
Abstract
Objective:
The objective of this article is to investigate brain activity of scalp acupuncture (SA) as compared to upper and lower limb acupuncture (ULLA) using functional magnetic resonance imaging (fMRI).
Subjects and methods:
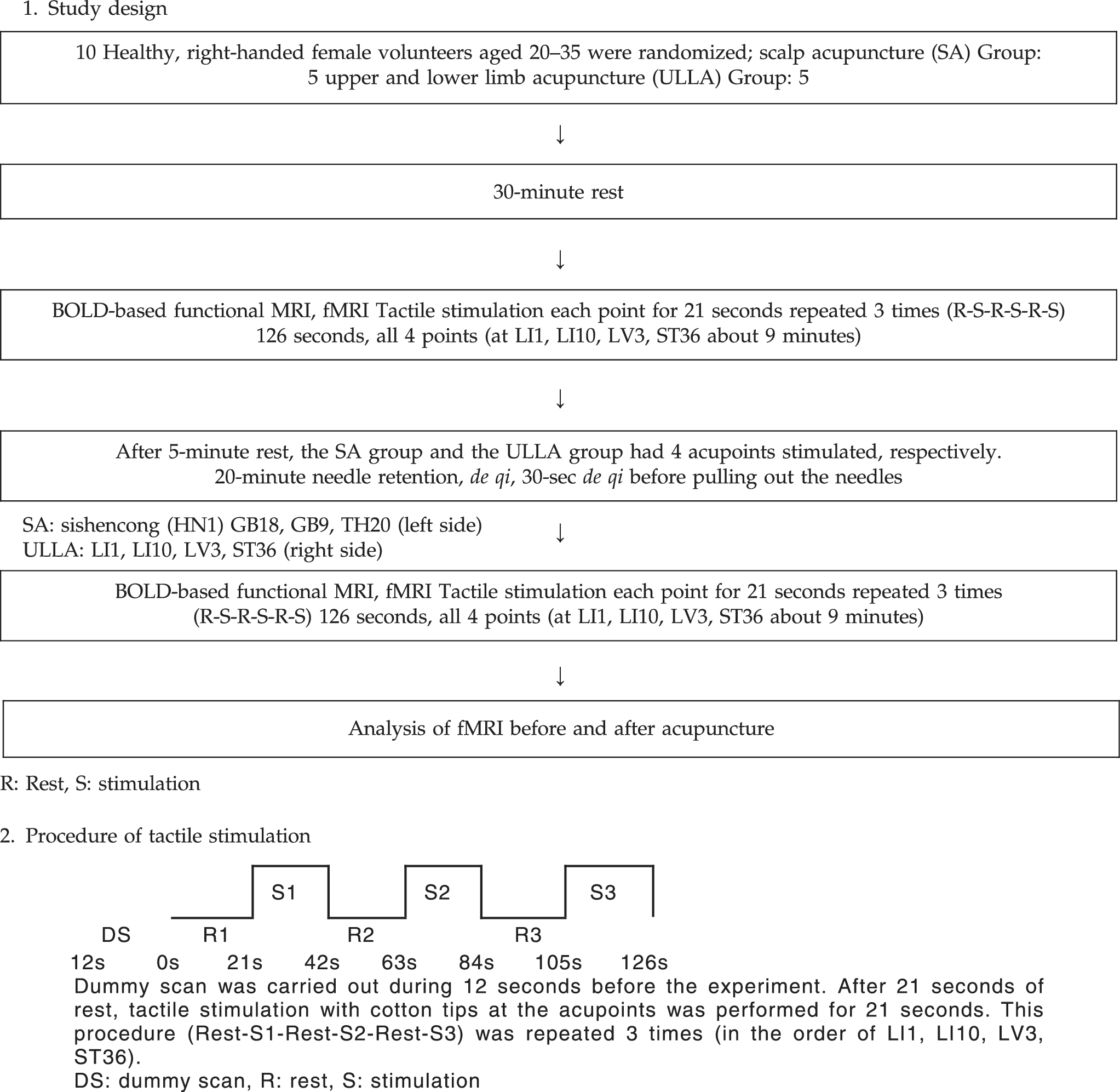
Ten (10) healthy right-handed female volunteers aged 20–35 were divided into 2 groups: a SA group and an ULLA group. The SA group had needles inserted at the left Sishencong (HN1), GB18, GB9, TH20, and the ULLA group at the right LI1, LI10, LV3, ST36 for 20 minutes, respectively. Both groups had tactile stimulation in the order of the right LI1, LI10, LV3, ST36 before and after acupuncture for a block of 21 seconds repeated 3 times. The blood oxygen level dependent (BOLD) fMRI was used to observe the brain and somatosensory cortex signal activation.
