
Abstract
This paper analyzes whether a black-white racial wage differential exists in the nursing labor market in the US. Despite claims of a nursing shortage, little examination of whether racial inequalities in the labor market might contribute to this purported shortage has occurred. Possible explanations for black-white differences in RN compensation include racial differences in: occupation; returns to skills; metropolitan residency; union membership. Regression analysis on wages for registered nurses (RNs) was conducted. Findings suggest a wage penalty for nonunion black nurses compared to non-union white nurses as well as the absence of a racial wage differential for union nurses.
Introduction
This paper analyzes the labor market for registered nurses (RNs) in the United States (US) to determine if Black nurses experience a wage penalty relative to White nurses. This is important because nursing and teaching represent two relatively well paid professional occupations with large representations of African American females. Some research argues that a nursing shortage exists (Bergmann 2006; Lovell 2006; Seago et al. 2001). However, few studies have examined the prospects for African American nurses to help alleviate the purported shortage. An impediment to these prospects could be real or perceived racial inequalities in the labor market. Some researchers argue that healthcare employers possess monopsony power (Bergmann 2006; Yett 1975). Monopsony power may allow them to indulge in exercising racial preferences; in light of purported shortages, this would represent a market failure. Others argue that unions may offer countervailing power as the result of imposing standard wages based on seniority that could prevent this situation from occurring in occupations such as nursing (Schmitt 2008).
Research exists that suggests the presence of a black-white wage gap in nursing. Buhr (2010) found immigrant nurses from Africa and the Caribbean received a 9% wage penalty in Canada. Scott (2008) contends that Black nurses earn less than White nurses in New York. Possible explanations for black-white differences in nurses’ pay include racial differences in: occupation; returns to skills; metropolitan residency; union membership. This study addresses the issue by performing regression analysis on the wages of RNs, which allows for a more focused analysis of the returns Black and White nurses receive for their characteristics.
Historical overview of Black and White nurses in the United States
Mosley (1995) suggests that segregation and discrimination has existed in nursing education and employment across the US since the late 19th century and includes: limited access to practice opportunities and learning institutions; separate state boards of nursing examinations for Black graduate nurses; membership policies that almost totally denied admission to Black nurses to professional nursing organizations. From 1879 to 1964, Black nurses were denied membership in at least some state nursing organizations (Campinha-Bacote 1988). Moreover, 20 years after the National Association of Colored Graduate Nurses (NACGN) voluntarily disbanded after full acceptance of their members by the American Nurses’ Association (ANA) in 1951, black nurses formed the National Black Nurses’ Association (NBNA). The history of Black nurses suggests that the formation of the NBNA was a direct response to the perceived neglect of African Americans by mainstream healthcare institutions and professionals. In fact, Hines argues that Black nurses and the masses of Black people have had little to gain under a separate and unequal healthcare system that was not their choice or creation, and an institution such as NBNA was a necessary weapon against the ill effects of racism in nursing (Hines 1989).
Black and White nurses in the current U.S. nursing labor market
Keels (2004) cites US Department of Health and Human Services (DHHS) data that project a nearly 30% shortage in registered nurses by 2020, compared to a 6% shortage in 2002. This purported shortage makes it perplexing to understand why Blacks, who have historically had higher rates of unemployment, have not flocked to educational programs to qualify for positions in nursing. Data from the 2000 census and 2002 National Sample Survey of RNs analyzed by Mingo (2008) suggests that Black RNs account for less than 5% of the US nurse population, while Blacks accounted for more than 12% of the US population.
