
Abstract
Introduction
Glomus tumors originating from the glomus body in the dermis account for less than 5% of all diagnosed tumors in the hand and almost all are benign. 4 Malignant glomus tumors—also termed glomangiosarcomas—are exceedingly rare2,3 and are more common in the lower extremity. There are only 6 reports of malignant glomus tumors in the hand—ranging from 5 mm to 4.5 cm in size.3,5-9 Re-classification of glomus tumors has suggested that a diagnosis of malignant should be reserved for tumors with a risk of metastasis, which seems to correlate with a deeper location, size greater than 2 cm, atypical mitotic figures equal or greater than 5 mitotic figures per 50 high-power field, and moderate to high nuclear grade. 1 We describe the largest malignant glomus tumor of the hand ever reported.
Case Report
A 59-year-old right-handed female visiting her family from Russia presented with over a 40-year history of extreme tenderness and hypersensitivity in the palm of her left hand. She reported that her symptoms started after her hand was stepped on by a cleated boot. The patient had undergone surgical exploration approximately 5 years after the injury, but no details were available. Her symptoms had progressively increased in severity, and she constantly protected her hand by elevating it, avoiding all external contact, and showed extreme reluctance to any examination.
Examination revealed disuse atrophy of the hand. The patient could hardly tolerate any palpation of her palm; the worst tenderness was over the palmar aspect of the index, middle, and ring finger metacarpals, but it also extended dorsally between the index and ring finger metacarpals. There was no obvious protruding mass in the palm and no ulcerations or other skin changes. Subjective sensation to light touch was normal in the finger tips, but there was severe stiffness and limited motion of the fingers. No lymphadenopathy was palpable at the elbow or axilla.
Magnetic resonance imaging revealed a 5.0 × 4.9 × 1.5 cm mass in the palm, palmar to the index and middle finger metacarpals, and extending into the thenar eminence and abutting the first and second palmar interosseous muscles radial and ulnar to the middle finger metacarpal (see Figures 1 and 2). The distal contents of the carpal tunnel were displaced ulnarly, and the flexor tendons were displaced palmarly. The mass was felt to be a giant lipoma or less likely a giant cell tumor of tendon sheath or a schwannoma.
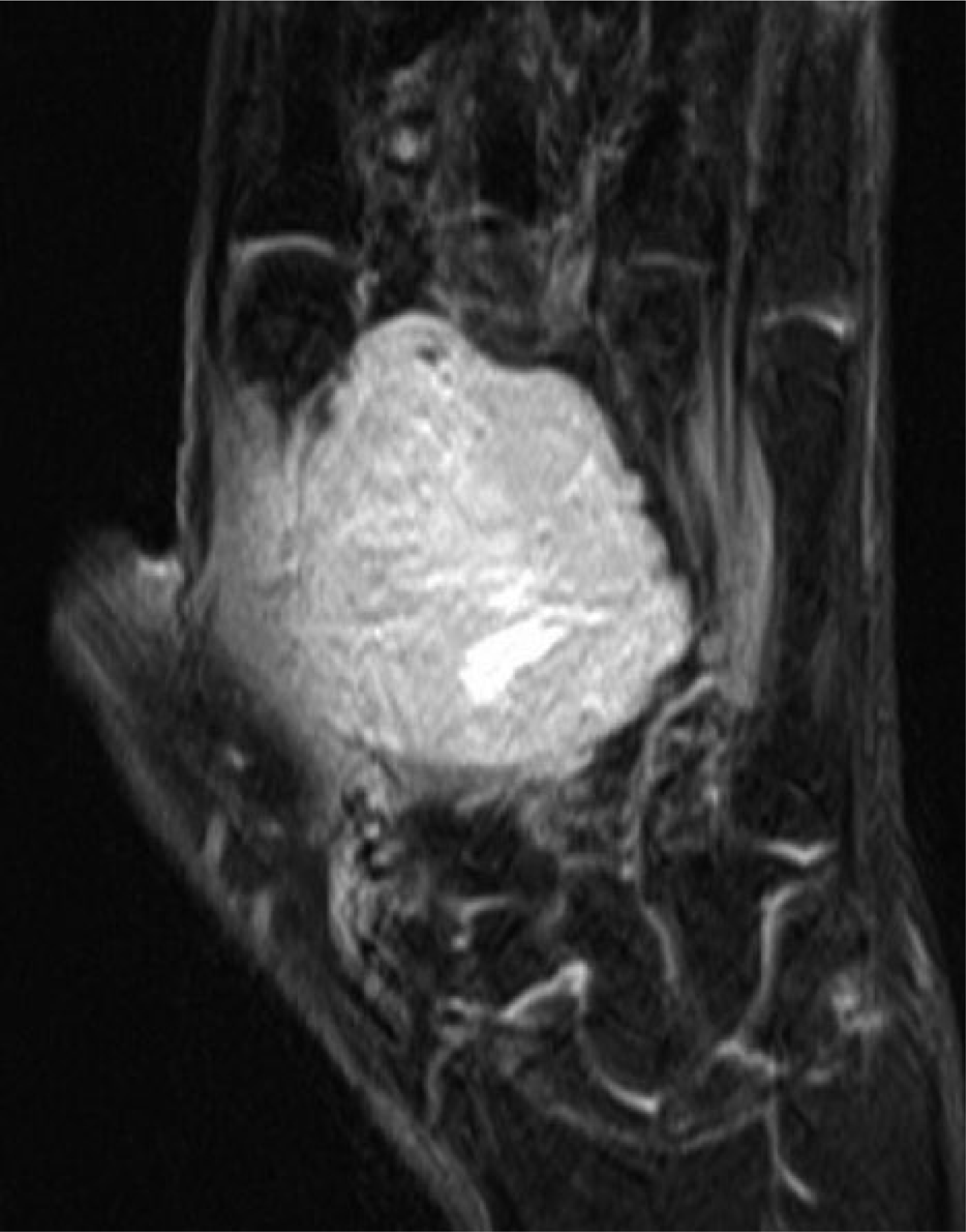
Magnetic resonance imaging, main body of tumor.