Results:
We compared the signal activation before and after acupuncture needling, and the images showed signal activation after removing the acupuncture needles and the contralateral somatosensory association cortex, the postcentral gyrus, and the parietal lobe were more activated in the SA group. The right occipital lobe, the lingual gyrus, the visual association cortex, the right parahippocampal gyrus, the limbic lobe, the hippocampus, the left anterior lobe, the culmen, and the cerebellum were activated in the ULLA group.
Conclusions:
We concluded that there were different signal activations of BOLD fMRI before and after SA versus ULLA, which can be thought to be caused by the sensitivity of acupoints and the different sensory receptors to acupuncture needling.
Introduction
Recently, fMRI has been used to image areas of the brain activated by visual, motor, and sensory stimuli and to visualize cognitive functions such as language and memory (functional brain mapping). 7 –19 Thus, early diagnosis and treatment of certain diseases through observation of brain functions prior to the structural change occurs has become possible. 20 –25
fMRI is also being utilized to verify the mechanisms and the efficacy of acupuncture. There have been several studies to observe which part of the brain is activated when a specific acupoint is stimulated, 26 –28 or after multiple acupoints were stimulated, 29,30 and to see whether different methods of needling have different brain activations. 31,32 These studies used acupuncture to a limited extent on the upper and lower limbs to see the effects of acupuncture on the brain.
However, this study observed the activation and deactivation of the brain and investigated which part of the brain performs specific functions of the high cerebral cortex when tactile stimulation was done on upper and lower limbs using fMRI. Furthermore, we observed the duration of the effects of acupuncture and compared blood oxygen level dependent (BOLD) fMRI signal activations before and after acupuncture in the SA and the upper and lower limb acupuncture (ULLA) groups.
Materials and Methods
Subjects
Ten (10) healthy right-handed female volunteers aged 20–35 were recruited and consented to the study. None of the participants were menstruating or pregnant. Volunteer candidates suffering from neurological, mental, or internal problems; drug abuse; alcohol abuse; or those with a history of cardiovascular or cerebrovascular diseases and on medications that could affect cerebral blood flow were excluded. Caffeinated drinks such as coffee were restricted on the day of the examination.
Materials
For acupuncture, disposable, stainless steel 0.25 mm ×40 mm (diameter × length) needles made by Dong-bang Acupuncture & Moxibustion Company were used.
Methods
The 10 subjects were randomized into 2 groups: a SA group and an ULLA group. After 30 minutes of rest, cotton tips were used to stimulate the members of both groups 3 times on the right upper and lower limbs (LI1, LI10, LV3, ST36) and the first fMRI was administered. After 5 minutes of rest, the SA group was stimulated at the left Sishencong (HN1), GB18, GB9, and the ULLA group was stimulated at LI1, LI10 (located at the right upper limb), LV3, ST36 (located at the right. lower limb) for 20 minutes. De qi was to be achieved through needle manipulation when inserting the acupuncture needles and 30 seconds before the needles were pulled out. The ULLA group had needles inserted 1.5–2 cm deep vertically while the SA group had them inserted obliquely. After the needles were pulled out, cerebral perfusion MRI and BOLD-based fMRI by blood oxidation were performed in the same manner as the first time after a 21-second block tactile stimulation was repeated 3 times. (To limit variables while stimulation, it was done by the same person. Tactile stimulation was performed twice per second consistently and softly. Acupoints were needled until de qi was achieved).
