
Abstract
Objective: Prescription drug misuse (PDM) is an emerging epidemic in the United States. This study examines the prevalence and correlates of PDM among homeless men. Homeless men experience higher risk for substance misuse and associated health problems and are particularly vulnerable to PDM and its negative health consequences. Methods: Participants were a representative probability sample of 305 heterosexually active homeless men interviewed from meal programs in the Skid Row region of Los Angeles. Interviews assessed demographics, substance use, mental health, and social networks. Logistic regression examined correlates of PDM. Results: Twenty-six percent of the study population reported PDM in the past year. PDM was more likely among homeless men suffering from posttraumatic stress disorder (PTSD) (odds ratio [OR] = 2.41, 95% confidence interval [CI]: 1.03–5.61) and among those with more substance-using social network members (OR = 1.07, 95% CI: 1.01–1.14). Decreased PDM was associated with good health (OR = 0.34, 95% CI: 0.16–0.75). Conclusions: The prevalence of PDM is higher among the homeless men in this study than in the general population. Correlates of PDM included PTSD and poor health, suggesting that homeless men may use PDM to self-medicate. PDM was also associated with increased substance-using social network alters. Physical and mental health and social context are important aspects to consider in prevention efforts to reduce PDM among homeless men.
Introduction
The prevalence of prescription drug misuse (PDM) is on the rise in the United States (1). In 2010, approximately 2.7% of the US population reported past-month nonmedical use of prescription opioid analgesics, sedatives, tranquilizers, or stimulants, making PDM second only to marijuana in general population prevalence (2). The misuse of prescription medication can have serious health consequences, including addiction, seizures, respiratory depression, and death (3). Nationally, emergency department visits related to the nonmedical use of prescription medication increased 81% between 2004 and 2008, with almost 1 million PDM-related medical emergencies reported in 2008 (4). Comparatively little research has been done to investigate correlates of the serious and expanding problem of PDM in the United States, relative to research addressing alcohol and other drug use.
This study examines the correlates of prescription drug misuse among homeless men; to our knowledge, no research has yet examined PDM among homeless persons. This is an important population to study, as conditions associated with homelessness can exacerbate the negative consequences of substance misuse (5) and research has found that men are at greater risk of substance use problems than women (6). Homeless persons are more likely than the housed population to experience acute and chronic illness (7), including substance misuse and mental health problems (8, 9, 10). Apart from our knowledge that certain mental health and social network characteristics are associated with use of alcohol, marijuana, and crack among homeless men (11), there is little previous research involving homeless men to help us understand correlates of PDM. Increased vulnerability associated with the physical and social contexts of homeless men's lives may further complicate the misuse of prescription drugs, including the misrepresentation of veterans among the homeless; nearly 11% of the homeless population in the United States are military veterans (12), though this figure does not take into account gender differences and the proportion of homeless men who are veterans is likely higher. The lack of research into PDM among homeless men may be associated with poor understanding of the health risks associated with substance use in this population. Further research into the correlates of PDM may aid prevention and treatment efforts for this particularly vulnerable group of individuals.
General physical health status and symptoms of illness may be associated with PDM. One potential explanation is that those in poor health are more likely to have contact with medical providers and thus have greater access to prescription medications, which they may then use in ways not prescribed. Access to medical services may therefore also be associated with PDM. Alternatively, PDM use among those in poor health may be the result of self-medicating for pain or other health concerns. An increase in reported physical symptoms of poor health was associated with PDM among adolescent male arrestees (13), and chronic pain has been associated with misusing prescriptions among veterans (14). The risk of PDM was also much higher among Canadian adults who reported their occupational status as “disabled” (15).
Homeless persons experience depression and PTSD at higher rates than the general population (9). PDM has been associated with mental health problems: it is more likely among those with major depression in a national sample of college women (16), among adolescents (17), and among veterans (14). PDM has also been associated with symptoms of posttraumatic stress disorder (PTSD) among low-income women (18), and with panic and anxiety among rural substance users (19). PTSD has also been associated with self-medicating substance use among veterans (20), and veterans are overrepresented among homeless populations. As the misuse of prescription drugs is likely to co-occur with mental health problems, and mental health problems are more prevalent among homeless populations, PDM is expected to be higher among homeless (vs. housed) men.
