
Abstract
Medical protective gloves must be assessed to adequate standards before becoming available for commercial use. Strength, integrity and contamination are assessed at the manufacturing stage. However, concerns are raised over the standardisation of the testing; should more be done to assess how gloves affect the performance? Over the years, studies have demonstrated how the design of gloves has reduced tactile sensitivity in medical staff, ultimately leading to poor patient care through missed information. Studies have also demonstrated that a loss of grip control and dexterity through glove use are detrimental to medical tasks. However, it remains relatively unexplored as to how wearing medical gloves affects the users and the patients. Gaps in research have been identified around the frictional and grip properties of gloves. Linking the key performance parameters to the manufacturing processes, which affect material properties, will provide more insight into the behaviour of medical gloves and how to properly assess materials.
Keywords
Introduction
Clinical staff, such as doctors and surgeons, are required to don medical gloves to protect themselves and patients from contamination. Two types of medical gloves exist. Examination gloves; worn for routine medical examinations and minor procedures and surgical gloves; worn for surgeries by surgical staff. The safety performance of these gloves is relatively undisputed. Their effects on hand performance, however, should not be overlooked. Medical gloves have been investigated for possible reduction in performance capabilities [1]. However, it has yet to be determined as to how gloves should be assessed for quality of purpose. Does placing a membrane over the hand have such an effect on performance that a medical professional cannot perform tasks correctly? This review aims to bring together the knowledge available on how medical glove performance has been assessed within the literature. Firstly, focusing on the varied materials of gloves before discussing how gloves have been assessed in previous studies. The advantages and limitations of such assessments will be discussed, and suggestions will be made on improvements if and where applicable. As the review is focusing on real-world applications, studies focusing on sensitivity, dexterity, friction, grip and performance perception will be evaluated. The studies searched for have been studies that look specifically at medical glove materials and measuring differences between them or the bare skin condition. The studies discussed in this review have been identified through searching scientific journal databases, specifically for medical examination and surgical glove assessments along with more specific key terms: ‘dexterity’, ‘sensitivity’ ‘grip’ and ‘friction’. Databases which included institutional access were used, including PubMed, ScienceDirect, PLOS, JSTOR and the University of Sheffield library database, to bring together research from across 38 journals.
Glove materials
The properties of gloves are dependent upon the raw manufacturing materials, manufacturing processes followed, and the chemical treatment gloves receive. Natural rubbers are commonly used, the most prominent being natural rubber latex (NRL), a substance found in the bark of Hevea trees [2]. By nature, NRL is a highly deformable elastomer, allowing easy conformation to the shape of the hand [3]. The Center for Disease Control (CDC) estimates that up to 6% of the worldwide population has a latex allergy [4]. Furthermore, the increasing incidence in NRL allergies means that alternative glove materials must be used where appropriate. Other glove materials include; nitrile (XNBR), polyvinyl chloride (PVC) and polychloroprene [5,6]. The most common alternative material to NRL is nitrile (XNBR), synthetically created using a copolymer of acrylonitrile and butadiene. However, the elastic loading response of XNBR means that the conformability to the hand is perceived to be inferior than that of NRL. The material properties of XNBR gloves are an issue for some, as they report it hinders their ability to carry out tasks [6,7].
Until 2000, powder (e.g. starch) was used to coat the interior surface of gloves, allowing a reduced friction coefficient for donning. However, due to the rise in the incidents of latex allergies, there have been concerns over the proteins in NRL being made airborne upon the removal of the glove [8]. Consequently, in 2010 the Health and Safety Executive (in the UK) released guidelines stating that NRL gloves must be free of powder, prompting the NHS to stop purchasing powdered NRL gloves [9]. As an alternative to powder, chlorination treatment has become a popular choice due to it being a cheap and easy way to treat the glove surface [10]. Gloves can also be treated by chemical coating, such as with hydrogel, a hydrophillic polymer which absorbs water [3,11,12]. Other polymers such as polyurethane can also be used, and new polymers are being developed such as the anti-microbial chlorhexidine-gluconate coating [13]. It is important to note, that medical gloves are not just composed of the raw materials, they contain varying degrees of compounding chemicals to aid the glove formation. The difference in manufacturing methods, the compounding chemicals, and the surface treatment method can create different end products which have differing properties [3,10].
