
Abstract
Background: Nonmedical use of prescription drugs (NMPUD) has become a critical public health concern. Chinese literature has paid growing attention to NMUPD, but scarce research has focused on females who are sex workers (FSWs), who have a high risk of substance use. The current study aimed to examine NMUPD and its biopsychosocial correlates in Chinese FSWs. Methods: A total of 410 FSWs (mean age = 33.58 years) from Guangxi, China, completed an anonymous, self-administered survey evaluating NMUPD, somatic symptoms, and psychosocial distress. Results: Overall, 46.6% of FSWs reported lifetime NMUPD and 17.6% reported past-3-month NMUPD. The most commonly reported medications that were used nonmedically were analgesics (46.3%, lifetime; 17.6%, past 3 months). A majority of FSWs (69.1%) reported “relieving pain” as the motive of their NMUPD. FSWs reporting NMUPD were more likely to be younger, be unmarried, have higher income, and work in multiple venues/high-paying venues. Somatic symptoms and psychosocial distress were associated with NMUPD in Chinese FSWs. Conclusions: NMUPD was prevalent in Chinese FSWs and was associated with biopsychosocial factors. Critical attention should be paid to NMUPD in FSWs. Future NMUPD prevention intervention among FSWs may benefit from attending to biopsychosocial factors.
Keywords
Introduction
Nonmedical use of prescription drugs (NMUPD) occurs when individuals take prescription medications (e.g., analgesics, sedatives, anxiolytics, and stimulants) without a physician's approval or use prescription drugs for other than a medical purpose (e.g., experiencing). 1 – 3 Due to detrimental consequences (e.g., fatal overdoses), NMUPD has become a major threat to public health worldwide. 4 It has been estimated that globally 24 million and 29 million engaged in past-year nonmedical use of prescription opioids and stimulants, respectively. 5 China has also been suffering from NMUPD problems. Existing data show high rates of lifetime NMUPD in Chinese students, including high school students (14.2%) 6 – 8 and college students (62.9%). 9 However, data are limited regarding NMUPD among other Chinese populations who have a high risk of substance use, such as females who are sex workers (FSWs).
FSWs in China may have a high risk of NMUPD. Substance use literature has documented that alcohol and illicit drug use were prevalent in Chinese FSWs. 10 , 11 There are only a handful of studies focusing on NMUPD in sex workers, and all were conducted in North America. A US study found that sex work was associated with NMUPD in the past month among adults in substance use treatment. 12 A second US study found that 12.2% street-based sex workers reported NMUPD in the past 6 months. 13 A similar finding was documented in Canada, showing that 18.8% of sex workers engaged in NMUPD in the past 6 months. 14 It is important to note that these rates were higher than that in general adult population (3.4%–5.5%). 15
NMUPD in FSWs may be influenced by numerous factors. The biopsychosocial model posits that health behaviors are determined by biological and psychosocial factors. 16 Applying this model, NMUPD studies in young adults or clinic samples identified several biological and psychosocial correlates, such as somatic symptoms (e.g., pain) 17 , 18 and psychosocial distress (e.g., perceived stress, depression, loneliness). 19 – 21 It is noteworthy that, possibly due to psych-behavioral disadvantages (e.g., exposure to violence, stigma, unhealthy lifestyle), FSW are particularly vulnerable to these biopsychosocial problems 22 and these problems have been robustly associated with substance use. 23 Accordingly, biopsychosocial factors may contribute to NMUPD in Chinese FSWs. The current study aimed to identify patterns of NMUPD and to examine the associations of somatic symptoms and psychosocial distress with NMUPD among Chinese FSWs.
Method
Participants and procedure
A convenience sample of women who provided commercial sex was recruited from five regions (Guilin, Guigang, Beihai, Baise, and Heizhou) in Guangxi, China, between September 2019 and December 2019. Guangxi Centers for Disease Prevention and Control (CDC) personnel approached FSWs in sex work venues (e.g., karaoke bars, hotels, and hairdressing rooms) and invited them to participate in the study. After providing informed written consent, 424 FSWs completed an anonymous, self-administered survey. Each FSW was paid 50 RMB (China's currency; equivalent to 7.3 USD at the time of survey) upon completion of the survey. After removing surveys with careless or random responses (e.g., 50% of missing values or more), a total sample size of 410 was used in the present study. The study protocol was approved by the Guangxi CDC Institutional Review Board.