Image acquisition
Preparations
A subject was positioned supine, with the head in the standard head coil to adapt to the surroundings after 30 minutes of rest. The head was fixed by a sponge and during fMRI shooting the subject was not supposed to move or open her eyes. The fMRI room was lit darkly and there was no sound other than the sounds from the fMRI machine. All images were acquired by a well-trained professional operator at East-West Neo Medical Center, Kyunghee University.
fMRI imaging
3.0 Tesla MRI (Philips, Acheiva, Best, The Netherlands) was used. To maximize the effect of BOLD, gradient-echo technique was used. With the echo planar imaging technique, matrix size 64 × 64, field of view (FOV) 230 × 148 × 230-mm T2-weighted images (echo time [TE] =30 ms, repetition time [TR] = 3000 ms, flip angle = 90°) were acquired. There were 30 slices, 5-mm width, the gap between slices was 0 mm, the size of voxel was 3.43 × 3.43 × 5 mm, and there were 42 volume images.
Anatomical MR acquisition
Additional 3D-T1-weighted images (TE = 5 ms, TR = 9.335 ms, flip angle = 8°, FOV =240 × 240 × 185 mm, 120 slices, slice width 1.0 mm) were obtained to see the anatomical structure.
Data analyses
SPM 2 (Wellcome Department of Cognitive Neurology, London, UK) was used for data analyses.
Motion correction
Motion of the head was calculated by rotation and translation on X, Y, and Z coordinates and realigned automatically using 3D motion correction.
Spatial normalization
fMRI images and anatomical MR images have different resolutions, so there needs to be a procedure to compound on the common coordinates. First, anatomical images were standardized using standard anatomical space 33 devised by Talairach and Tournoux. Anatomical images before normalization and fMRI images went through coregistration, and anatomical images were normalized in the same fashion as the anatomical images. 34
Spatial smoothing
Gaussian filter was used to smooth the checkered 64 × 64 plane resolution and 5 mm in width data. The full width at half maximum was set to 9 × 9 × 12 mm for multi-analysis.
Statistical analysis
Individual statistical analysis.
Each normalized image was processed by general linear model (GLM) taking hemodynamic response into consideration. Among the GLM-processed BOLD signal, we chose significantly activated areas to analyze.
We obtained a contrast map for activated areas of each experimental group. Through multiple comparison using NONE p-value below 0.001 was considered significantly different. Group statistical analysis
To compare the BOLD fMRI signal activation before and after acupuncture, we used a contrast map of individual patient and went through an analysis of variance test. P-value less than 0.001–0.05 was considered significantly different.
Results
Change of BOLD fMRI signal activation after tactile stimulation (total 10 volunteers)
LI1
Tactile stimulation at the right LI1 activated the left parietal lobe, the postcentral gyrus, the primary somatosensory cortex (BA 1, 2, 3), and the primary motor cortex (BA 4) (p = 0.001) (Fig. 1).