Having drug and alcohol users in an individual's social network (individuals are called social network “alters”) may be associated with increased substance use; alters may provide substances or paraphernalia, or communicate social norms supportive of drug use (21, 22, 23, 24). The association between substance-using alters and individual substance use has been supported in previous research among homeless populations, though PDM has not yet received research attention in this context. More alcohol and drug users in homeless women's personal networks was associated with heavy drinking and drug use (25) and having peers who regularly use drugs was associated with increased severity of substance use among homeless young adults (26).
This study examines the correlates of prescription drug misuse among homeless men. To our knowledge, PDM has not been previously studied in homeless populations. We hypothesize that perceived good health will be inversely associated with PDM. We also hypothesize that PDM will be more likely among men with more drug- or alcohol-using social network alters and among those who experience mental health problems (symptoms of PTSD and depression).
Methods
Participants in this study were 305 homeless men randomly sampled and interviewed in 13 meal programs in the Skid Row area of Los Angeles. This area is home to the highest concentration of homeless persons in Los Angeles County. Men were eligible if they were at least age 18, could complete an interview in English, had experienced homelessness in the past 12 months (i.e., stayed at least 1 night in a place such as a shelter, abandoned building, voucher hotel, vehicle, or outdoors because they didn't have a home to stay in), and provided informed consent. This sample was collected as part of a larger study of heterosexual risk behavior, and thus all participants must also have reported vaginal or anal sex with a female partner in the past 6 months to be eligible. For the data collection, computer-assisted personal interviews were conducted with the software EgoWeb (http://egoweb.github.com), an open source software designed specifically for the collection, analysis, and visualization of personal network data. Of the 338 men who screened eligible for the study, 320 men were interviewed (18 refusals). Of these 320, 4 named fewer than 20 network members (alters), 7 were partial completes/break-offs (when interviews could not be completed because the respondent had to leave suddenly, refused to finish the interview, or otherwise did not fully complete the interview process), and 4 were later found to be repeaters. The final sample size was 305, for a completion rate of 91% (305/334). Men were paid $30 for participation in the interview, which lasted on average 83 minutes. The research protocol was approved by the institutional review boards of the University of Southern California and the RAND Corporation.
To obtain a representative sample of heterosexually active homeless men from the Skid Row area of Los Angeles, we implemented a probability sample of men recruited from meal lines in the area. The list of operating meal lines in Skid Row was developed using existing directories of services for homeless individuals and performing interviews with services providers. Our final list contained 13 meal lines: 5 breakfasts, 4 lunches, and 4 dinners offered by 5 different organizations. Each of the meal lines was extensively investigated to obtain an estimate of the average number of men served daily. This information was used to assign an overall quota of completes to each site, approximately proportional to the size of the meal line. We then drew a probability sample of homeless men from the 13 distinct meal lines. When the assigned quota could not be achieved in a single visit, the quota was divided approximately equally across the number of visits for each meal line. The interview team randomly selected potential recruits for screening by their position in line using statistician-generated random number tables. Tables were generated such that the site daily quota could be achieved before the meal line was exhausted. Once the field director selected a potential recruit, an interviewer would wait for him to finish his meal before screening him. Interviews were conducted in any area that afforded privacy: these included corners in dining rooms, chapels, hallways, empty rooms, and in one case, the sidewalk.
The adopted sample design deviates from a proportionate-to-size stratified random sample because of changes in sampling rates during the fielding period, differential response rates of men across meal lines, and variability in how frequently men use meal lines. This last factor means that some men are more likely to be included in the sample. We accounted for the differential frequency of using meal lines by asking respondents how often they had breakfast, lunch, and dinner at a meal line in the Skid Row area in the past 30 days, and how much of the past 6 months they had been homeless. This information was used to develop and implement sampling weights to correct for departures from a proportionate-to-size stratified random sample and potential bias due to differential inclusion probabilities (27).
Measures
Prescription drug misuse
Prescription drug misuse was assessed with an item from the Composite International Diagnostic Interview short-form (CIDI-SF) (28). Men were asked to consider use of prescription medication “on their own,” that is, “without a doctor's prescription, in larger amounts than prescribed, or for a longer period than prescribed.” With this definition in mind, men were asked whether they had used prescription pain relievers, tranquilizers, sedatives, or barbiturates on their own during the past 12 months. Respondents were reminded that the interviewers were not interested in over-the-counter drugs that can be bought in drug stores or grocery stores without a prescription.