Measures
Demographics
Participants were asked to provide their age, ethnicity, education, marital status, monthly income, the number of working venues in the past year, and the number of clients in the past week. Venues were rated based on an average payment per service as low (<50 RMB), medium (50 − 150 RMB), or high (>150 RMB).
NMUPD
Participants were initially asked whether they had ever used a prescription drug without a physician's approval (yes or no). Participants then answered their lifetime and past-3-month NMUPD (yes or no), respectively, on a list of 21 prescription medications that were commonly available in China. 9 Prescription medications fell into 4 categories: analgesics (e.g., Tramadol), sedatives (e.g., Halcion), anxiolytics (e.g., Valium), and stimulants (e.g., Ritalin). Responses were dichotomized to indicate participants’ NMUPD on these 4 classes of medications in lifetime and the past 3 months, respectively. This measure was similar to a scale utilized in prior research. 9
An 18-item checklist assessed motives (e.g., “help me sleep”) and sources (e.g., “drug stores”) of NMUPD. This scale was adapted from a measure developed by Boyd et al. 24
Somatic symptoms
A Chinese version of the Patient Health Questionnaire-15 (PHQ-15) 25 , 26 was utilized to evaluate participants’ somatic symptoms in the past 30 days. Participants responded on a 3-option scale (0 = not bothered at all, 1 = bothered a little, 2 = bothered a lot) to indicate whether they experienced any of the 15 somatic symptoms, which were divided into 4 categories (pain, cardiopulmonary, gastrointestinal, and fatigue).
Psychosocial distress
Participants completed a Chinese version of the Center for Epidemiologic Studies Depression Scale Revised (CESD-R-10). 27 , 28 The CESD-R-10 included 10 items assessing depressive symptoms that occurred in the past week. Participants rated items on a 4-point scale (1 = less than 1 day to 4 = 5–7 days). A sum score was generated, with a higher score indicating a higher level of depression. The Cronbach's alpha of this scale was 0.71 in the current study.
Participants completed a Chinese version of the short-form UCLA Loneliness Scale (ULS-8). 29 , 30 This 8-item scale measures loneliness, referring to scarcity of social contact compared to what was desired. Participants rated items on a 4-point scale ranging from 1 (never) to 4 (always). One item (“I am an outgoing person”) was deleted because it deteriorated internal consistency. A sum score was calculated among 7 items, with higher scores indicating higher loneliness. The Cronbach's alpha of this scale was 0.70 in the current study.
Participants completed a Chinese version of the Perceived Stress Scale (PSS). 31 , 32 The PSS is a 10-item measure assessing perceived stress (e.g., “felt nervous and stressed”) in the past month. Participants rated items on a 5-point scale (1 = never to 5 = very often). A sum score was generated, with higher scores indicating a higher level of perceived stress. The scale was internally consistent in the study sample (Cronbach's alpha = 0.72).
Data analysis
Exploratory factor analysis was used to identify factorial structure for biopsychosocial measures (i.e., CESD-R-10, PSS, and PHQ-15) and found identical structures suggested by prior research in China. 26 , 33 , 34 Descriptive statistics were performed on demographic variables, NMUPD, and motives and sources of NMUPD. Analysis of variance (ANOVA; for continuous variables) and Chi-square tests (for categorical variables) were employed to examine differences on demographic factors, somatic symptoms, and psychosocial distress by NMUPD measures. Due to non-normality (skewness or kurtosis >3.0) 30 and small sizes in certain categories (<5% of N), we dichotomized several variables (i.e., ethnicity, education, marital status, number of working venues, and somatic symptoms). Data analyses were conducted using SPSS software version 27. 35
Results
Demographics characteristics
Among 410 participants, the mean age was 33.58 years (SD = 9.93). The majority of FSWs were of Han ethnicity (58.8%), followed by Zhuang (26.8%), Yao (9.3%), and Miao (2.0%). Most participants reported that their highest educational attainment was middle school (36.1%), followed by elementary school (23.9%), high school or occupational school (20.5%), no formal education (13.7%), and college or above (5.9%). A majority were married (47.0%), with the remainder being unmarried (35.4%), divorce/widowed (15.1%), and unmarried or cohabitating (2.4%). Participants reported an average monthly income of 4999.95 RMB (SD = 3768.58). The mean number of working venues in the past year was 1.46 (SD = 0.88). Participants reported having 10.12 clients in the past week on average (SD = 5.91).