Magnetic resonance imaging, extension of tumor into intercarpal spaces.
The mass was explored through an inverted J-shaped incision extending distally from the carpal tunnel over the index and middle finger metacarpals. The median nerve and its branches were identified and retracted, along with the flexor tendons, which were not involved by the mass. A very large, amorphous, fragile, tan-colored mass was identified deep to these structures, without a well-defined capsule, infiltrating the thenar muscles and first and second palmar interosseous muscles (see Figure 3).
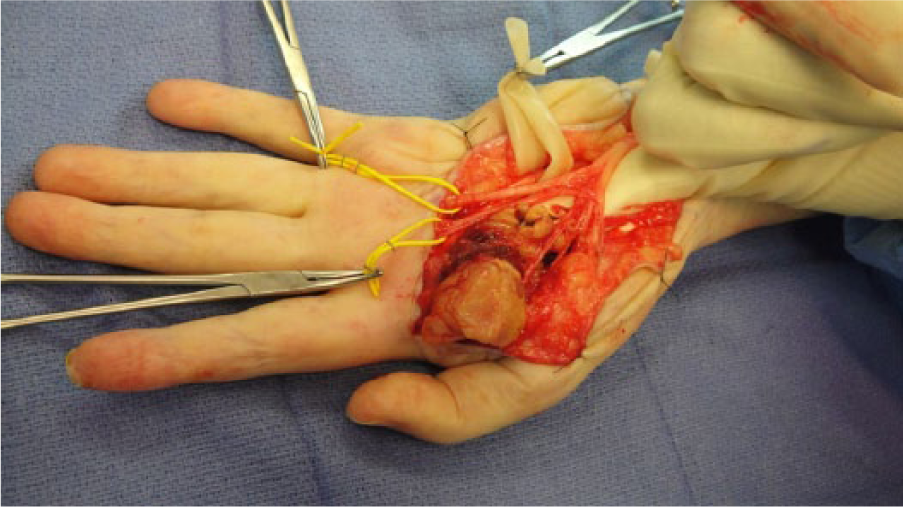
Intraoperative photo of tumor in-situ.
A frozen section was consistent with a glomus tumor, and a wide local resection was performed. Final pathological review was reported as an epithelioid tumor indeterminate for malignancy, but failed to classify the tumor definitively. Histology revealed solid sheets of cells as well as cells arranged in vague cords, with low vascular density, minimal cytologic atypia, minimal necrosis, and only one mitosis per 10 high-power fields. Immunohistochemistry revealed heavy staining for caldesmon and patchy staining for smooth muscle actin (see Figure 4). Diagnosis by the Department of Pathology at the Mayo Clinic was most consistent with a malignant glomus tumor. The malignant portion of the tumor was negative for smooth muscle actin, desmin, type IV collagen, cytokeratin, S100 protein and CD 34, but IN11 expression was retained. A small focus of benign appearing glomus tumor was positive for smooth muscle actin and type IV collagen.