Background characteristics
Control measures included background characteristics that we have utilized in previous studies (11, 25): age, race/ethnicity, education (having at least a high school education or General Equivalency Diploma [GED]), having been in jail, prison, or on parole in the prior 6 months, and being a military veteran.
Health
General health status was measured by asking men: In general, would you say your health is: 1, Excellent; 2, Very good; 3, Good; 4, Fair; or 5, Poor. A single indicator of “good health” was created to indicate a response of 3 or more to this question. This item has been used in general population and homeless surveys as a valid indicator of general health (29, 30, 31). Health service utilization was measured by asking men whether they had accessed medical/dental services in the Skid Row area in the prior 30 days (32).
Mental health
Past 12-month depressive disorder (Yes/No) was measured using a 3-item screening instrument (33) that was tested on community residents, medical patients, and mental health patients, and that has demonstrated sensitivity between 83% and 94% and specificity of 90% in these samples (34). Items from this instrument were drawn from the Diagnostic Interview Schedule (35) and the Center for Epidemiologic Studies Depression Scale (CES-D) (36). This screening instrument has been used in several recent studies with homeless persons (37, 38).
PTSD was measured with the Primary Care PTSD Screen, a 4-item screener originally designed for use in primary care settings (39). The 4 items reflect 4 underlying factors specific to PTSD: reexperiencing, numbing, avoidance, and hyperarousal. Respondents in this study are defined as screening positive for PTSD if they answer “Yes” to any 3 of 4 items. A cut point of 3 on the Primary Care PTSD Screen has been shown to maximize sensitivity and specificity of this measure in primary care patients (40). In a primary care setting, persons identified as having at least 3 of the 4 PTSD symptoms would then be administered a structured interview to formally diagnose PTSD (39).
Social network characteristics
We used established procedures for conducting personal network interviews (41, 42) and our experiences in a prior study of homeless women (37,43) to develop the instrument. We asked respondents to provide the first names of 20 individuals (called “alters”) that they knew, who knew them, and that they had contact with sometime during the past 6 months (alters had to be at least 18 years or older). Contact could be face-to-face, by phone, by mail, or through the Internet. We constrained network size to be the same across respondents to maximize comparability of network structure measures (44). Twenty alters has been shown to capture structural and compositional variability present in personal networks (45); 4 men who were not able to name 20 alters were excluded from the sample to maintain comparability across cases.
In this study, we focused specifically on social network alters who use alcohol or drugs. Respondents were asked which of their social network alters were likely to use drugs or drink alcohol to intoxication, and a measure was created indicating the total number of these alters in the network.
Analysis
Logistic regression models were used to predict the odds of misusing prescription medication in the past year. Analyses were conducted in Stata 9.2 (StataCorp, College Station, TX). Each predictor associated bivariately at P < .10 with PDM was retained in the multivariate model; this stepwise model building technique is utilized to create a parsimonious multivariable model out of a larger group of potential predictors (46). Individual demographic characteristics were retained in the multivariate model as controls: age, race/ethnicity, education, jail/prison/parole, and military service.
Results
Sample Characteristics
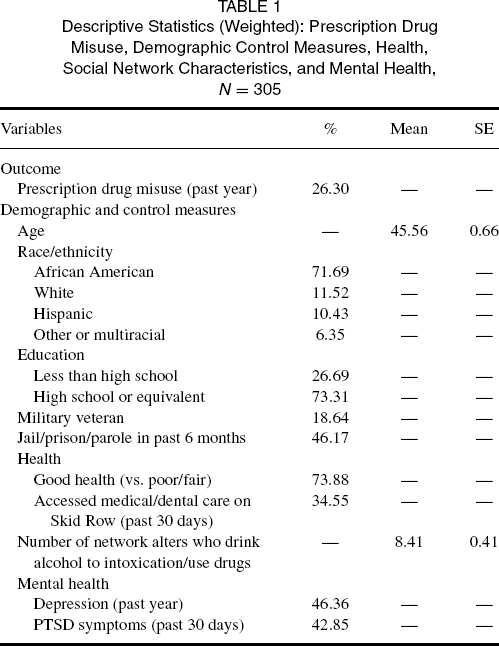
Past-year prescription drug misuse was reported by more than one quarter (26.3%) of the men in this study (Table 1). Most men self-identified as African American (71.69%), followed by white (non-Hispanic, 11.52%), Hispanic (10.43%), and other or multiracial (6.35%). Most respondents (73.31%) had a high school diploma/GED. Nearly 20% (18.64%) had served in the military, and 46.17% had been incarcerated or on parole in the prior 6 months. Men had an average of 8 social network alters whom they perceived to use drugs or drink alcohol to intoxication in the past 6 months. More than one third of the men (34.55%) had used medical or dental care in the past 30 days on Skid Row. Nearly half (46%) experienced depression in the past year, and about 43% reported symptoms of PTSD in the past 30 days.