In the context of the current labor market for nurses in the US, it is important to determine whether groups that are underrepresented in the nursing profession can be persuaded to invest the time and resources necessary to become nurses. Real or perceived inequalities in this labor market could hamper efforts to simultaneously diversify the nursing workforce and reduce the projected shortages. Potential inequalities could be deduced through an analysis of the comparative wages of Black and White nurses. Gary Becker (1957) argued that competition would help to mitigate the ability of firms to indulge in the types of racial preferences that could lead to differential wages among Black and White nurses. However, some economics research suggests that healthcare employers may possess some level of monopsony power (Bergmann 2006; Yett 1975). This sort of monopsony power might, in fact, allow these employers to indulge in racial preferences. If monopsonistic healthcare employers are able to indulge in racial preferences, this could result in Black nurses in the US facing a wage penalty relative to their White counterparts similar to the 9% penalty received by nurses from Africa and the Caribbean in Canadian nursing labor markets (Buhr 2010). This could also help to explain why Scott (2008) argues that Black nurses in New York make less than White nurses. Of course, it must be noted that racial differences in the likelihood of residing in metropolitan areas or belonging to labor unions could serve to explain some of the racial wage differentials in nursing.
Data and earnings model
Individual worker information is taken from 1994 to 2006 Current Population Survey-Outgoing Rotation Group (CPS-ORG) files to examine wage compensation patterns of Black and White nurses. Information on pension and health care coverage, however, is taken from 1996 to 2006 March CPS files. The population sample taken from the ORG files is stacked over time rather than reported as a true panel data set. Therefore, each observation presents information for a unique individual nurse for each observation year. The information utilized was limited to individual respondents who self-identified as Black or White and were employed in clinics, hospitals, nursing homes, and other healthcare offices. These nurses reported information on their usual weekly earnings, usual hours worked, union status, and a set of demographic characteristics.
Equation 1 listed below is estimated to analyze the black-white wage differential of nurses employed in the US. Given the possibility of union endogeneity, a Heckman-Lee two-step technique is used to correct for selectivity bias when estimating this wage equation.

Where ‘j’ indexes individual workers and the dependent variable is the log of the jth worker's real hourly wages. Hourly wage rates are calculated by taking the ratio of individual workers’ weekly earnings and weekly hours worked. Matrix Z consists of a set of worker residency and worker profile explanatory variables including residency dummies for US geographic regions and metropolitan residency status. Worker profile measures are dummies depicting workers': marital status; gender; foreign birth status; full-time employment; health care employment sector; public sector employment; educational attainment; age and age-squared. The variable T is a time trend that is included to account for possible changes in the wage determination process over time. The variable Black is a dummy equaling one if the individual has self-identified as having African ancestry and has a value of zero otherwise. The variable Union is a dummy equaling one if the individual belongs to a union. The final variable presented in Eq. 1 is the inverse Mills ratio, denoted as λ, which is calculated as the ratio of the standard normal probability density and the standard normal cumulative density for individual nurses. The estimated coefficient on this variable depicts the influence of differential union-nonunion unobserved worker characteristics on wages.
Coefficients that are of special interest to this study are β3, β4, and β3+β5. β3 measures the Black-White log wage differential for non-union nurses employed in the US. β4 measures the union and non-union log wage differential for White nurses in the US. The sum of β3+β5 measures the Black-White log wage differential for union nurses. These estimated coefficients are converted to percentage differentials by using the formula (∊β-1)×100. Interpreting findings on these coefficients, however, may be problematic because estimating an equation specified with a log transformed dependent variable could introduce heteroscedasticity (Ai and Norton 2006). Therefore, Basu's semi-parametric derivative estimator was used to compute consistent estimates of β3, β4 and, β5 (Basu 2005).
