
Abstract
Objectives:
The purpose of this study was to evaluate the effectiveness of P6 acupressure on vertigo and neurovegetative symptoms, its possible interference with vestibular-ocular reflex (VOR), and its clinical usefulness during acute vertigo.
Materials and methods:
Two hundred and four patients, either affected by acute vertigo (n=124) or undergoing labyrinth stimulation (n=80), were randomly divided in two homogeneous groups: an experimental group A and a placebo group B. Each patient rated severity of vertigo and neurovegetative symptoms on a visuo-analogue scale ranging from 0 to 10, before and after bilateral placement of a P6 device. The latter was placed on the P6 acupressure point (appropriate placement) in Group A patients or on the dorsal part of the carpus (inappropriate placement) in the Group B patients. Furthermore, qualitative and quantitative nystagmus parameters were collected via recorded video-oculoscopy and electronystagmography.
Results:
Eighty-five percent of Group A patients reported improvement of symptoms, which was significant for neurovegetative symptoms, but not for vertigo. In contrast, only 11% of the Group B patients reported improvement. VOR analysis did not show any significant variation of qualitative and quantitative nystagmus variables.
Conclusions:
This study demonstrated that the P6 device is effective in improving neurovegetative symptoms in patients affected by spontaneous and provoked vertigo, without any interference with VOR. Given the low cost and lack of side-effects of the P6 device, its routine application is suggested for acute vertigo and during labyrinth stimulation.
Introduction
The point P6 Nei-Guan is one of the main points in acupuncture, and it is specific for nausea, vomiting, and digestive dystonia. 8 –25
Some authors have demonstrated that stimulation through P6 acupressure causes an increase of the electrical discharge in the dorsal motor nucleus of the vagus nerve in the brainstem and subsequently induces prolonged slow waves of gastric peristalsis with respect to the baseline as revealed by electrogastrography. The prolonged slow waves, together with decreased spike waves, reduce antiperistalsis, which is the cause of nausea and vomiting. 26,27 P6 acupressure is in essence prolonged acupuncture on the P6 point, which is located three fingerbreadths from the wrist crease on the volar surface of the arm between the palmaris longus and flexor carpi radialis. P6 acupressure is successfully used in treating sea and motion sickness, postoperative nausea and vomiting, chemotherapy-induced nausea, and hyperemesis gravidarum. 11 –25 With the exception of rare cases, the majority of results show positive outcomes without any side-effects or contraindications. 28 –30
Aim of the study
The aim of the present double blind randomized study was to evaluate the effect of P6 acupressure applied through the P6 Nausea Control SEA BAND® (Hinckley, England, U.K.) (P6 device), in patients affected by acute spontaneous or provoked vertigo. In particular, the study evaluated two specific topics: (1) the effect of acupressure on vertigo and neurovegetative symptoms related to the acute phase, and (2) the possible interference of acupressure with VOR.
Materials and Methods
Two hundred and eight patients (25–85 years old, 118 men and 90 women), examined at the Otolaryngology Department of the University of Rome “Tor Vergata” between January and November 2008, constituted the study group. Four subjects were excluded from the study due to unilateral vestibular hypofunction, leaving 204 for analysis.
All the subjects either suffered acute vertigo or underwent tests to evaluate vestibular function for clinical-diagnostic or forensic-medical aims. In particular, 108 patients were affected by paroxysmal positional vertigo (PPV) and 16 patients by vestibular neuronitis (VN), and 84 patients underwent labyrinth stimulation (LS) in order to evaluate the VOR either through caloric (40 patients) or rotatory (44 patients) stimulation.
According to a computer-generated randomization schedule, the patients were divided into two matched groups with regard to age, pathology, and cause of vertigo, with the same number of patients (n=102) per group: experimental group A and placebo group B. All patients were advised to not take anti-emetics, vestibular suppressants, anti-epileptics, antidepressants, or drugs that interfere with the central nervous system. All the patients gave their informed consent to participate to the study and were unaware of the possible effects of the treatment they were receiving.
Each patient was asked to subjectively evaluate the severity of vertigo and neurovegetative symptoms on a visuo-analogue scale (VAS) ranging from 0 to 10, before and after the bilateral placement of P6 device for 30 minutes. Our study considered a 10%–39% decrease in pre- and post-placement scores as a mild improvement of symptomatology, a 40%–59% decrease as a moderate improvement, a 60%–100% decrease as a strong improvement, and a less than 10% decrease as no improvement.
