
Abstract
Objectives:
The acupoint GB20 is known to affect vertebrobasilar blood flow regulation. However, no previous study has used transcranial Doppler imaging to examine whether acupuncture at GB20 has a selective effect on blood flow in various cerebral arteries, such as the basilar artery (BA) and the middle cerebral arteries (MCAs). Therefore, this study sought to determine the specific effects of GB20 acupuncture on cerebral blood flow (CBF).
Materials and Methods:
Blood flow velocity and CO2 reactivity were measured by transcranial Doppler imaging with a 2-MHz pulsed Doppler probe observed through both temporal windows for the MCAs and through the suboccipital window for the BA before and after GB20 acupuncture treatment in 15 healthy young male volunteers. The changes in hyperventilation-induced CO2 reactivity and corrected blood flow velocities at 40 mmHg (CV40) were assessed for the BA and both MCAs. Blood pressure and heart rate were measured before and after the acupuncture treatment.
Results:
CO2 reactivity in the BA increased significantly after GB20 acupuncture treatment compared with baseline (p=0.041). In contrast, CO2 reactivity in both MCAs remained unchanged. The CV40 in the BA and the MCAs showed no change after the GB20 acupuncture treatment. The mean heart rate decreased significantly after the GB20 acupuncture, whereas the mean blood pressure showed no change.
Conclusions:
This study demonstrated that acupuncture treatment on GB20 increases CO2 reactivity specifically in the BA, with no effect in the MCAs. These results clinically support the use of GB20 to treat disorders of posterior cerebral circulation and support the idea that particular acupoints affect specific brain regions and cerebral arteries.
Introduction
A
It has been suggested that specific acupoints show acupuncture-induced increase of CBF in specific regions. 12 Previously, acupuncture at LI4–LI11 was reported to induce significant increases in regional CBF in both frontal lobes in healthy persons, as determined by using single-photon emission computed tomography; this finding differed from the results of electro-acupuncture on GB34–GB39, which showed significant increases in regional CBF in both temporal lobes. 13 –15 In addition, studies using TCD, which can measure blood flow velocity in intracranial arteries with high accuracy and monitor the real-time flow velocity, reported that specific acupuncture produced specific, quantifiable effects on blood flow velocity in arteries to the brain and eye. 12,16,17 Recent studies using TCD monitoring have also shown that GV20 acupuncture increased blood flow velocities in both the middle cerebral arteries (MCAs) and the anterior cerebral artery, an effect that is associated with improvements in vasomotor reactivity during hypocapnia in healthy persons. 18 However, no study appears to have used TCD monitoring to examine whether acupuncture at GB20 has a selective effect on blood flow in cerebral arteries, such as the basilar artery (BA) and the MCAs.
To determine the specific effects of GB20 acupuncture on CBF, the current study assessed changes in hyperventilation-induced CO2 reactivity and corrected blood flow velocities at 40 mmHg for the BA and both MCAs.
Materials and Methods
Participants
Fifteen healthy male volunteers were enrolled (mean age±standard deviation, 25.6±1.8; age range, 23–28 years). None of the participants had a history of cerebrovascular disease, cardiac disease, diabetes mellitus, hypertension, thyroid disease, or psychiatric problems. The participants were not allowed to drink alcohol or coffee, smoke, or take any medicine for 24 hours before the study. Each participant was informed of the procedures before the study. The Institutional Review Board at the Hospital of Korean Medicine, KyungHee Medical Center approved the study (KOMCIRB-2012–18).
Acupuncture at the GB20
The GB20 acupoint is located on the neck below the occipital bone, in the depression between the upper ends of the sternocleidomastoid and trapezius muscles. 19 One experienced acupuncturist performed all the acupuncture procedures. GB20 on the left side was treated with a stainless steel acupuncture needle (DongBang Acupuncture, Seoul, Korea; diameter, 0.25 mm; length, 4 cm). The needle was inserted into the skin to a depth of 2 cm at the GB20 acupoint toward the opposite eye. No other stimulations were performed throughout the procedure. The retention time of acupuncture was 20 minutes. 20,21
Measurement
The study protocol and method were based on our previous study. 18 Each participant took part in the study once per day on 2 separate days, 1 week apart. The CBF of both MCAs were measured on visit 1 and the BA was measured on visit 2 in a set order by TCD.