NMUPD patterns
Nearly one-half (46.6%) of the sample reported lifetime NMUPD and 17.6% reported past-3-month NMUPD. The most commonly misused medication was analgesics, followed by sedatives, stimulants, and anxiolytics (see Table 1).
Patterns of non-medical use of prescription drugs in Chinese females who are sex workers (FSWs) (n = 410).
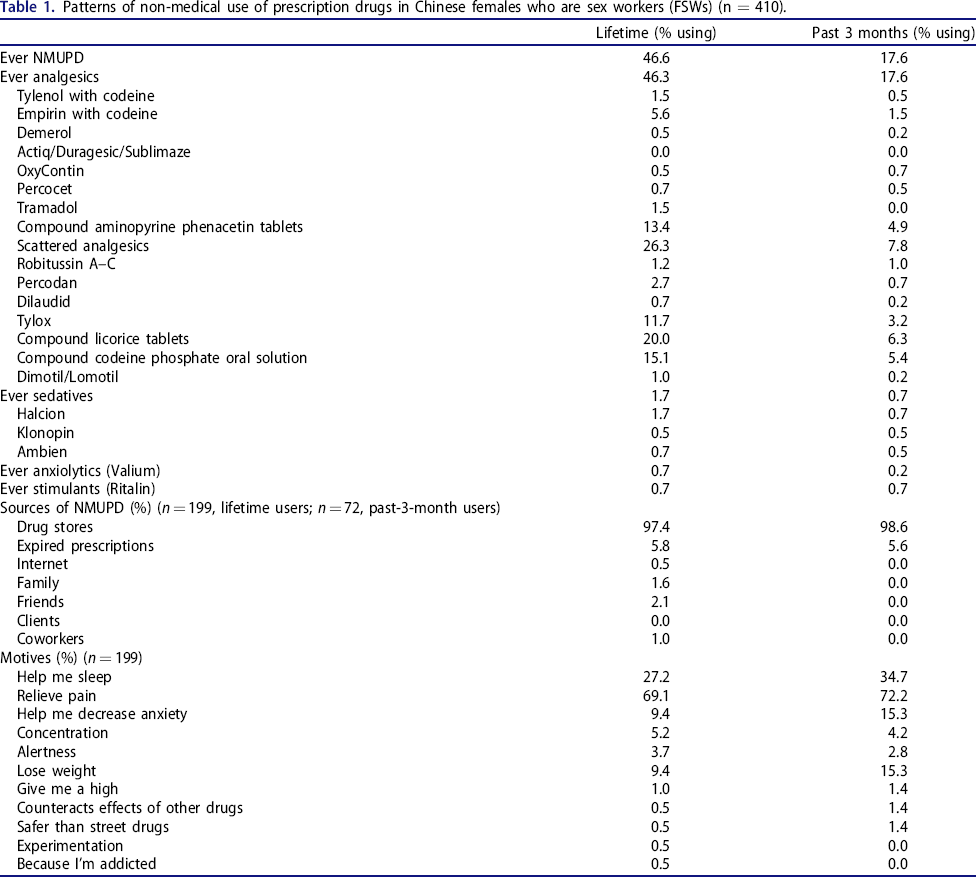
Among lifetime users, the most common source of NMPUD was drug stores followed by expired prescriptions, friends, family, coworkers, and the Internet. The most common motive was “relieve pain,” followed by “help me sleep,” “help me decrease anxiety,” “lose weight,” “concentration,” “alertness,” “give me a high,” “safer than street drugs,” “experimentation,” and “because I'm addicted.” Past-3-month users reported similar patterns of their sources and motives of NMUPD.