Furthermore, in order to evaluate any possible interference of acupressure on VOR, the nystagmus qualitative (morphology) and quantitative (frequency and angular velocity of slow phase) variables were analyzed through recorded video-oculoscopy (r-VO) and electronystagmography (ENG) before and after the bilateral placement of the P6 device. These evaluations were always collected by the same physicians (Team A) who were blinded to the groups throughout the study.
The P6 Nausea Control SEA-BAND is an elasticized cloth wristband with a convex plastic button that is worn against the skin. This device exerts constant pressure on the P6 point, which is located three fingerbreadths from the wrist crease on the volar surface of the arm between the palmaris longus and flexor carpi radialis.
The P6 device placement on the P6 acupressure point was defined as appropriate in Group A; placement on the dorsal part of the carpus, which is considered to have no effect on acupressure, was inappropriate in Group B. The P6 device placement was performed in both groups by the same persons (Team B), who were blinded to the study design (Fig. 1).
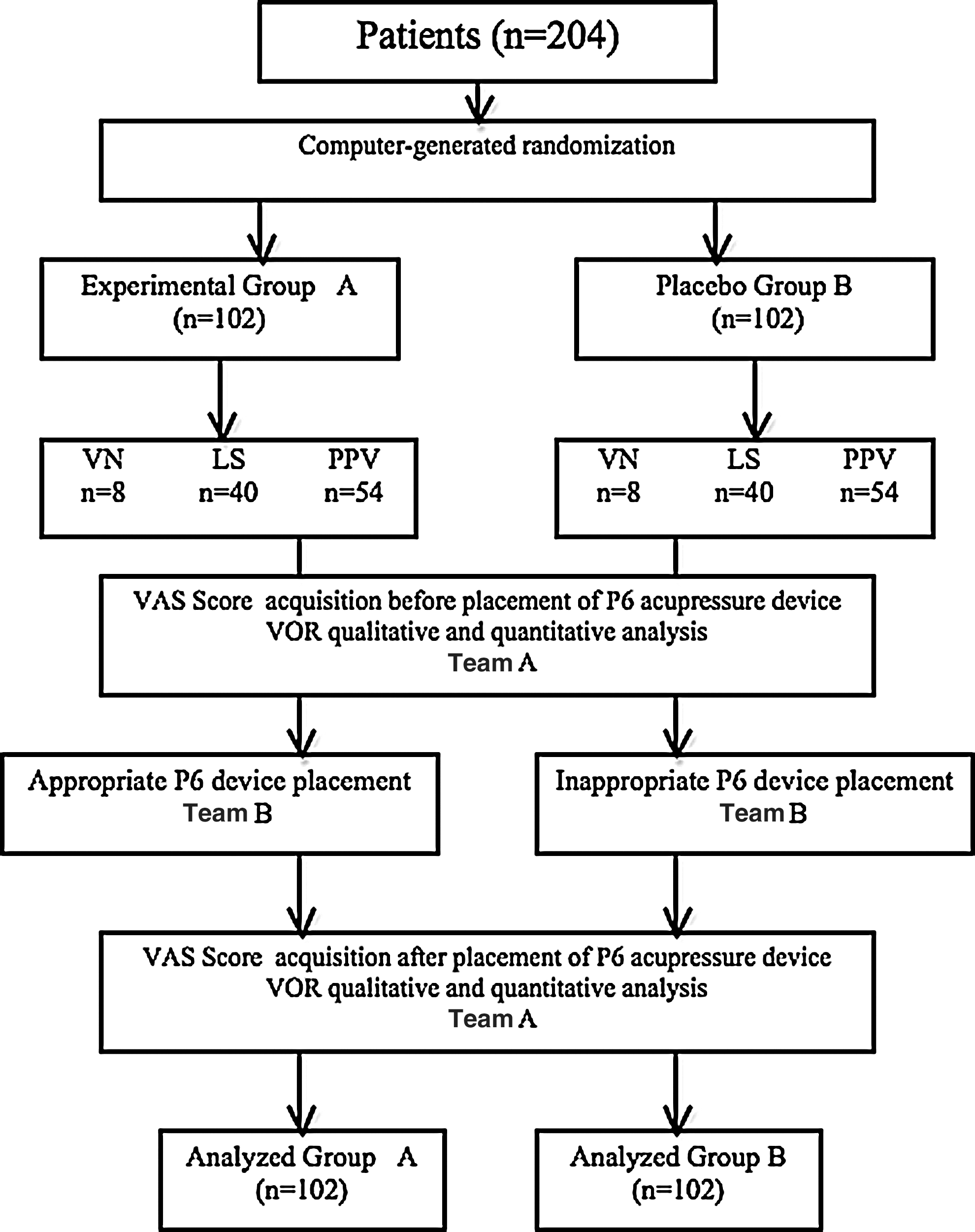
Flow diagram of participants in the study. PPV, paroxysmal positional vertigo; VN, vestibular neuronitis; LS, labyrinth stimulation; VAS, visuo-analogue scale; VOR, vestibular-ocular reflex.