For the MCAs and BA, CO2 reactivity and blood flow velocity were measured by TCD using a Multi-Dop X4 system (Compumedics DWL, Singen, Germany). 18,22,23 Measurements were taken at rest and during 1-minute hyperventilation-induced hypocapnia. TCD was measured through both temporal windows on visit 1 for both MCAs and through the suboccipital window on visit 2 for the BA, using a 2-MHz pulsed-Doppler probe. To avoid shifting of the probe and to permit continuous measurements, a removable bilateral probe holder (LAM-Rack; Compumedics DWL) was attached for both temporal windows (Fig. 1) and a modified probe-holding device was attached for the suboccipital window (Fig. 2). The strongest available signal was sought at depths ranging from 45 to 60 mm for the MCA and 75 to 110 mm for the BA. The sample and gain values were adjusted to the value and recorded when the waveform of CBF was well maintained. All investigations started after the participants were stabilized for 5 min (Fig. 3). The participants were in the supine position during the MCA examination and in the sitting position during the BA examination. The mean flow velocity was calculated continuously as the time-averaged maximum velocity over the cardiac cycle, as computed from the envelope of the maximum frequencies. During continuous monitoring by a Cardiocap S/5 capnometer (Datex-Ohmeda, Helsinki, Finland), each participant was instructed to breathe normally until a steady state was reached. Mean MCA and BA blood flow velocities at rest were obtained in the stable normocapnic condition. The lowest mean blood flow velocities near the end of the hyperventilation period were then examined. All TCD spectra were recorded for later review.

Bilateral probe holder.

Suboccipital probe holder.

Timeline of study procedures. BP, blood pressure; HR, heart rate; TCD, transcranial Doppler imaging.
Because the blood flow velocity depends on the arterial CO2 tension, the corrected blood flow velocity was calculated at 40 mmHg of CO2 tension (CV40, cm/s) by the following formula:
24
where b is the CO2 reactivity, V1 is the velocity at P1CO2, and
CO2 reactivity refers to the percentage change in mean blood flow velocity per mmHg change in P
ETCO2
, as calculated by the following formula:
22
where V
rest
is the blood flow velocity during the most stable 10 seconds at rest in the stable normocapnic condition, V
hypocapnia
is the blood flow velocity during the most stable 10 seconds in the 1-minute period of hyperventilation, and
The variables that may control CBF were controlled using various modules of the Cardiocap S/5 collector (Datex-Ohmeda, Helsinki, Finland). Blood pressure was measured in a stable normocapnic condition before hyperventilation 3 times, with a 2-minute interval between the measurements to determine the mean blood pressure. The heart rate was continuously monitored by an oximetry apparatus positioned on the participant's finger. Further,
Using the above tools, before the GB20 acupuncture treatment for each participant, the blood pressure was obtained 3 times with a 2-minute interval between measurements. Simultaneously, pulse rate was continuously assessed during a 4-minute interval. CO2 reactivity and mean blood flow velocity were obtained before and after TCD measurement. After the 20-minute GB20 acupuncture treatment, the measurements were repeated (Fig. 3).
Analysis of data
Statistical analysis was performed with SPSS software for Windows, version 12.0 (SPSS, Inc., Chicago, IL). Statistical comparisons between the values before and after the GB20 acupuncture treatment were made with the Wilcoxon signed-rank test, and p<0.05 was considered to indicate a statistically significant difference. Data are summarized as mean±standard deviation.
Results
Fifteen healthy male participants were evaluated by using TCD (mean age, 25.6±1.8; age range, 23–28 years). To determine the effect of GB20 acupuncture, measured CO2 reactivity, CV40, blood pressure, and heart rate were measured. CO2 reactivity in the BA was significantly increased after GB20 acupuncture treatment compared with baseline (p=0.041). In contrast, CO2 reactivity in both MCAs was not significantly changed after GB20 acupuncture treatment (Table 1, Fig. 4). The CV40 in the BA and both MCAs showed no change after GB20 acupuncture treatment (Table 2). Mean heart rate decreased significantly after GB20 acupuncture, and mean blood pressure showed no change (Table 3).