NMUPD, demographic factors, and biopsychosocial correlates
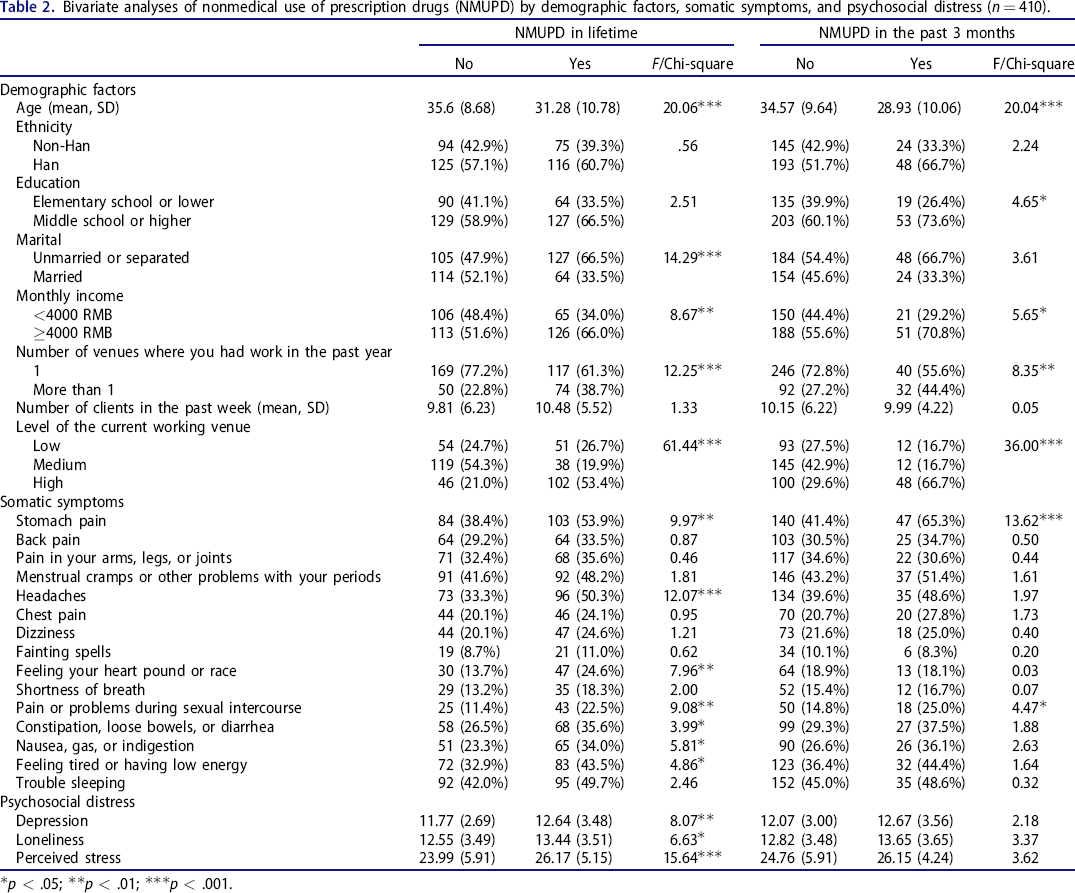
As shown in Table 2, FSWs with lifetime or past-3-month NMUPD were more likely to be younger, earn more than 4000 RMB monthly, work in more than one venue, and currently work in a high-paying venue. FSWs with lifetime NMUPD were more likely to be unmarried, and FSWs reporting past-3-month NMUPD were more likely to have attained middle school or higher education.
Bivariate analyses of nonmedical use of prescription drugs (NMUPD) by demographic factors, somatic symptoms, and psychosocial distress (n = 410).
p < .05;
p < .01;
p < .001.
Regarding somatic symptoms, FSWs with lifetime NMUPD were more likely to report stomach pain, headaches, feeling the heart pound or race, pain/problems during sexual intercourse, constipation/loose bowels/diarrhea, nausea/gas/indigestion, and feeling tired/having low energy. FSWs reporting past-3-month NMUPD were more likely to experience stomach pain and pain/problems during sexual intercourse.
In terms of psychosocial distress, FSWs with lifetime NMUPD reported significantly higher levels of depression, loneliness, and perceived stress. Similarly, FSWs with past-3-month NMUPD reported higher levels of loneliness and perceived stress, but the differences were marginally significant (ps = 0.058–0.067). Depression was comparable between FSWs with NMUPD and no NMUPD in the past 3 months (p = .140).
Discussion
We found that NMUPD was prevalent among Chinese FSWs (46.6%, lifetime). Their recent NMUPD rate (17.6%, past 3 months) was similar to findings in previous studies with sex workers (12.2%–18.8%; past 6 months). Compared to findings for other Chinese groups, the rates of NMUPD among FSWs were higher than that among adolescents (2.9%–14.2%; lifetime) 6 – 8 but lower than that among college students (67%, lifetime; 33%, past 3 months). In terms of specific NMUPD classes, consistent with prior Chinese NMUPD research, 9 the most commonly misused medications in FSWs were analgesics, and this was also reflected in their self-medication motives (e.g., “relieve pain,” 69.1%). Consistent with previous research, 6 , 9 , 36 , 37 prescription analgesics specific to China (compound licorice tablets and scattered analgesics) were among the most commonly used without a prescription. It is noteworthy that nonmedical use of analgesics can lead to severe health problems, such as irregular heart rate, hypertension, respiratory suppression, overdose, and death. 38 – 40 Therefore, NMUPD in Chinese FSWs merits immediate attention. Our results suggested that 0.5% of FSWs engaged in NMUPD with a motive of addiction (i.e., “I'm addicted”), which was similar to findings (0.5–1.0%) in a systematic review in young adults. 41 However, it is worth noting that responses on NMUPD motives may be subjected to several factors, such as classes of drugs 42 and social desirability. To better understand NMUPD motivations in FSWs, future research should utilize validated measures and assess motives according to different classes of drugs.