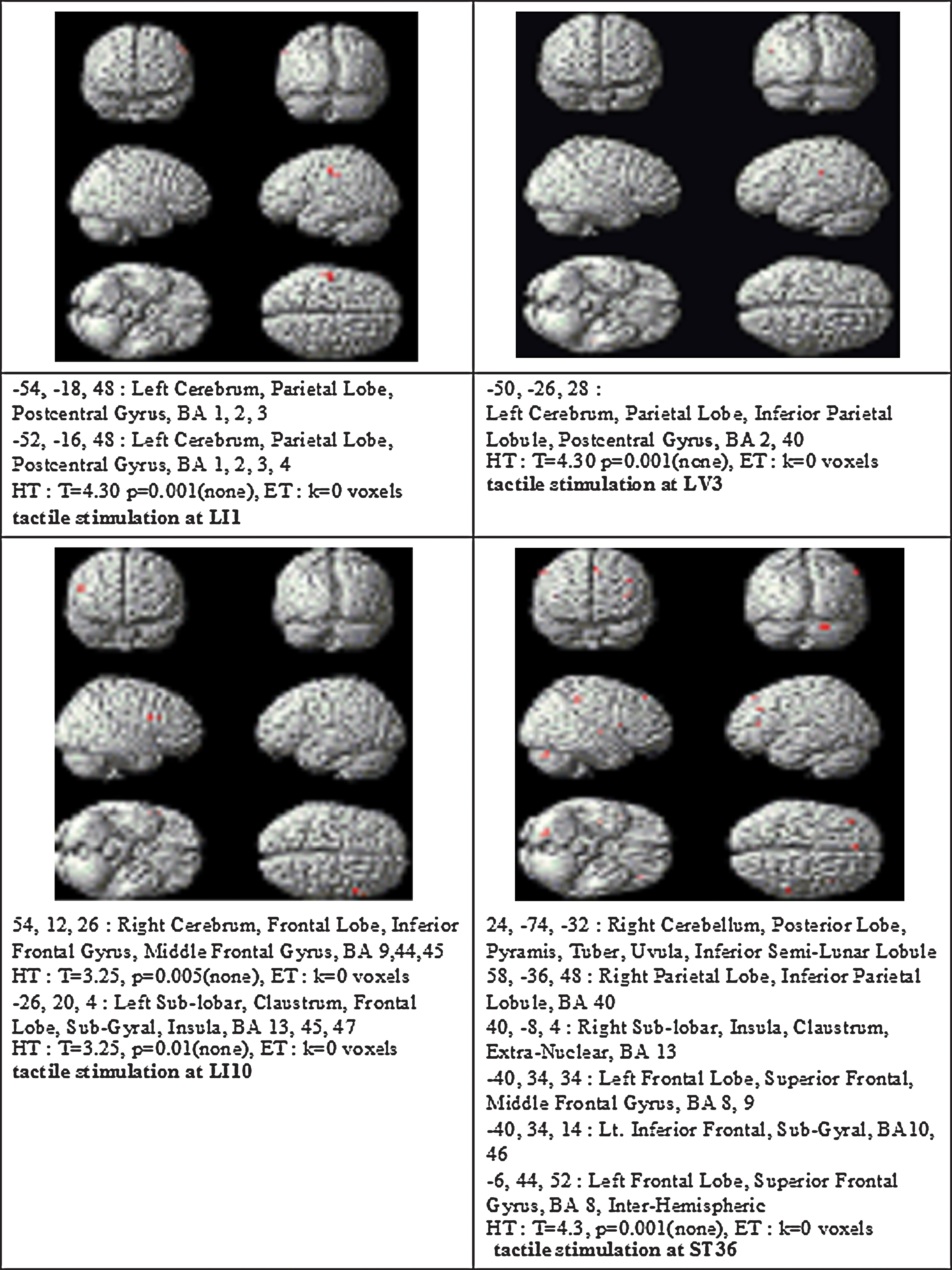
Brain areas with significantly increased cortical and brain activation during sensory tactile stimulation. HT, height threshold; ET, extent threshold; BA, Brodmann area.
LI10
Tactile stimulation at the right LI10 activated the right frontal lobe, inferior frontal gyrus, the middle frontal gyrus (BA 9, 44, 45, p = 0.005) and the left sublobar, the claustrum, the frontal lobe, and the subgyral insula (BA 13, 45, 47, p = 0.01) (Fig. 1).
LV3
Tactile stimulation at the right LV3 activated the left parietal lobe, the inferior parietal lobule, the postcentral gyrus, BA 2, 40 (primary somatosensory cortex, supramarginal gyrus part of Wernicke's area, p = 0.001) (Fig. 1).
ST36
Tactile stimulation at the right ST36 activated the left frontal lobe, the superior frontal, the middle frontal inferior frontal gyrus, the subgyral (BA 8, 9, 10, 46), the interhemispheric, the right cerebellum, the posterior lobe, the pyramis, the tuber, the uvula, the inferior semilunar lobule, the parietal lobe, the inferior parietal lobule, the sublobar, the insula, the claustrum, the extranuclear, and BA 13, 40 (p = 0.001) (Fig. 1).