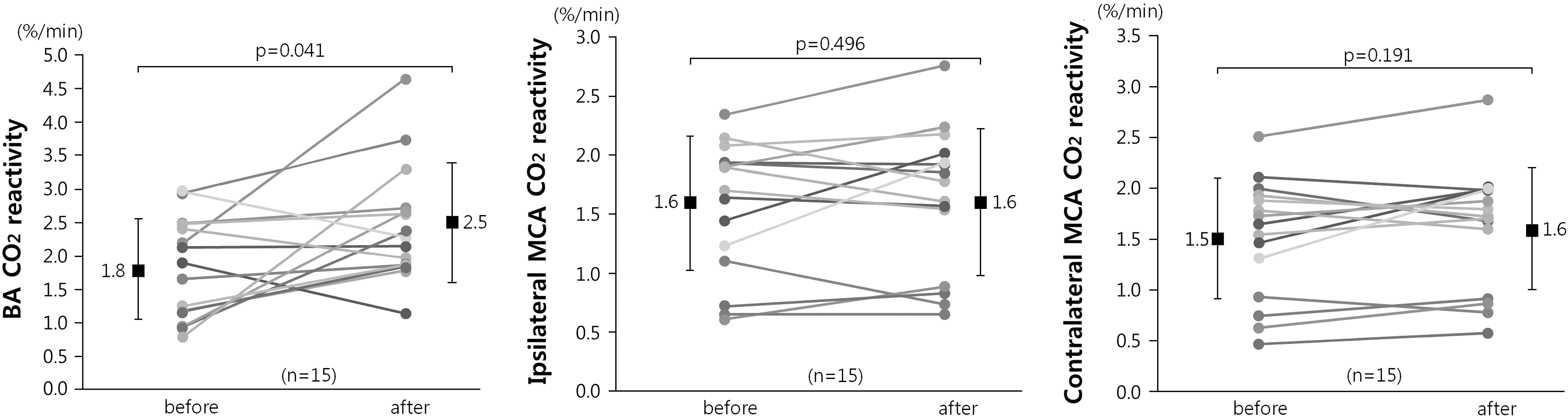
Changes in CO2 reactivity (%/min) in basilar artery (BA; left) and ipsilateral middle cerebral artery (MCA; middle) and contralateral middle cerebral artery (right) before and after GB20 acupuncture. (Wilcoxon signed-rank test, n=15.) CO2 reactivity in basilar artery significantly improved after the GB20 acupuncture (p=0.041). In contrast, the CO2 reactivity in both MCAs was not significantly changed after GB20 acupuncture treatment.
Values are mean±standard deviation.
By Wilcoxon signed-rank test.
CO2 reactivity, cerebrovascular reactivity to hyperventilation-induced hypocapnia; BA, basilar artery; MCA, middle cerebral artery.
Values are mean±standard deviation.
By Wilcoxon signed-rank test.
CV40, corrected blood flow velocities at 40 mmHg; BA, basilar artery; MCA, middle cerebral artery.
Values are mean±standard deviation.
By Wilcoxon signed-rank test.
Discussion
This study found that acupuncture treatment using TCD at GB20 on the left side increased CO2 reactivity selectively in the BA and had no effect on the MCAs. These results correspond with those of previous studies indicating that GB20 affects vertebral-basilar blood flow regulation. 9,10 The data support the theory that particular acupoints have effects only on specific brain regions and cerebral arteries. 12,16,17
TCD is an inexpensive, low-risk, and easy-to-administer bedside procedure. 25 Moreover, it enables measurement of CBF velocity in the main intracranial vessels noninvasively and with high accuracy. 26 By using a probe-holding device, the window, depth, and direction could be adjusted during the TCD monitoring to avoid shifting of the probe and permit continuous measurements. Although probe-holding devices for the anterior cerebral circulation system have already been developed, devices for the posterior cerebral circulation system are not yet common. In the past, examining the BA or vertebral artery using TCD involved holding the probe in the examiner's hand. This meant that the examiner's skill could greatly influence results. For this reason, studies have been conducted to develop a probe-holding device for the posterior cerebral circulation system. 25,27 Similarly, the suboccipital probe-holding device was modified for this study such that the probe could be in a fixed position during TCD monitoring. By using the modified suboccipital probe holder, more accurate and stable TCD spectra could be obtained.
Cerebral vasomotor reactivity is used to evaluate the compensatory potential of the vessels regulating blood flow to the brain and is represented as the percentage change in response to an arteriolar-dilating stimulus, such as CO2 or acetazolamide. 25,28,29 This study used hyperventilation-induced hypocapnia to measure CO2 reactivity. 22 –24 The increased CO2 reactivity in the BA can be explained by the improvement of endothelial function. Acute electro-acupuncture stimulation has been reported to notably improve neurologic function and vestibulomotor function. 30 In addition, one study showed that endothelial dysfunction was improved by acupuncture treatment. Endothelial dysfunction is characterized by a shift in the actions of the endothelium toward reduced vasodilation, a proinflammatory state, and prothrombic properties. It represents an important early event in the development of atherosclerosis and may serve as a useful independent predictor of stroke and cardiovascular disease. 31 –34 Endothelial nitric oxide synthase plays an important role in regulating endothelial function 35 and is one of the most important vasodilating factors. Acupuncture improves the synthesis of endothelial nitric oxide. 36 Increased levels of endothelial nitric oxide after acupuncture treatment improve endothelial dysfunction and lead to an increase in CO2 reactivity. Thus, acupuncture treatment might be directly applied to prevent stroke.