It is noteworthy that a majority of FSWs (97.4%) reported obtaining their prescription drugs from drug stores. This reflects the loose pharmaceutical regulation in pharmacies, which has been an important concern in China. 43 Regulatory or administrative attention and discussion are warranted to address this issue.
Consistent with previous NMUPD studies, 44 , 45 younger age, higher monthly income, and unmarried status were risk factors for NMUPD. In terms of sex work–related factors, the current study found that FSWs who worked in multiple venues and worked in high-paying venues were more likely to engage in NMUPD. This may be related to hazardous alcohol use, which is strongly encouraged in high-paying venues. Drinking is usually associated with commercial sex in China 11 and FSWs’ income may be substantially dependent on clients’ orders of liquor. Hence, FSWs working in these venues (or multiple venues) would be at high risk for alcohol intoxication, leading to NMUPD for treating alcohol-related symptoms such as hangover. 46 Future research may benefit from examining the association of alcohol use and NMUPD in Chinese FSWs.
This study adds to the growing literature on biopsychosocial influences on NMUPD. 47 Our findings suggested that somatic symptoms (i.e., stomach pain, headaches, feeling the heart pound or race, pain/problems during sexual intercourse, constipation, or fatigue) and psychosocial distress (i.e., depression, loneliness, and perceived stress) were associated with lifetime NMUPD in Chinese FSWs. This finding is important in that Chinese FSWs are particularly vulnerable to physical and psychological problems due to unhealthy lifestyle, stigma, and violence. 48 , 49 In addition, psychosocial distress may worsen physical symptoms and further increase the risk of NMUPD. Such a psycho-physical pathway on NMUPD has been found in a recent study among individuals with trauma (e.g., sexual assault). 50 To better address NMUPD in FSWs, future interventions should attend to nonpharmaceutical strategies (e.g., mindfulness) for managing psychological and physical symptoms. 51 In clinic settings, it is important to assess psychiatric symptoms and NMUPD, which are not usually included in risk screen tools.
This study had several methodological limitations. First, a convenience sample of FSWs was recruited in Guangxi. Generalization of findings to other populations or other Chinese regions may not be warranted. Second, data were cross-sectional, and our findings may not draw causal inference. Third, measures were self-reported. Data may be subject to bias such as social desirability (e.g., endorsing the “I'm addicted” motive). Fourth, measures were adapted, and measures adapted from previous U.S. research (e.g., NMUPD motives checklist) 24 may have limited cultural validity. The fifth limitation was bivariate analyses. Given the small sample size in the recent NMUPD group (n = 72), this study had insufficient statistical power for a multivariate model (e.g., logistic regression) which included all demographic and biopsychosocial measures. 52 Sixth was the NMUPD measure. Our NMUPD scale may not cover other aberrant behaviors associated with prescription drug misuse, such as the use of extra doses or early refills. 53 In addition, drug categories may be potentially overlapping (e.g., Valium could be classified as an anxiolytic or a sedative). Seventh, there was a focus on lifetime NMUPD results. Given a concern of statistical power, our discussion of biopsychosocial correlates was largely based on lifetime NMUPD data. This may not draw inference to recent NMUPD. To better understand NMUPD in Chinese FSWs, future research should employ multivariate analysis using a longitudinal design, culturally validated measures, and a broad measure of prescription drug use from a large sample. Despite these limitations, this is the first study to document NMUPD patterns and its correlates in Chinese FSWs. Critical attention should be paid to NMUPD in Chinese FSWs, and interventions for reducing NMUPD risk in FSWs may benefit from attending to biopsychosocial factors.
Footnotes
Author contributions
CCT and YZ were responsible for the original draft and revisions of the manuscript and data analyses. CCT, YZ, EB, XL, SQ, and QZ were responsible for conceptualizing the study, including developing the methodology, designing the study, and providing leadership. YZ was responsible for data collection.