Glove standards
Medical gloves must conform to the EN455 [14] standards, which covers the material integrity, strength, shelf life and carries the CE mark. These also describe the properties required by glove materials to protect from chemicals and micro-organisms [15]. From manufacture, gloves are tested for durability, tensile strength and force at break. The question of whether these are good enough assessments of medical gloves remains. It can be argued that the glove assessments and standards should also be focusing on the user compatibility, rather than just the protection properties of the materials. Very few areas of literature aim to seek out how medical gloves can be assessed to fully evaluate the extent at which placing a barrier between the fingers and the patient or tools in a surgical setting can, for instance, affect tactile and haptic feedback.
Tactile sensitivity
Studies relating to the effect glove materials have on tactile sensitivity. Reduced sensitivity is defined as a reduction in ability to discriminate or identify sensations. For a clear representation of the effects on dexterity, only studies looking at the differences between bare hand and gloves are shown here.
Studies relating to the effect glove materials have on tactile sensitivity. Reduced sensitivity is defined as a reduction in ability to discriminate or identify sensations. For a clear representation of the effects on dexterity, only studies looking at the differences between bare hand and gloves are shown here.
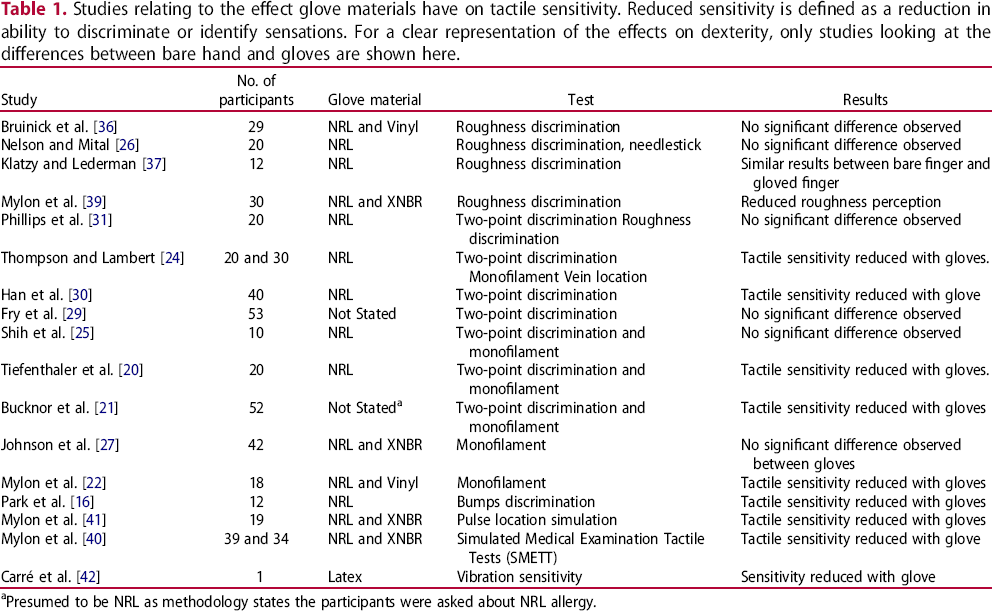
aPresumed to be NRL as methodology states the participants were asked about NRL allergy.