Change of BOLD fMRI signal activation before and after acupuncture in the SA group (group statistical analysis, 5 subjects)
After SA, the right somatosensory association cortex (BA 7), the postcentral gyrus, and the parietal lobe showed more activation (p = 0.001) (Table 1).
Height threshold: p = 0.001 uncorrected.
BA, Brodmann area.
Change of BOLD fMRI signal activation before and after acupuncture in the ULLA group (group statistical analysis, 5 subjects)
There was more signal activations before acupuncture in the left and right sublobar, the thalamus, the right frontal lobe, the left inferior semilunar lobule and after acupuncture the left and right occipital lobe, the lingual gyrus, the visual association cortex (BA 18, 19), the right parahippocampal gyrus, the limbic lobe, the hippocampus, the left anterior lobe, the culmen, and the cerebellum (Table 2).
Pre, before upper and lower limb acupuncture (ULLA); post, after ULLA; BA, Brodmann area.
Comparison between BOLD fMRI signal activation of the SA group versus upper and lower limb group (Group statistical analysis)
In the ULLA group, there was more activation on the left side of the brain such as the left frontal lobe, the precentral gyrus, the postcentral gyrus, the subcentral area, the parietal lobe, and the right parietal lobe, the postcentral gyrus, and the primary somatosensory cortex (BA 2). In the SA group, particularly in the right (contralateral) pre–post central gyrus, the frontal lobe, the parietal lobe, the primary somatosensory cortex (BA 3), and the primary motor cortex showed more activation compared to those of the ULLA group (Table 3).
BA, Brodmann area.
Discussion
With the instrumental development of MRI and its new imaging techniques in the 1990s, it has become possible for us to get functional information of the brain such as diffusion, perfusion, MR spectroscopy, and functional brain mapping as well as anatomical information. 7 Images by fMRI, which is capable of mapping brain functions, show a close correlation with those obtained by positron emission tomography, and are excellent in spatial resolution and do not require any radioisotope or contrast media with its repeated use, so fMRI is being widely used. 8 –10 Healthy subjects have been part of the studies that visualize images of activated brain areas invoked by visual, motor, and sensory stimulation. Recently, cognitive functions such as language and memory functions are also being visualized by fMRI. 11 –17,35 Clinically in brain tumor removal operations, fMRI is used to decide which part of the tumor should be operated and to predict functional damages after the surgery. 19 –22 It is also used to locate language dominance in patients with epilepsy, 18 to evaluate recovery from strokes, and to explain reorganization of the brain. 23 –25
In the field of Korean traditional medicine, fMRI is mainly used to investigate the mechanisms of acupuncture and to verify its effect. There have been several studies to observe which part of the brain is activated after a specific acupoint is needled, 26 –28 or after multiple acupoints were needled, 29,30 and to see whether different methods of needling have different brain activations. 29,30 However, there has been no study so far involving scalp acupuncture with fMRI because of technical problems. A previous study was done to see whether the fMRI images were still valid after 30 minutes of acupuncture, and was designed to investigate brain activity after acupuncture needles were pulled out. 36 Thus, we designed this study accordingly to compare before and after acupuncture needling when sensory tactile stimulation was done throughout the session.
This fMRI study proves the theory that tactile stimulation is received bilaterally in the brain but shows contralateral dominance. 37,38 Also, tactile stimulation is consistent with high cerebral cortex functions and the specific acupoint ST36 showed diverse activations in the frontal lobe, the parietal lobe, the cerebellum, the posterior lobe, as well as the interhemispheric.
In a preliminary study where they used electroacupuncture, manipulation time varied at the same frequency in each subject to make sure de qi was achieved. After SA on the left side, we could observe that the right parietal lobe, the postcentral gyrus, and the somatosensory association cortex were activated (Table 1). It mostly accords with the areas activated by tactile stimulation, but the fact that the right parts of the brain were more activated by acupuncture needling shows that acupuncture stimulates the contralateral side of the brain compared to tactile stimulation. We could infer that tactile stimulation sets off the left sides of the brain activations and SA stimulates contralateral parts of the brain.