The VOR and VAS evaluation was performed as follows. For PPV, the evaluation was performed once vertigo was provoked by positioning maneuver and after bilateral placement of the P6 device; VOR analysis included only its qualitative variations by means of r-VO. For VN, the evaluation was performed when the patient underwent physician examination and after bilateral placement of P6 device; VOR analysis included only its qualitative variations by means of r-VO. For LS, each patient first underwent bilateral labyrinth stimulation by caloric or rotatory test to confirm a symmetrical labyrinthine response, and a first evaluation was performed. As previously mentioned, four subjects were excluded from the study due to unilateral vestibular hypofunction. A second evaluation was performed, after 4–6 hours, when stimulation was repeated on one or the other side alternatively after bilateral placement of P6 device. VOR analysis included both qualitative and quantitative variations by means of r-VO and ENG.
The present study tested the null hypothesis (H0) that the VAS and VOR ratings of the two groups, after P6 device application, would not show any statistically significant difference. Significant cut-off level (α) was set at a p value of 0.01. Thus, p levels associated with the difference between the two groups were considered as statistically significant if lower than 0.01. Statistical comparisons were performed with paired t test (SPSS-Microsoft Windows, Chicago, IL, USA).
Results
Two hundred and four patients, 102 per group, were analyzed. Among the 102 patients of Group A, 85% reported an improvement of symptoms from mild to moderate, mainly with regard to neurovegetative symptoms rather than to vertigo; in contrast, only 11% of the 102 patients of Group B reported similar improvement. VOR analysis did not show any significant variation of nystagmus qualitative or quantitative variables in 99% of cases.
Paroxysmal positional vertigo
Group A patients
The evaluation of neurovegetative symptoms showed significant variation (p<0.01) between pretreatment (7.8±0.2) and post-treatment (5.8±0.5) VAS scores. The evaluation of vertigo showed nonsignificant variation between pretreatment (8.5±0.5) and post-treatment (8.2±0.3) VAS scores. The following pattern of neurovegetative symptoms improvement was reported by the 54 patients belonging to Group A: 38 patients (70%) reported a moderate improvement; 11 (20%), a mild improvement; and five (10%), no improvement.
Group B patients
Nonsignificant variation was shown between pretreatment and post-treatment VAS scores on the evaluation of both neurovegetative symptoms (7.5±0.4 versus 7.1±0.8) and vertigo (8.3±0.3 versus 7.7±0.2). The following pattern of neurovegetative symptoms improvement was reported by the 54 patients belonging to Group B: three patients (6%) reported moderate improvement; three (6%), mild improvement; and 48 (88%), no improvement (Fig. 2).