Another commonly occurring test is the roughness discrimination tests. These tests require participants to identify varying bump sizes or roughness/patterns [16,22,34–37]. Of these, only two studies found that detection rates declined when gloves were worn [16,38]. Sandpaper has also been used as a means of measuring discrimination. Mylon et al. [39] showed that subjects could perceive roughness differences when moving their gloved fingers across sandpaper, but not when statically pressing. Palpation or surface anomaly detection with patients would require interaction with skin and tissue that is much more viscoelastic and pliable than the materials used in these studies. Thus, it would be pre-emptive to say that gloves have no effect on the ability to discriminate surface anomalies on or within the body by these test methods. More advanced assessment methods have been produced, such as the Simulated Medical Examination Tactile Tests (SMETT) developed by Mylon et al. [40]. In the ‘bumps’ SMETT test, 100–600 µm pimples were 3D printed on a soft rubber-like sheet which was fixed onto a board. Participants were asked to run their fingers across the sheet to see if any pimples were identifiable. The ‘Princess and the Pea’ SMETT test required participants to identify pegs of varying heights (2.5–14.5 mm) which were submerged in silicone. A similar test was carried out by Gnaneswaran et al. [38] which utilised 1.25 cm dried glue spots covered by sponge. Although the SMETT tests in Mylon et al. [40] do appear to be a valid means of in-situ glove assessment, several areas with room for improvement exist in the methodology and design. It was found that the silicone became stiffer over time, making it harder to identify the pegs. Participants also varied placing their fingers flat or perpendicular to the test beds, which could produce different results due to the dispersion of mechanoreceptors. This could provide differing results between people and between the gloving conditions. Although the bumps and roughness discrimination tests are a good measure of identifying tactility loss, it could be argued that the use of more appropriate surfaces that replicate the body and environmental conditions would lead to more accurate results in a clinical context.
An inability to detect a pulse is the most common reported reason for removing or not donning gloves. A study by Mylon et al. [41] considered the effects of gloves on pulse detection using a design whereby water was pumped through one of five tubes under a layer of neoprene sponge using a peristaltic pump. They found significant differences in ability to feel the ‘pulse’ in gloved and ungloved conditions. The authors note that this cannot accurately simulate a pulse test due to the pump limitations on the speed and pressure. Also, there was the potential for bias due to the inability to vary the pulse location. Using a pump that will allow the same pressure and speed of blood would be more simulative of the real world. A more quantifiable way of assessing tactility differences is through the use of vibrations. Carré et al. [42] used a vibrating platform to measure the sensitivity difference of fingers when an NRL glove was donned. The glove was found to reduce tactility when compared to the no-gloves condition. However, only one participant was used for this. Overall, studies regarding tactile sensation show that gloves have an adverse effect on ability to feel. However, the extent to which this becomes a detriment still remains unknown. Many of these tests aim to quantify tactility loss, but results differ between studies, possibly due to the different methodology. To quantify tactility loss, further studies looking at how the gloves dampen vibration, like in Carré et al. [42], could prove vital for future work. Some of the studies discussed here were conducted prior to the banning of powder-coated NRL, thus the results may not applicable to gloves used today due to the differences in manufacturing. Gnaneswaran et al. [38] stated that powdered NRL gloves are better because they have ideal properties. There is a chance that this powder could affect the frictional properties of gloves in any of dynamic tactility tests, which may give different results. Many of the studies cited regarding sensitivity are vague in terminology, describing the gloves tested as ‘thick or ‘thin’ without giving any measurements. Due to the issues arising with these assessments, it is unknown as to how much medical gloves affect the tactile sensitivity of a user, but it is clear they are having a negative effect. When comparing glove thickness, studies have found that the thinner gloves provide more sensitivity [28,30]. Surgical gloves are often marketed as offering better ‘tactile sensitivity’, however, studies looking at the difference between medical examination and surgical gloves have found no measurable difference in sensitivity [20].
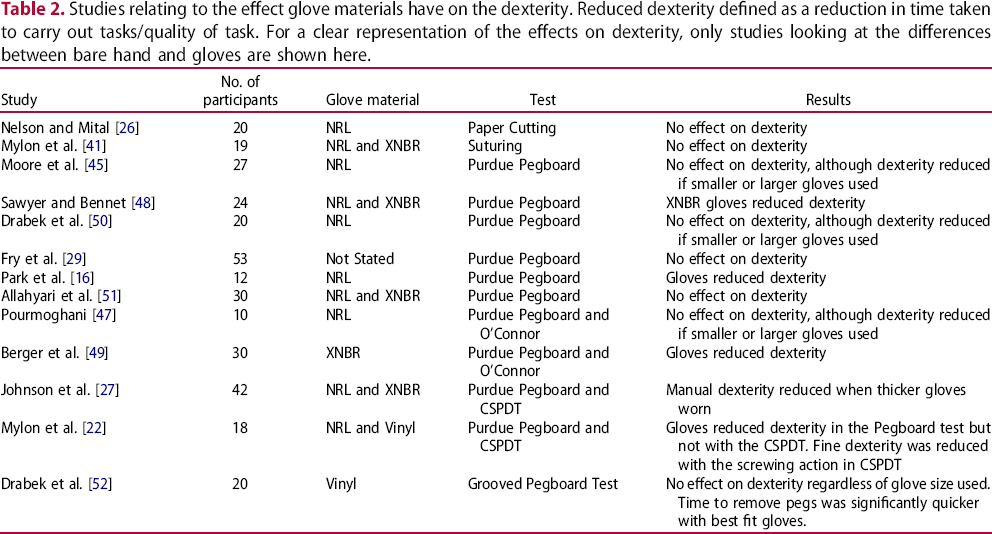
Studies relating to the effect glove materials have on the dexterity. Reduced dexterity defined as a reduction in time taken to carry out tasks/quality of task. For a clear representation of the effects on dexterity, only studies looking at the differences between bare hand and gloves are shown here.