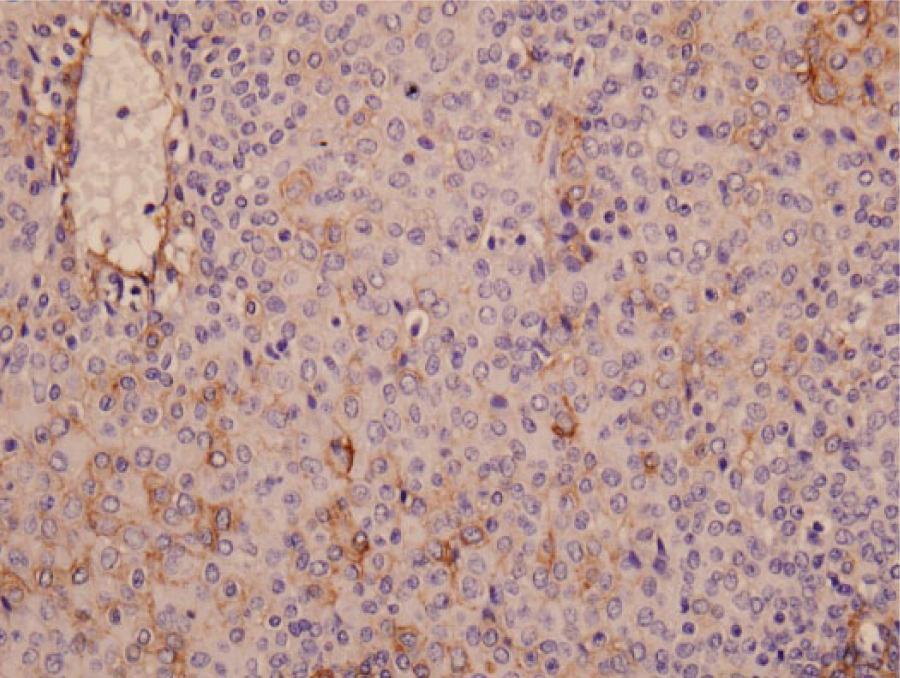
Immunohistochemical staining of malignant glomus tumor.
Postoperatively, her pain improved dramatically; she kept her hand at her side and could even massage the incision herself. There was no change in sensation in the median and ulnar nerve distribution. There was improved flexion of the ring and small fingers to touch the distal palmar crease, but she continued to have stiffness of the index and middle fingers. She had had no systemic symptoms over the previous 40 years, such as chronic cough or liver failure to suggest a metastasis, and chest X-ray and liver function tests were normal in a metastatic workup. It is unclear whether the resected lesion was present for the entire history of her symptoms, or was present for a shorter more recent period of time. Four years postoperatively, she has no signs of local recurrence or metastasis.
Discussion
Malignant glomus tumors, or glomangiosarcomas, have been reported almost exclusively in the pathology and dermatology literature. However, hand surgeons should be aware of the possible diagnosis and metastatic risk of a malignant glomus tumor in the hand.
There are only 6 previous reports of malignant glomus tumors in the hand.3,5-9 Khoury et al reported a 2.8-cm glomangiosarcoma of the thumb that metastasized to the lungs in a 48-year-old woman. 3 Oh et al described a malignant glomus tumor in a 33-year-old pregnant woman with an 18-year history of an enlarging 2-cm mass on her middle finger that grew to 4.5 cm following delivery. 5 This was treated with ray resection and is the largest previously reported glomangiosarcoma. Terada et al reported a 2.5-cm malignant glomus tumor resected from the palm, which recurred locally and was re-excised. 8 A glomus tumor of the thumb with classic symptoms was reported by Wetherington et al in a 30-year-old woman. 9 Excision revealed a tumor 0.5 cm in size that was thought to be malignant on immunohistochemistry. Park et al reported a 74-year-old woman with a 1.5-cm ulcerating mass on her palm that was determined to be a glomangiosarcoma with no evidence of metastasis. 6 Finally, Perez de la Fuente et al described a 0.5-cm glomangiosarcoma arising in a glomus tumor in the hypothenar eminence in a 36-year-old woman. 7
Wide local excision has traditionally been recommended as adequate treatment, as most malignant glomus tumors are considered to be unlikely to metastasize. 1 The pattern of metastatic spread is not well understood and metastases have been seen both in lymph nodes and hematogenously. The most recent classification scheme pertaining to glomus tumors suggests that malignant characterization should be reserved for tumors with a risk of metastasis, and suggests a correlation with deep location, size greater than 2 cm, atypical mitotic figures equal or greater than 5 mitotic figures per 50 high-power field, and moderate to high nuclear grade. Based on these criteria, the incidence of metastasis was 38% in a series of 52 malignant glomus tumors. Stratifying these patients with regard to their risk of metastasis, based on the size and depth and histological characteristics of the tumor, may now be possible. 1
Malignant glomus tumors can remain undiagnosed or incorrectly diagnosed for years, and even when excised, can present diagnostic challenges for histological conformation.
Footnotes
Acknowledgements
The authors would like to thank William Wu, MD, for providing pathology slides.
Ethical Approval
Ethical approval not needed; no animals or live patients participated in this case report.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained when necessary.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.