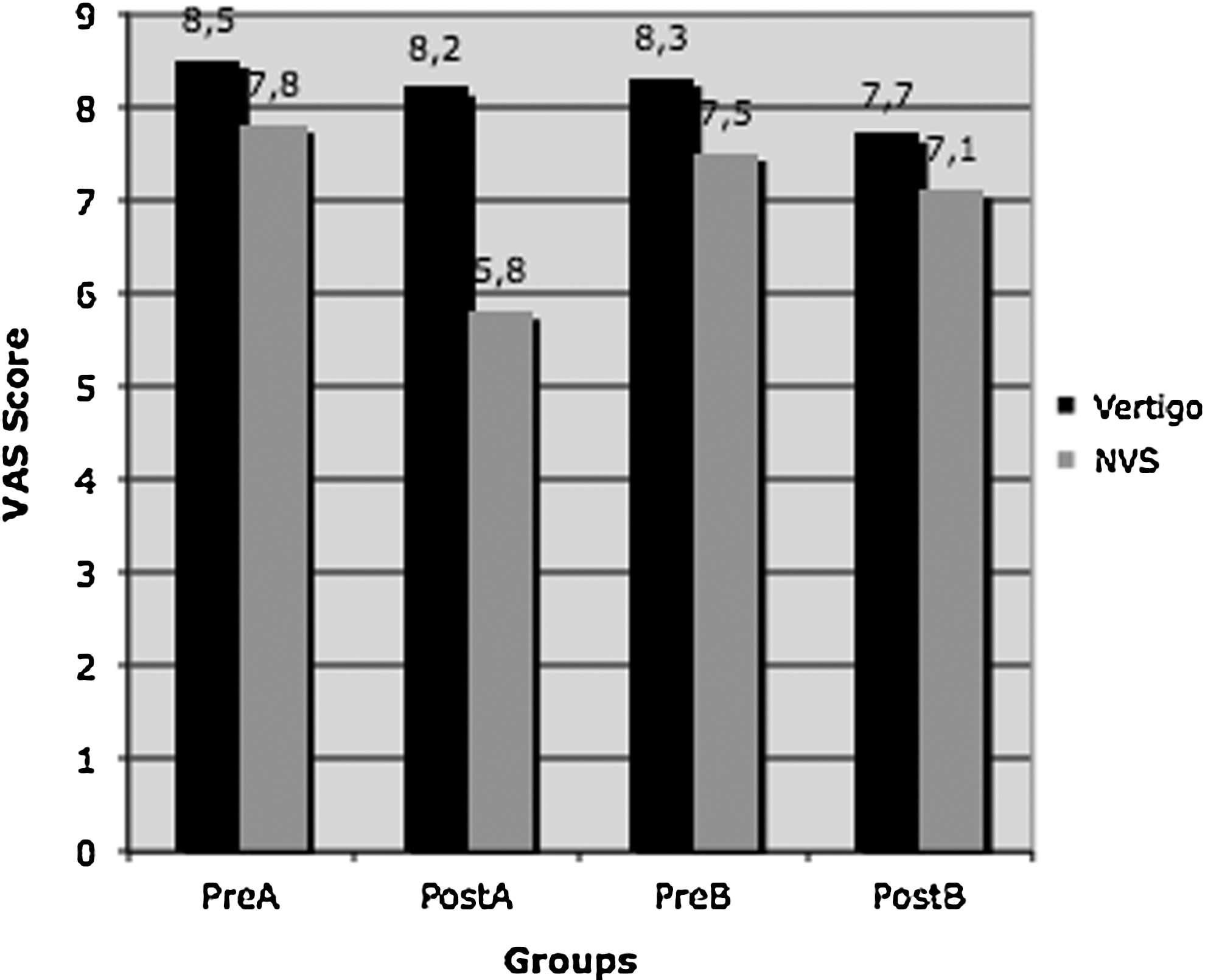
Visuo-analogue scale (VAS) score in paroxysmal positional vertigo. NVS, neurovegetative symptoms.
Analysis of qualitative parameters of VOR did not show a significant pre- versus post-treatment variation in either group (Table 1).
PPV, paroxysmal positional vertigo; VN, vestibular neuronitis; LS, labyrinth stimulation; VAS, visuo-analogue scale; VOR, vestibular-ocular reflex; NS, not significant; NF, not found.
Vestibular neuronitis
Group A patients
Although 75% of patients reported a mild or moderate improvement of neurovegetative symptoms, nonsignificant variation was shown between pretreatment and post-treatment VAS scores in the evaluation of both neurovegetative symptoms (7.9±0.2 versus 7.0±0.8) and vertigo (9.2±0.3 versus 9.1±0.1). The following pattern of neurovegetative symptoms improvement was reported by the eight patients belonging to Group A: two patients (25%) reported moderate improvement; four (50%), mild improvement; and two (25%), no improvement.
Group B patients
Nonsignificant variation was shown between pretreatment and post-treatment VAS scores on the evaluation of both neurovegetative symptoms (7.8±0.1 versus 7.2±0.5) and vertigo (9.3±0.4 versus 9.0±0.3). The following pattern of neurovegetative symptoms improvement was reported by the eight patients belonging to Group B: one patient (12.5%) reported moderate improvement; one (12.5%), mild improvement; and six (75%), no improvement (Fig. 3).