Studies relating to the effect glove materials have on the dexterity. Reduced dexterity defined as a reduction in time taken to carry out tasks/quality of task. For a clear representation of the effects on dexterity, only studies looking at the differences between bare hand and gloves are shown here.
The frictional properties of medical gloves are an important factor which glove manufacturers should consider. It is these properties which allow for the users to ascertain grip and have a sense of force they are applying, which is imperative for the ability to carry out tasks such as holding tools and applying pressure to wounds. Accurate force control for grip precision demands finer detailed information from mechanoreceptors in the skin, thus when these are blocked by a membrane, it would be reasonable to assume that grip force would be impaired [16]. Much of the work regarding grip is oriented at industrial applications and extra vehicular activity gloves for use in space [43], with few looking at medical gloves. Gnaneswaran [38] showed that when powder was present on the gloves, more grip force was exerted. This is presumably because the frictional properties of the gloves were lowered due to the presence of the powder. However, similar findings were reported in Shih et al. [25], Willms et al. [57], and Kinoshita [58] who reported that thicker NRL gloves made participants exert more grip force when picking up a desired load. They conclude that gloves should be thicker in order to retain a greater grip force. However, it has been shown that that thicker gloves impair sensitivity [28,30]. Park et al. [16] looked at the role of mechanoreceptors in force control and the effect of gloves on precision grip. The study found that there was a 20% increase in measured grip force when subjects lifted a heavy object after lifting a light object when gloves were not worn. This grip force was not significantly different when the same test was carried out with NRL gloves, suggesting the sensorimotor effects of gripping were not affected by the gloves. Only one study was located where there was a measured decrease in the grip force with XNBR and vinyl gloves [59]. Many of these studies appear to see an increase in force as beneficial, as grip is imperative for control. Although, these studies do not look at the effects of this force increase on the hands. It could be that this increase in grip, however slight, could affect fatigue on the hand and arm, thus affecting dexterity and performance. It should also be noted, that the over-gripping effect could be due to a reduced friction coefficient between the object and the hands when gloves are introduced [59]. As with Willms et al. [57] it would be interesting to assess how much pressure is instinctively applied and then how that adjusts overtime during a surgical procedure. However, assessing whether the change in load is down to the gloves or the tasks carried out during surgery itself could prove to be a difficult.