In the upper (LI1, LI10) and lower (LV3, ST36) limb acupuncture group, we could see both sides of sublobes, the thalamus, right frontal lobe, and left inferior semilunar lobule activated before acupuncture and both sides of the occipital lobe, the lingual gyrus, the visual association cortex, and the right parahippocampal gyrus, the hippocampus, the limbic lobe, the left anterior lobe, the culmen, and the cerebellum activated (Table 2). To sum up, after ULLA activations in the left sublobe, the thalamus, and the frontal lobe disappeared and the bilateral occipital lobe, the lingual gyrus, the visual association cortex and the right parahippocampal gyrus, the hippocampus, the limbic lobe, the left anterior lobe, the culmen, and the cerebellum became more activated. It indicates that after pulling out the needles, the activations of the brain remain as in the SA group but in the ULLA group it showed more signal activations in various regions than the SA group or in case of tactile stimulation. Among the 4 acupoints, ST36 showed the signal activations in the occipital lobe, the visual association cortex, and the cerebellum, suggesting that ST36 has the strongest effect. On the other hand, the right parahippocampal gyrus, the hippocampus, and the limbic lobe were only activated because the left sides were offset, showing dominance only on the right sides. This is possibly explained as follows. Acupuncture at ST36 sends signals to the multiple levels at the occipital lobe and limbic systems. 26 Although we instructed the subjects not to open their eyes or move their eyeballs during the study, there is a slight chance that they might have moved their eyeballs toward the end of the session. The other acupoints in the ULLA group activated the prefrontal cortex, the insula, and the hippocampus, which possibly have a cognitive function and memory as well. 39,40
In comparing the SA and the ULLA groups, it may be concluded that the ULLA group had more activated areas doubled with tactile stimulation at the same acupoints, whereas in the SA group the effect of the left acupoints on the scalp and that of the right lower limb acupoints counterbalances each other, or further research is needed to see whether SA chiefly activated contralateral parts of the brain.
The sensory system of our body perceives and controls the organs against surroundings consciously and unconsciously. The sensory system consists of the exteroceptive sensation, the interoceptive sensation, and the proprioception sense. The exteroceptive sensation perceives stimuli or change from surroundings such as pain, temperature, position, and touch. Thus, stimuli such as acupuncture and tactile stimulation are perceived through receptors, which change mechanical, chemical, and optical energy into electronic signals and the generated action potential is transmitted to the central nervous system via the special sensory route. Various outer stimuli are perceived by respective sensory receptors or sensory end organs and via peripheral nerves reaching the central nervous system, the dorsal root ganglia, the spinal cord, the brain stem, the thalamus, and the cortex.
Tactile stimulation on the upper and lower limb synapses at the nucleus cuneatus and nucleus gracilis of the medulla, respectively. Then the secondary afferents cross on the other side of the brain via the internal arcuate fiber and synapse in the thalamus (ventroposterolateral [VPL] nucleus) via the medial lemniscus, which ascends all the way through the brainstem to the primary somatosensory cortex through the posterior limb of the internal capsule.
SA travels through the trigeminothalmic pathway on the fifth cranial nerve, and its first sensory neuron is in the gasserian (semilunar) ganglion. The axon from here enters the ipsilateral pons and travels down to C2 along the spinal trigeminal tract and synapses with the second neuron, which is the spinal trigeminal tract nucleus at various places. Then it ascends to the other side of the brain to synapse with the ventral posteromedial (VPM) nucleus in the thalamus and to the parietal lobe through the posterior limb of the internal capsule. This study shows the contralateral (right side) parietal lobe, and postcentral gyrus activated (Table 1).