Descriptive Statistics (Weighted): Prescription Drug Misuse, Demographic Control Measures, Health, Social Network Characteristics, and Mental Health, N = 305
Logistic Regression Results
Multivariate Logistic Regression Results (Weighted) Predicting Prescription Drug Misuse by Demographic Control Measures, Health, Social Network Characteristics, and Mental Health, N = 305
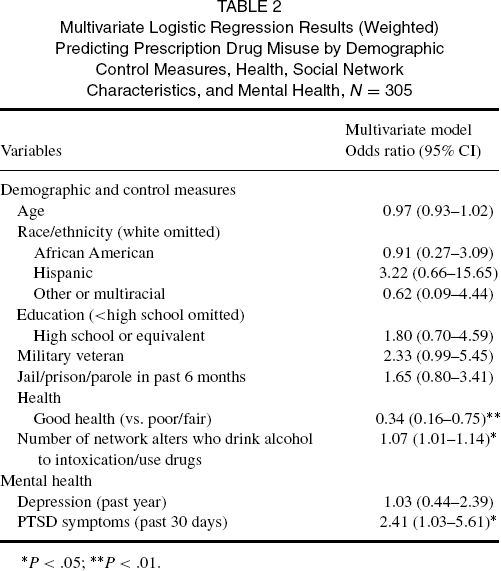
P < .05;
P < .01.
Discussion
More than one quarter of the men in this study reported past year misuse of prescription medication; this rate is much higher than the past year prevalence rate of 4.5% in a national survey of US adults (47). The prevalence of PDM in this population is comparable to or higher than those rates found in studies of other vulnerable populations; other research has found PDM rates of 24% in a community sample of human immunodeficiency virus (HIV)-negative men who have sex with other men (MSM) (48), 15% among low-income women using public clinics in Texas (18), and 11.4% among incarcerated juveniles (13). The high prevalence of PDM among homeless men suggests that this vulnerable population is in need of measures aimed at reducing misuse of prescription medication.
Challenges in addressing PDM among homeless men include the fact that this population already underutilizes substance abuse treatment programs (49, 50). Further, alcohol use and hard drug use are more typically perceived to be associated with homelessness, perhaps limiting awareness of PDM among some service providers. An additional challenge is that there may be fewer barriers for homeless men to obtain access to prescription drugs as compared with illicit drugs, as the there is increasing environmental availability of prescription drugs (3). The men in this study may also have reported misuse of the therapeutic substances that had been prescribed specifically to them, which perhaps suggests the need for improved counseling and monitoring of prescriptions by health care providers (51). These findings should not, however, be used to justify the withholding or underprescribing of pain or other medications from men experiencing homelessness; disparities in prescribing having been documented among racial and ethnic minorities, who are less likely to be prescribed appropriate medication for pain management (52, 53, 54). These findings emphasize the important roles of both drug addiction counselors and primary care physicians in addressing misuse of medications and monitoring the use of prescribed medications.
Perceiving that more social network alters used drugs or alcohol was associated with increased misuse of prescription drugs. This finding is similar to previous research that has found that having social network members who are substance users is associated with increased individual substance use (not including PDM) (25, 26). This finding suggests that social network norms associated with other types of substance use may also play a role in increasing the misuse of prescription drugs. It may also be the case that the men procured prescription drugs through their substance-using social network members, as the majority (70%) of those who misuse prescription medication report obtaining the drugs from friends or relatives (55). Despite increased availability of health care services for homeless persons on Skid Row through initiatives or organizations such as the Community Clinic Association of Los Angeles County (56), homeless persons in general have high levels of unmet need for health care (57, 58), and homeless men may rely in part on their social networks for informal exchange of needed items and help with various problems they face. The possibility that homeless men either share their prescribed medications with members of their social networks or sell them is a topic deserving of additional research.