Studies looking at the frictional properties focus on surfaces that are impractical to the medical profession, such as glass and sandpaper [25,60,61]. Mylon et al. [39] found no significant difference between NRL and bare hand friction with sandpaper but found a significantly lower friction coefficient with XNBR. Carré et al. [42] looked at the friction of surgical gloves on steel and found that the friction coefficients of NRL gloves were greater than the bare hand condition. This finding is different from Shih et al. [25], who noted that the coefficient of friction decreases when NRL gloves are donned. Laroche et al. [62] looked at the static friction of wet NRL and XNBR gloves on a variety of dental tool patterns. Greater friction coefficients for tools with knurled surface patterns were observed. Although this is the first test to incorporate real tool patterns with fluids, this could be greatly improved by having more realistic bodily fluids in contact with the gloves, such as saliva [63]. The study also did not include a control, such as no gloves or dry gloves to compare. However, this is the only study found measuring the performance of medical gloves in the presence of a contaminant. Evermore, paying consideration to the reason why gloves are worn is vital for friction assessments. In medical settings, gloves act as a barrier to protect from bodily fluids. None of the frictional tests incorporate simulative bodily fluids into the systems to assess how frictional properties may change, which will affect sensitivity and dexterity. This is a fundamental consideration, especially in surgical tasks where gloves are more likely to be in contact with bodily fluids (such as blood) and then wide range of tools. Including fluids into assessments would provide a greater significance to the results of any of the friction and grip studies being conducted. Further studies could then look at the effects of vibration on dexterity with fluids, such as replicating holding a tool such as a surgical drill. The frictional properties of the inside of the gloves also require consideration from glove manufacturers. Often a quick change of gloves is needed in fast-paced environments which can be made difficult with the presence of moisture [64]. Roberts and Brackley [12] found that coating the glove with hydrogel gives a lower coefficient of friction than chlorination treatment, thus enabling easier donning. Pavlovich et al. [64] demonstrated that when hands were wet, the gloves became more difficult to don and greater force was required to pull the glove on, when compared to dry. However, in this study, the hands were wet, with no drying process involved. This is unrealistic of the real-world scenario of requiring a quick change of gloves. Damp skin has been demonstrated to have higher friction coefficients when compared to dry skin [65]. As many issues lie with donning gloves with damp hands, this should be of consideration when assessing the frictional properties of the inner surface of glove materials with [64].
Double gloving
Throughout the literature, it is recommended that where surgery is a high risk due to diseases, such as HIV, two layers of gloves are worn to minimise exposure. Much of the research on double gloving is centred around puncture indication during surgeries (i.e. using different coloured gloves to indicate the outer glove layer has ruptured) [66]. Johnson et al. [27] and Kopka et al. [28] both show that dexterity decreases when thicker gloves are worn. Thus, it would seem reasonable to believe that dexterity would be greater affected when multiple layers are worn, as the thickness is increasing which could restrict movement. However, Webb and Pentlow [67] found that double gloving did not affect dexterity when looking at knot tying. Fry et al. [29] also determined that there was no statistically significant difference in performance when subjects wore two glove layers compared to one when completing the Purdue Pegboard test. There are, however, opposing results with regards to the effect of double gloving on tactile sensitivity. Novak et al. [19], Shih et al. [25] and Han et al. [30] show that there is a loss in tactile sensitivity when assessed by monofilament or two-point discrimination. On the other hand, Fry et al. [29] and Webb and Pentlow [67] show no statistical difference in two-point discrimination between one and two glove layers. Germaine et al. [68] demonstrated that double gloving is not favoured amongst surgeons. Out of the 170-medical staff asked, when practice recommends that they double glove, 78 said that they do not as it decreases their dexterity and 62 said that it was not comfortable. Regardless of the evidence involving the practicality of double gloving during high-risk surgery, there is little discussion in the literature as to how to double glove. Hollaus et al. [69] discuss using the same sized gloves as well as whatever makes the user comfortable. However, much of the literature focuses on the method used in Fry et al. [29] and recommend double gloving by using a larger inner layer glove and a smaller outer layer glove. The authors suggest this reduces dermatological issues but does not offer any insight into how dexterity and tactile feedback may be affected via this method.
Performance perception
One of the major issues in glove assessment is the material preference of the user. Studies show glove users have a negative perception of performance when un-preferred glove materials are used, despite there being no statistically significant change in measured performance in some of the studies. [7,29,35,36]. Along with Mylon et al. [7], Fry et al. [29] also showed that surgeons prefer NRL to XNBR because the XNBR appeared to be thicker, although, the materials were in fact, the same thickness. Few studies have demonstrated a correlation between the perceived and actual performance [22,70]. The studies looking at performance perception, such as Mylon et al. [7] focus on more experienced medical practitioners rather than junior. In terms of assessing perceptions within a clinical environment, focusing on junior staff could give more accurate feedback as they more inclined to undertake a variety of tasks. Thus, the increase in task variety could induce a broader and more accurate determination of perceived use in different areas and activities. Irrespective of performance, surgeons and clinicians’ express criticism for glove materials that are different from their preferred choice by claiming the gloves are too thick, slippery and ill fitting. To properly assess medical gloves, this bias against other materials needs to be considered when evaluating the performance, as it is possible the perception of the performance can decrease the actual performance.