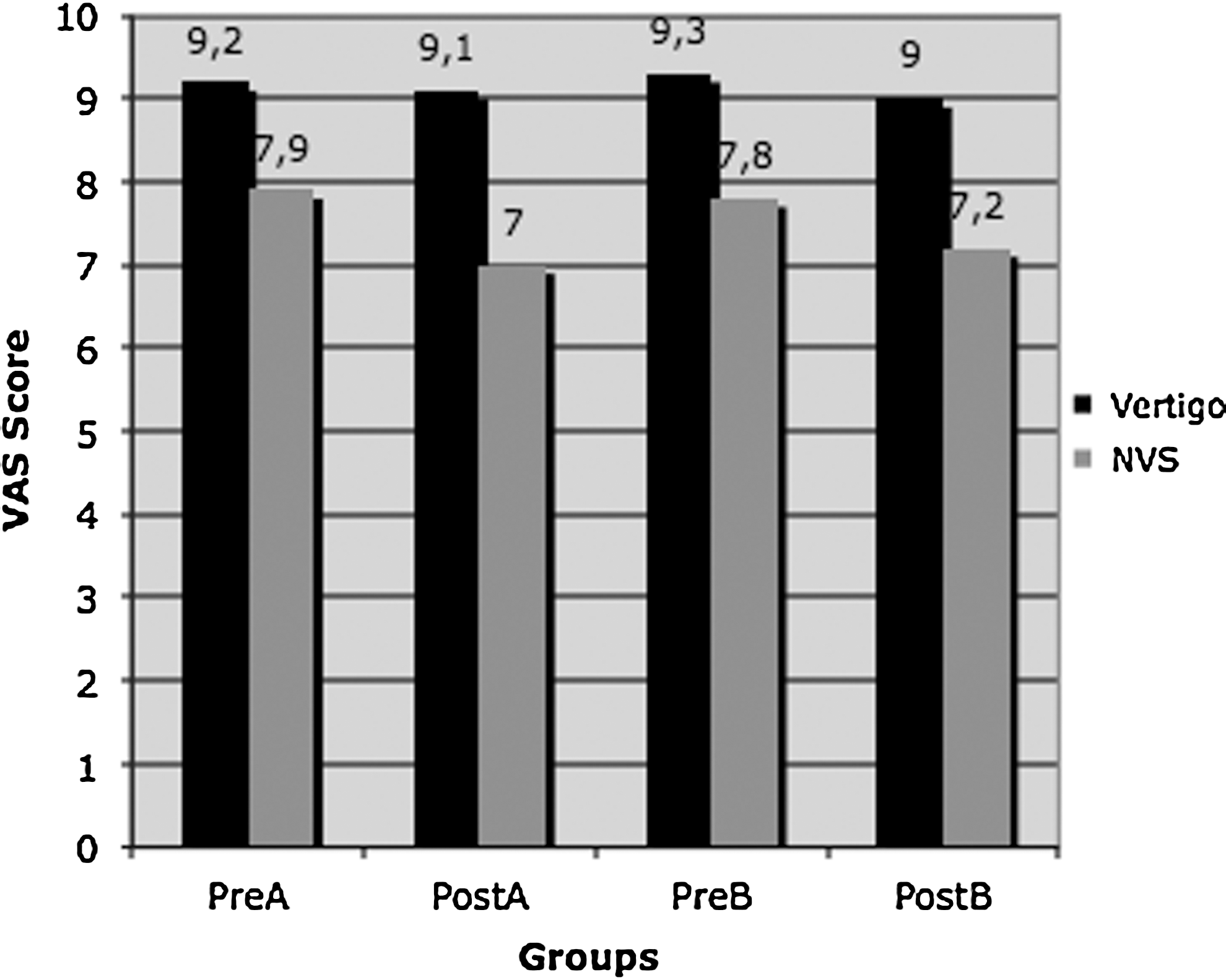
Visuo-analogue scale (VAS) score in vestibular neuronitis. NVS, neurovegetative symptoms.
Analysis of qualitative parameters of VOR did not show significant pre- versus post-treatment variation in either groups (Table 1).