Descriptive statistics
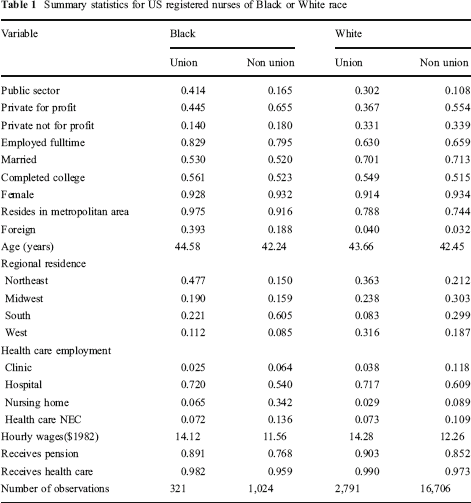
Summary statistics for Black and White registered nurses appear in Table 1. Compared to their White counterparts, Black nurses are more likely to: belong to labor unions; work in the public or the private for profit sectors; be employed fulltime; have a college degree; have urban residency; be foreign born; have Northeast or South regional residency; be employed in nursing homes and health care nec's. Moreover, compared to their White counterparts, Black nurses are less likely to: work in the private not for profit sector; be married; have Midwest or West regional residency; be employed in clinics or hospitals; receive employer sponsored pension or health care coverage. Black and White registered nurses are equally likely to be female, and they are approximately the same mean age. Black nurses ($12.17) earned less on average than White nurses ($12.54): among unionized nurses, Black nurses earned $0.16 less per hour than White nurses; among non union nurses, Black nurses earned $0.70 less per hour than White nurses.
Summary statistics for US registered nurses of Black or White race
Estimation results
Estimates of Eq. 1 appear in Table 2: parsimonious results are in column (i); results from a more complete specification without the black-union interaction variable are in column (ii); results for the full specification are in column (iii). T-statistics are in parentheses.
Log hourly earnings regression results
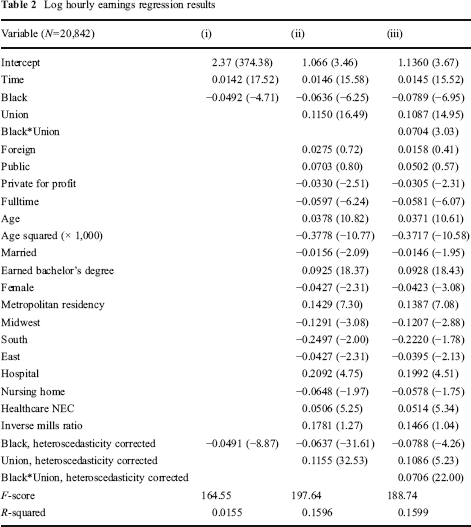
The estimated coefficients on the Black dummy variable in columns (i) and (ii) indicate a 4.8% wage penalty for Black nurses when control variables are not included in the specification and a 6.12% penalty under a more complete set of controls. The estimated coefficient for the Black dummy variable in column (iii) suggests Black non-union nurses receive a wage penalty of 7.58% compared to their White non-union counterparts after including the complete set of control variables. The estimated coefficient for the variable Union in column (ii) indicates that nurses in unions earn a wage premium of 12.18% compared to non-union nurses. Moreover, the estimated coefficient for the Union variable in column (iii) indicates that among White nurses, nurses in unions earn a wage premium of 11.48% compared to non-union nurses. The sum of estimated coefficients for the Black dummy variable and the Black x Union interaction variable in column (iii) indicates a negligible 0.85% Black-White wage penalty among union nurses in the wage equation with the full set of control variables. These results suggest that union membership may mitigate monopsonistic employers’ ability to indulge in racial preferences. Also, it must be noted that correcting for heteroscedasticity did not appreciably change the results in either specification.
Conclusion
Policymakers continue to search for solutions to a purported persistent nurse shortage. One solution may be greater utilization of Black nurses. Nursing has historically been held in high esteem by Black communities as a viable professional career option for women (Hines 1989). The likelihood of Black women investing the time and resources needed to become registered nurses; however, may be diminished by perceptions of a labor market where healthcare employers may indulge in racial preferences. This suggests the possibility of a degree of market failure in light of the purported nurse shortage. Wage regression results in this study suggest a wage penalty for Black non-union nurses relative to White non-union nurses, but the absence of a racial wage differential between Black union nurses and White union nurses. These results are consistent with findings from non-US developed countries and the notion that unions can help to mitigate monopsonistic healthcare employers’ ability to indulge in racial preferences.