Paper grading
To identify gaps where research is required, a paper grading system has been adapted from Harmon and Lewis [71] and Watson et al. [72] who found that study design and reporting of key findings was flawed across the field of tribology. The aim of this grading differs from these by the way of trying to identify areas where research should be focused in the future. The grading is focused on application of research to relevant systems within the clinical environment and categories differ from those used in previous papers in order to reflect the aim and the practices used in this area of research. It is noted that this way of grading papers is subjective, thus the grading has been kept to matter-of-fact as opposed to subjective analysis (i.e. focusing on participant number and statistical analysis as opposed to the experimental design). It is important to note that not all of these criteria will be applicable to the study designs for this grading. This means that a study which scores highly is not essentially a good study, but a study that fulfils more of the criteria. Similarly, a high score may include all criteria, but whether the entire study is fundamentally flawed will not be determined by this grading. The research papers used in this review have been graded according to the following criteria:
Repetition of work: does the study repeat tests to obtain an average result? Number of participants/samples: does the study have a respectable number of participants/tests? (The average participant/sample number throughout these tests is 30, thus this has been used as a benchmark. Anything <30 does not meet these criteria). Statistical analysis: has a statistical analysis been conducted? Conclusions: are the conclusions in the paper based on the results presented? Real-world simulation: does the work simulate a real-world clinical and/or surgical scenario? E.g. suturing, pulse-feel, etc. Glove material: have multiple glove materials been studied?
A grade ‘A’ constitutes as fulfilling 5–6 of the criteria; grade ‘B’ constitutes fulfilling 3–4 of the criteria and grade ‘C’ constitutes 0–2 of the criteria. A graphical representation of the results is displayed in Figure 1. Much of the research is focused on durability; this is most likely to be because the durability of medical gloves is significant to function. Thus, this is an area of primary focus. However, these assessments have focused mainly on obtaining and testing gloves after surgical procedures have been performed. As there are a great number of different surgical procedures, each with different tasks and different periods of glove wearing, this may result in incomparable data within the literature. Very few studies focus on the grip and frictional properties of medical gloves. It is recommended that further research should be carried out into the frictional properties as well as the performance effects of tactile sensitivity and dexterity of gloves. Although many of the studies here have good grades by these defined criteria, many of the methodologies lack standardisation and do not have a control or a baseline reading of the gloves. Also, as these studies are looking at a variety of surgeries, there is a tendency to statistically compare the perforation rates. However, in some studies there are orders of magnitude difference between the duration and type of procedure as well as the total number of procedures included, thus making for an unfair comparison between studies, leading to erroneous conclusions [5,12,16,19–32,34–42,45–54,57–62,73–91].