Labyrinth stimulation
Group A patients
The evaluation of neurovegetative symptoms showed significant variation (p<0.01) between pretreatment (4.8±0.7) and post-treatment (2.5±0.6) VAS scores. The evaluation of vertigo showed nonsignificant variation between pretreatment (6.8±0.2) and post-treatment (6.1±0.7) VAS scores. The following pattern of neurovegetative symptom improvement was reported by the 40 patients belonging to Group A: 20 patients (50%) reported moderate improvement; 12 (30%), mild improvement; and eight (20%), no improvement.
Quantitative nystagmus parameters did not show any significant pre- versus post-treatment variation: in particular the mean slow phase velocity showed a pretreatment value of 22±0.8°/s and a post-treatment value of 22±0.4°/s; the frequency showed a pretreatment value of 1.2±0.5 beats/s and a post-treatment value of 1.1±0.3 beats/s.
VOR analysis showed significant pre- versus post-treatment qualitative variation in only two cases.
Group B patients
Nonsignificant variation was shown between pretreatment and post-treatment VAS scores in the evaluation of both neurovegetative symptoms (4.5±0.5 versus 4.1±0.4) and vertigo (7.1±0.3 versus 6.7±0.2). The following pattern of neurovegetative symptoms improvement was reported by the 40 patients belonging to Group B: three patients (6%) reported moderate improvement; one (4%), mild improvement; and 36 (90%), no improvement (Fig. 4).
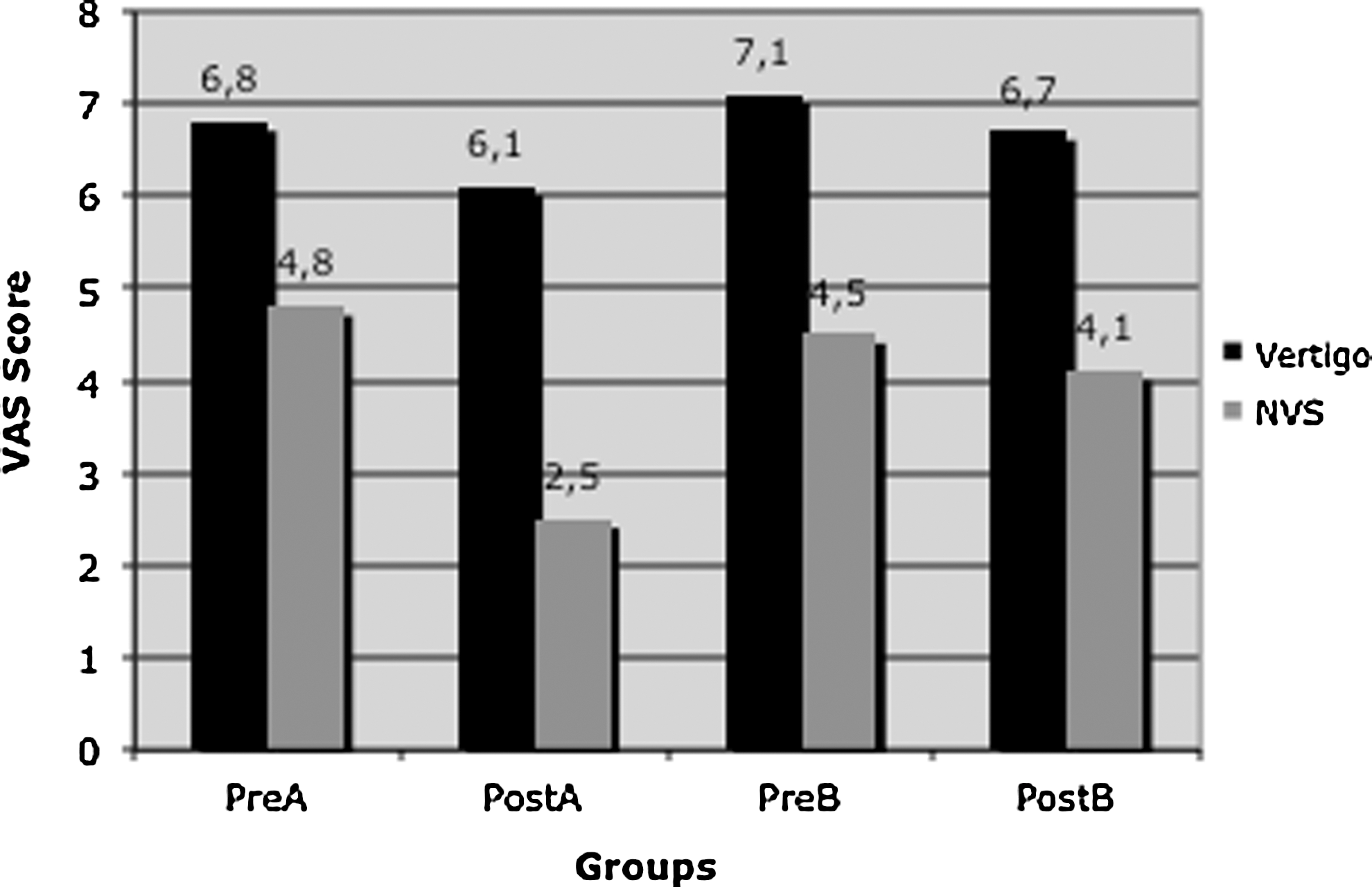
Visuo-analogue scale (VAS)score in labyrinth stimulation. NVS, neurovegetative symptoms.
