, 14]. Only one of our two patients presented with early DIC with slight increase in PT and PTT, low fibrinogen and normal platelets and D-dimmer levels.
On physical exam, hemangiomas tend to be compressible and soft, whereas IFS tends to be firm with violaceous shiny color [2, 22]. Although large hemangiomas can be associated with a consumptive coagulopathy (Kasabach Merritt syndrome), still there are differences from the coagulopathy associated with IFS [2, 13]. For example, in hemangiomas we expect to find profound thrombocytopenia manifesting in petechiae and ecchymoses over the lesion and surrounding it [2, 13]. In IFS, in contrast, the DIC is characterized by moderate thrombocytopenia, mild hypofibrinogenemia, and elevated levels of fibrin split products [2].
Imaging studies for IFS include MRI, CT and Angiography which can be helpful in diagnosis as well as in follow up after surgery and/or chemotherapy [3]. MRI is considered to be the technique of choice [3]. In some case reports, both CT and MRI were used and similar findings were reported [2, 8, 16, 17, 20, 21]. A study was conducted by Canale et al. [3]on six patients with IFS where the MRI features were reported to be a large well circumscribed mass, sometimes heterogeneous and septate, and exhibits an isointense T1- and hyperintense T2-weighted signals and strong enhancement with contrast. Other groups report cystic architecture and intralesional bleeding and osseous involvement [1, 2, 7, 8, 14, 16, 17, 21, 22]. Recurrence and metastasis especially to lymph nodes, bones and lungs, can also be ruled out via imaging, mostly by CT scan [10, 14, 20]. Angiography on the other hand is important to check the vascularity of the tumor and the arteries supplying it [1–3, 8, 14, 17, 20]. Angiographic characteristics of IFS include hypervascularity with abnormal caliber and hypertrophied arteries and tortuous and dilated draining veins associated with dense and heterogeneous capillary blush [2, 3, 8, 9, 17]. Some of these features may be present in hemangiomas and arterio-venous malformation whereas rapidly involuting capillary hemangioma may exhibit identical angiographic pattern [9] — hence, the confusion with a vascular tumor. None of the three techniques, however, give confirmation to a specific diagnosis of a soft tissue tumor [1–3, 8, 14, 17, 20].
The abundant blood supply of the tumor and the histological similarities to other tissue tumors and sarcomas also make it rather difficult to diagnose [16]. Nevertheless, histological studies showed some pathognomic signs for IFS including herringbone pattern with interlacing fascicles of spindled to ovoid cells [5, 19, 21]. The tumor shows cells with little nuclear pleomorphysim and abundant mitotic figures poorly infiltrated with chronic inflammatory cells mostly lymphocytes [5, 19, 21]. The ulcer associated with hemangiomas is also different from that associated with IFS. In hemangiomas, ulceration is due to invasion of the epidermal basement membrane by the tumor forming an eschar, while in IFS, the tumor ruptures and ulcerates, either superficially or deeply, secondary to intralesional bleeding and presents with a crater of clots [1, 2, 8, 14, 19, 22].
IFS also has important immunohistochemical features that might help in the diagnosis of the tumor. Vimentin, for example, which is also established in the adult subtype, is found in 100 % of cases, while other markers like smooth muscle actin, S-100 protein, CD34, CD57 are not as common [5, 19, 22].
Recently, cytogenetic and chromosomal abnormalities have been extensively reported in the literature. ETV6/NTRK3 (also known as TEL/TRKC) fusion is considered characteristic and consistently found in immunohistochemistry studies in IFS [6, 11, 12, 16, 19, 21, 22]. Trisomies 8, 11 and 20 are also associated with IFS; however, these abnormalities are neither as common nor as specific as TEL/TRKC fusion in IFS [1, 5–7, 12, 14, 22].
Conclusion
When a mass or discoloration in an infant is present at birth (similar to an arteriovenous malformation) yet grows very rapidly and ulcerates (similar to a hemangioma), the diagnosis of an IFS should be highly considered.
Footnotes
The authors declare that they have no conflict of interest.