In addition, the ULLA needling can be considered the spinothalamic pathway of the anterolateral system. The pathways that pain, temperature, and nondiscriminative (light, crude) touch are transmitted by are called the anterolateral system, and it has the direct and the indirect pathway. The direct pathway, the (neo)spinothalamic pathway, is clinically important because localized pain and temperature are directly transmitted to the cerebral cortex from the spinal cord through the thalamus. Pain, temperature, and nondiscriminative touch from the contralateral upper limb, lower limb, and trunk are being passed on, and all the receptors have free nerve endings. This (neo)spinothalamic pathway runs for 2 to 3 segments after the nociceptor (pain receptor) signal enters the posterlateral fasciculus (Lissauer tract) of the spinal cord through the Aδ fiber. One segment heading downward synapses with the interneuron and is involved in the segmental spinal reflex. The other heading upward synapses at the second neuron in the dorsal horn, goes through the ventral white commissure, ascends to the thalamus (VPL nucleus) through the contralateral white matter. When the SA group and the upper and lower limb group were compared, the latter was shown to follow this route because the left frontal lobe, the precentral gyrus, the postcentral gyrus, the subcentral area, the parietal lobe and the right parietal lobe, the postcentral gyrus, and the primary somatosensory cortex including insula were activated (Table 3).
When we compared results between before and after acupuncture, the ULLA group showed activations in the cerebellum, the occipital lobe, the visual association cortex, the limbic lobe, the hippocampus, and the posterior lobe (Table 2). This can be explained by the following two theories: that the subject could have moved her eyes or acupuncture has something to do with the spinocerebellar tract. The unconscious proprioception is conveyed through the dorsal and ventral spinocerebellar tract to the cerebellum and engages in the unconscious control of posture and movement. This comes from the neuron in the intermediate gray matter of the spinal cord and has a fast conduction speed through wide-diameter fibers. Information from the lower limb is transmitted to both sides of the cerebellum. The dorsal spinocerebellar tract and the cuneocerebellar tract deliver the proprioception and the exteroceptive signal generated in the muscle to the cerebellum and control the feedback of fine motor control through the cortical and the subcortical motor nucleus. Therefore, we could observe both sides of the cerebellum activations after acupuncture needling, and further research is required.
Conclusions
In conclusion, when the 4 acupoints were tactile stimulated, it was received bilaterally in the brain but showed dominance in the contralateral side of the brain. It is consistent with the functions of high cerebral cortex. On tactile stimulation at ST36, various locations such as the frontal lobe, the parietal lobe, the posterior lobe, and the cerebellum as well as the inter-hemispheric showed activations. In the SA group it showed more activation after acupuncture to prove the stimulation remains even after pulling out the needles. The left SA activated the right side of the brain. The left SA activated the right side of the brain, which can be explained as signifying that the left side of the brain activation could have been offset by tactile stimulation or that acupuncture activated the brain contralaterally. It also showed brain activations after the needles were pulled out in the ULLA group, and the typical contralateral activations were different from those with tactile stimulation.
This study is different from the previous study, which focused on the parts of the brain activated after a specific acupoint was needled 24 –29,41 in that it had tactile stimulation at the 4 acupoints before and after SA and ULLA, respectively, and observed the effects of acupuncture after pulling out the needles and the difference of brain signal activations between the two groups. Thus, we excluded the data of each acupoint's brain activity in this article.
On a final note, the LI1 acupoint showed contralateral and bilateral activations, particularly in the limbic lobe, and the anterior cingulate to show that LI1 may have aroused emotional stimulation caused by strong pain. In the upper and lower limb group, LI10 and LV3 did not show signal activation after the needles were pulled out in the limbic lobe, and the anterior cingulate where it controls fear and instinct, 40,42 thus showing a need for further research on a specific acupoint involving in the pain control mechanisms by suppressing the pain stimulus ascending to the brain through the descending analgesia circuit.
Footnotes
Acknowledgments
We would like to thank Ja-Young Gwak and Yun-Kyung Park for their time and efforts spent on this study. This research was supported by the Kyunghee University Research Fund in 2007 (KHU-20070622).
Disclosure Statement
All of the authors declare that no competing financial interests exist.