Grading of glove related papers to assess gaps in knowledge.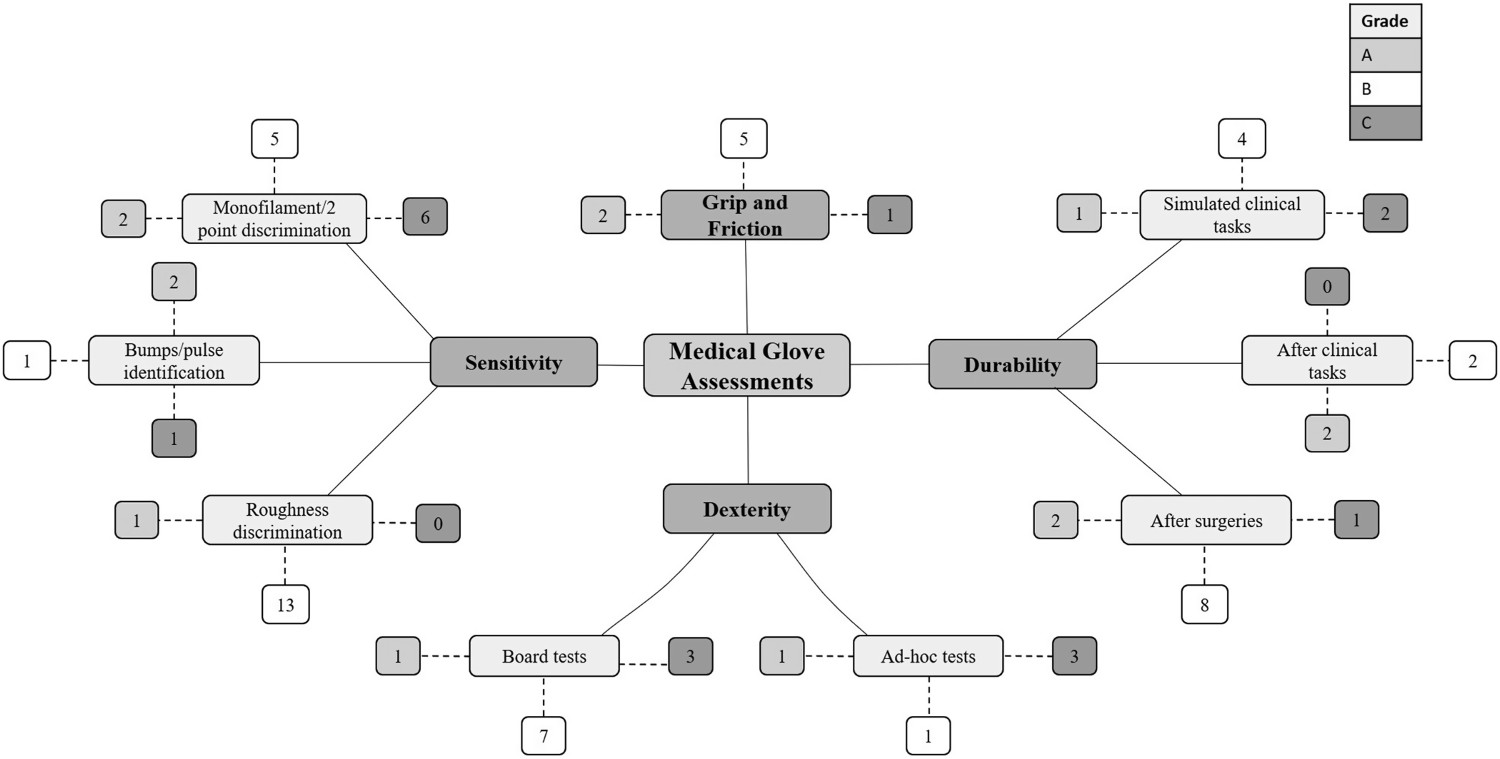
The results of most of these studies indicate that medical gloves have a negative effect on tactile sensitivity and user comfort. The research in this field compares different glove materials to determine differentiating performance, rather than assessing the effects gloves have overall. It can be argued that, as no general differences are present between NRL and XNBR gloves there are no major differences in the overall effects on the user. However, research needs to focus on how to assess the gloves effectively to reduce any negative impact they may have on the performance of users. In order to fully evaluate the effects of medical glove materials on user performance, the use of contaminants must be present in the assessments. Similar assessments to existing studies could be developed using different materials and/or simulations that reflect the depth and feel of the skin/tissues to have a more realistic view of the effect of gloves in medical environments. Evaluation of the frictional performance of medical gloves is crucial to understanding how gloves affect grip. This understanding of the principle friction mechanisms can then be applied to key performance issues such as dexterity and sensitivity. Thought should also be given to the fact that the materials surface could be different due to the different processes and treatment methods involved in glove manufacturing. Linking these key manufacturing parameters to performance will give better information about which processes affect the key performance areas. Blinding tests where possible is recommended to limit the psychological ‘status-quo’ bias that is evident throughout the literature when medical professionals are used as participants.
Conclusions
Overall, studies suggest that sensitivity, friction and grip are affected when medical gloves are worn but dexterity is not. The differences in results between studies of the same tests, could be down to the difference in glove properties, arising from differences in manufacturing When assessing medical gloves, the purpose of the barriers should be considered in the tests and contaminants should be incorporated. Understanding how these affect the frictional properties of the gloves will provide vital insight into how medical gloves perform Linking the key manufacturing parameters to performance will give better information about which processes affect performance. Including the assessment of a desired performance characteristic into the manufacturing process will ensure the production of high-quality gloves that are fit for purpose
Footnotes
Disclosure statement
No potential conflict of interest was reported by the author(s).