As was expected, those in better health were less likely to misuse prescription medications. However, past-30-day use of medical or dental services in the Skid Row area was not associated with PDM, suggesting that access to medical services (and thus prescriptions) may not be the primary reason why those in poorer health are more likely to misuse prescription medications. Instead, these men may be self-medicating symptoms of pain or other problems with substances obtained through their social networks or other outlets. Similarly, as homeless populations have high rates of unmet need for medical care (57, 58), PDM among this population may represent self-medication of symptoms for which men are not currently receiving medical treatment. Chronic pain may be of particular concern, as prior research has found that homeless persons are at increased risk for receiving inadequate care for chronic pain symptoms (59). Given the potential for negative health consequences related to PDM (3), misuse of prescribed substances may conceivably also contribute to poor health. Similarly, suffering from symptoms of PTSD was associated with PDM among homeless men living in the Skid Row area. This finding confirms prior research, which has found increased PDM among low-income women with PTSD (18); PTSD has also been associated with crack use in this same population of men (11), and with the self-medicating use of illicit substances among veterans (20). The prevalence of PDM among homeless men with PTSD further supports the hypothesis that these men may be using prescription drugs to self-medicate for both physical and mental health symptoms (both physical and mental health related); this may be particularly relevant given the high proportion of veterans in this study (nearly 19%), as veterans are more likely to suffer from PTSD (though veteran status and PDM were only marginally associated in this analysis).
PDM may be associated with poor general health and symptoms of PTSD in this population not because homeless men are misusing prescription medication as a “high,” but rather to achieve relief of symptoms for which they are not receiving adequate treatment. These findings argue for further investigation to determine the extent of unmet health needs that may be motivating men's use of prescription drugs on their own and without a prescription. Prior research also suggests that understanding the motivations behind PDM is important for prevention and treatment efforts (3).
Several important limitations exist in this study. This paper utilizes data from a study of risk behavior among heterosexually active homeless men in the Skid Row region of Los Angeles and findings may not be generalizable to populations of homeless men outside of this area. Because PDM was not the focus of this study, there are limitations to its measurement in this analysis, particularly because a single measure was utilized that did not differentiate between types of prescription medications. It is important to measure the type of prescription medication being misused; for example, opioid pain relievers are now responsible for more overdose deaths in the United States than those involving heroin and cocaine combined (60). It will be key for future research to examine the specific types of prescription drugs being misused by homeless populations.
Additionally, it is possible that by focusing on sexually active men, we have excluded men whose illnesses precluded them from sexual activity, but whose poor health status may have been associated with a greater propensity to misuse prescription drugs. We also did not ask about pain symptoms, which may be directly related to PDM. These data are also cross-sectional, so we cannot make inferences about the causal direction of the findings. For example, the association between increased drug and alcohol use in the social network and men's own PDM might be a product of substance-use norms in these social groups that encourage PDM; alternatively, the association between social network substance use and respondents’ PDM could be related to homophilous network selection, wherein men choose to associate with other substance users.
Further, we did not ask men in this study how they accessed the prescription medications for which they reported misuse. Although we did control for past-30-day medical and dental service use on Skid Row, it is possible that prescription medications taken during the past year may have been obtained via legitimate prescriptions from other medical service encounters. Additional research into how prescription medication is procured by homeless men could provide insight into how best to address PDM in this population. If homeless men are misusing medication that has been prescribed to them, then interventions could focus on working with medical providers to encourage the appropriate use and monitoring of prescription medication; different responses would be needed to address prescription medication that is being acquired on the street or through social network connections. Despite these limitations, and given the lack of information about PDM among homeless persons, this analysis is an important first step in understanding the correlates of PDM in this vulnerable population.
The prevalence of PDM among this population of homeless men suggests an urgent need for interventions to combat this growing epidemic. As these findings suggest, important factors to be addressed in this context include potential self-medication of PTSD symptoms or other health problems, and the role of substance-using social network connections in influencing the misuse of prescription medication.
Footnotes
Acknowledgments
This research was supported by grant R01HD059307 from the National Institute of Child Health and Human Development.
The authors thank the men who shared their experiences with the authors, the service agencies in the Skid Row area that collaborated in this study, and the RAND Survey Research Group for assistance in data collection. The authors also thank Daniela Golinelli, PhD, for her contributions to the study sampling design, and David Kennedy, PhD, and Harold Green, PhD, for their contributions to the social network analysis design.