Quantitative nystagmus parameters did not show any significant pre- versus post-treatment variation. In particular, the mean slow phase velocity showed a pretreatment value of 20±0.7°/s and a post-treatment value of 19±0.6°/s, and the frequency showed a pretreatment value of 1.1±0.6 beats/s and a post-treatment value of 1.1±0.5 beats/s.
VOR analysis showed no significant pre- versus post-treatment qualitative variations (Table 1).
Discussion
Medical therapy of vertigo can include causative, symptomatic, or preventive approaches. Vestibular suppressants, including anticholinergics, antihistamines, and benzodiazepines, provide symptomatic relief of distress by down-regulating vestibular excitability. Anti-emetics control nausea and vomiting by acting on the medullary vomiting center, the chemoreceptor trigger zone, or the gastrointestinal tract itself.
At present, general criteria for pharmacological therapy of vertigo suggest avoiding drugs that act on hypothesized but not verified causes of vertigo that are, at the same time, characterized by effects contrasting with recovery. Furthermore, a variety of drugs commonly used for symptomatic relief of vertigo and nausea have the major side-effect of general sedation, which interferes with vestibular reflexes and strongly reduces the reliability of the vestibular test. 2 –7
The present study evaluated the adequacy of treating symptoms related to vertiginous syndrome using acupressure on the P6 point. 8 –11 Our data showed that P6 device placement is associated with an overall improvement of clinical pattern for both vertigo and neurovegetative symptoms in PPV and LS patients.
Conversely, placement of the P6 device did not induce any significant variation of the clinical pattern in patients affected by VN, although 75% of patients reported a mild or moderate improvement of neurovegetative symptoms. In fact, as expected, it was possible to plan the treatment before the onset of symptoms in the PPV and LS patients. In contrast, VN patients usually presented several hours after the onset of symptoms and the P6 device could only be placed after symptoms had already started. The efficacy of acupressure was probably reduced by a desensitization of dorsal motor nucleus of vagus nerve, due to longer disease activity. 26,27
It can be hypothesized that P6 acupressure is more effective for treating neurovegetative symptoms than vertigo, because, unlikely the common antivertiginous drugs, it seems to behave as a modulator of the neural centers responsible for nausea and emesis genesis. In particular, as shown by electrogastrography, P6 acupressure increases the electrical discharge in the dorsal motor nucleus of the vagus and prolongs slow waves of gastric peristalsis with respect to the baseline, reducing antiperistalsis. 26,27
VOR analysis did not show any significant variation of quantitative nystagmus variables prior to and after bilateral placement of the P6 device in LS patients and showed variations of qualitative nystagmus variables in only two subjects. However, we believe that these variations, considering their type and low incidence, do not interfere with the analysis of results.
Conclusions
This study demonstrated that the application of the P6 device is useful in improving neurovegetative symptoms in patients affected by spontaneous and provoked vertigo. Furthermore, the device placement, unlike vestibular suppressant drugs, did not show any significant interference with VOR, allowing its application for the evaluation of vestibular function based on analysis of nystagmus. Particularly due to the low cost and lack of side-effects, routine application of the P6 device is suggested in acute vertigo and during labyrinth stimulation.
Footnotes
Disclosure Statement
No financial conflicts exist.