Sympathetic nervous system has a role in regulation in CBF. Innervation of vessels by sympathetic nerve fibers originating from the sympathetic ganglia is considered a main pathway of regulation. Cervical sympathetic ganglion block also shows an increase in CBF. 37 As classically proposed in the gate theory of Melzack and Wall, activation of myelinated fibers can produce inhibitory effects of the transmission of impulses in the small unmyelinated primary afferent fibers via the inhibitory circuits at the superficial laminae of the dorsal horn. 38 Previous nerve block studies have asserted that acupuncture can have a neuronal modulatory effect via segmental and/or suprasegmental mechanisms on noxious peripheral afferent inputs, largely mediated through the myelinated fibers. 39,40 Thus, it is also assumed that acupuncture at GB20 inhibits sympathetic input from the cervical ganglia to the cerebral arteries and leads to an increase in CO2 reactivity.
Previous studies have suggested that particular acupoints affect only specific brain regions and cerebral arteries. 12,16,17 The defined acupoints are considered important because the classical theory of traditional Oriental medicine claims that targeting an acupoint results in a clinical effect and that the stimulation of different acupoints results in different effects. 1,41 –43 Previously, acupuncture at acupoints LI4–LI11 was reported to induce significantly increased regional CBF. 13,14 Another study showed that electro-acupuncture at acupoints GB34–GB39 increases regional CBF in both temporal lobes. 15 Hence, the present study measured not only the BA but also both MCAs to analyze the specific regional effect on CBF. GB20 acupuncture showed a specific effect on the BA and not on the MCAs. These results correspond with previous studies showing that GB20 affects vertebral-basilar blood flow regulation. 9,10 However, those studies were conducted with several acupoints in addition to GB20, whereas this study focused on GB20 alone. Furthermore, some studies have shown that ipsilateral cerebral regions may be affected by acupuncture. 14,44,45 To compare the effects between the ipsilateral and contralateral MCAs, CO2 reactivity was measured in both MCAs simultaneously. However, no differences were found between the MCAs. The specific effect of GB20 acupuncture on the BA can be explained by a redistribution of CBF. 13,46 According to previous studies, brain areas were both activated and deactivated by acupuncture treatment. 13,41 The treatment may redistribute CBF to a specific area. Therefore, increased CO2 reactivity in the BA may be a result of the coordination and redistribution of CBF from other cerebral circulatory regions. This indicates an important finding of the current study: the idea that each acupoint may have specific effects. Furthermore, these results clinically support the use of GB20 to treat disorders of posterior cerebral circulation, such as stroke and vertebrobasilar insufficiency.
The change in CV40 was not significant in the BA or the MCAs after the acupuncture treatment on GB20. In previous studies, acupuncture treatment with continuous stimulation, such as electro-acupuncture or physical manipulation, had an effect on CBF. 14,15,18,30,41 Presence of acupuncture manipulation accompanied with de qi sensation was more closely linked to the induction of brain hemodynamic responses compared with acupuncture without manipulation. 21 Further, a comparison of brain perfusion images from superficial acupuncture and electro-acupuncture groups showed a significant difference in the increased perfusion area. 13 Simple acupuncture without manipulation provides stimulation that is relatively weak compared with that generated by electro-acupuncture. For this reason, we assume that the stimulation may be insufficient to affect CBF velocity.
The mean heart rate was significantly decreased after GB20 acupuncture treatment. It has already been reported that acupuncture induces heart rate reduction. 20,38,47 This is assumed to be a result of acupuncture-induced suppression of cardiac sympathetic activity. 48,49 Acupuncture produces a decrease in heart rate by activating gamma-aminobutyric acid–ergic neurons in the brainstem and inhibiting sympathetic outflow to the heart. 20,37 Furthermore, it is suggested that activation of parasympathetic cholinergic system by acupuncture leads to heart rate reduction. 38
One limitation of the current study was the limited sample size. Further studies with more participants may be required to confirm the present findings. Another limitation was the absence of a sham acupuncture control group. It was not possible to apply sham acupuncture on GB20 because hair disturbed the adhesion. However, because both MCAs and BA were measured in each participant by TCD and the CO2 reactivity was increased only in BA, both MCAs could be suggested as the control of the BA. Future studies should also address the reason the change in CV40 was not significant.
Conclusions
In conclusion, this study demonstrated that acupuncture treatment at GB20 increases CO2 reactivity specifically in the BA, with no effect in the MCAs. This is important evidence that each acupoint may have a specific effect on CBF. Furthermore, these results clinically support the use of GB20 to treat disorders of posterior cerebral circulation, such as stroke and vertebrobasilar insufficiency.
Footnotes
Author Disclosure Statement
No competing financial interests exist.