
Abstract
Background and Objective:
Patients in critical care settings often require prolonged mechanical ventilation (MV) therapy and, occasionally, they cannot be weaned from MV. The authors evaluated the efficacy of acupuncture treatment for improving the respiratory status and promoting successful weaning from prolonged MV in patients at intensive care units (ICUs).
Design:
Retrospective observational study.
Setting:
Gifu University Hospital, Gifu, Japan.
Subjects:
The authors included 16 tracheostomized patients receiving MV for >21 days at the ICU of Gifu University Hospital, who underwent acupuncture therapy for improving their respiratory status.
Intervention:
Acupuncture treatment was conducted in four sessions per week.
Outcome measures:
The data of tidal volume (VT), respiratory rate (RR), heart rate (HR), oxygen saturation as measured by pulse oximetry (SpO2), dynamic lung compliance (Cdyn), rapid shallow breath index (RSBI; RR/VT) values before and immediately after acupuncture were extracted from the medical records.
Results:
The median number of days on MV before acupuncture initiation was 31 days. VT and Cdyn were significantly increased immediately after acupuncture (all p < 0.001), whereas RR, HR, and RSBI were significantly decreased (all p < 0.05). Eleven patients were successfully weaned from MV after acupuncture initiation. In the weaning success group, VT and Cdyn were significantly increased (all p < 0.01), whereas RR, HR, and RSBI were significantly decreased (all p < 0.05) after acupuncture. Conversely, in the weaning failure group, these values were not changed significantly. The increase in Cdyn after acupuncture was larger in the weaning success group than in the weaning failure group (p < 0.05).
Conclusion:
Acupuncture treatment might have beneficial effects on the respiratory status of ICU patients receiving MV and may help in weaning from prolonged MV. Further large prospective cohort studies are warranted.
Introduction
P
To establish strategies for promoting successful weaning from MV and improving the respiratory status to discontinue MV therapy is important in the management of ICU patients because prolonged MV therapy involves risks of several ventilator-associated events, including ICU-acquired weakness 5 and ventilator-associated pneumonia (VAP), which are closely associated with increased morbidity and mortality. 6,7 In addition, ICU patients who receive MV are reported to have longer ICU and hospital stays compared with those who do not receive MV. 2 MV has also been associated with significantly higher daily costs for patients receiving ICU treatment. 2 Particularly, the expenses of patients who require prolonged MV have been reported to account for >50% of total ICU costs in the United States. 8,9
Recently, acupuncture treatment and acupuncture-point stimulation therapy have been reported to be effective for improving the respiratory status of patients with lung disease 10 –13 in the following ways: by reducing dyspnea, increasing respiratory muscle strength, improving the mobility of the rib cage, increasing β-endorphin levels, increasing forced expiratory volume in 1 sec, and improving exercise tolerance. Furthermore, the beneficial effects of acupressure on dyspnea and respiratory rate (RR) in patients receiving MV therapy in ICUs have been reported. 14 Acupressure has also been reported to improve the indices related to weaning, including the tidal volume (VT) and rapid shallow breath index (RSBI; i.e., the RR/VT ratio), in patients in a coma. 15 A preliminary retrospective review of a small group of hospitalized infants reported that some infants requiring MV were successfully weaned after acupuncture using press needles and acupressure using magnets, although the detailed data of respiratory conditions improved with acupuncture were unavailable. 16 However, to the best of knowledge, no reports have demonstrated the effects of acupuncture on the respiratory status in adult patients receiving prolonged MV therapy in the ICU.
The authors hypothesized that acupuncture is also beneficial for improving the respiratory parameters related to weaning from MV in patients receiving prolonged MV in ICU settings. For several years, they have been treating patients receiving MV in the ICU of their hospital with acupuncture to improve their respiratory status. The aim of this study was to investigate the effects of acupuncture for improving the respiratory status in ICU patients receiving prolonged MV, through a retrospective chart review.
Subjects and Methods
Study design and ethical approval
This retrospective observational study was performed using medical records (chart review) from April 2008 to March 2015. This study was performed at the Advanced Critical Care (ACC) center, which is the ICU section of Gifu University Hospital, Gifu, Japan. This study was approved by the Ethics Committee of Gifu University Graduate School of Medicine and was conducted in accordance with the Declaration of Helsinki.
Participants
Patients with respiratory failure, who were maintained on prolonged MV at the ACC center of Gifu University Hospital and who received acupuncture for improving their respiratory status and for helping them to wean from MV, were included in this study. In this clinical situation, the patients with prolonged MV received acupuncture in addition to standard treatment when they could not be weaned after 2 weeks or had difficulties in weaning due to abnormalities in traditional weaning parameters 17,18 such as low VT, high RR, high VT/RR ratio, and hypoxemia, although the criteria for acupuncture commencement were not very strict. For the consideration of prolonged MV, patients who received MV for >21 days before acupuncture initiation were included in this study.
Acupuncture treatment
For acupuncture treatment, standard acupuncture points, including LU1, LI4, ST36, CV12, KI3, and CV4 (Fig. 1), were used. The detailed locations of these points were determined in accordance with the World Health Organization standard textbook. 19 These acupuncture points were mainly chosen with reference to previous reports describing the effects of acupuncture on dyspnea in patients with chronic obstructive pulmonary disease (COPD) 20 and clinical experiences. 21 LI4 was used because it has been reported to reduce dyspnea and RR. 14,22 LU1, CV12, and CV4 were also selected because these points are close to the respiratory accessory muscles, including the pectoralis major and minor muscles and rectus abdominis muscle. The authors also considered the concepts of modulation of qi energy of the lung and kidney and the yin/yang energies in Traditional Chinese Medicine (TCM) theory, according to which they presumed that respiratory failure is mainly induced by the deficiency of qi and yang energy and dysfunction of the lung, kidney, and spleen. LI4 and ST36 were used for increasing qi energy. LU1 and KI3 were used for modifying lung and kidney dysfunction according to the TCM theory.
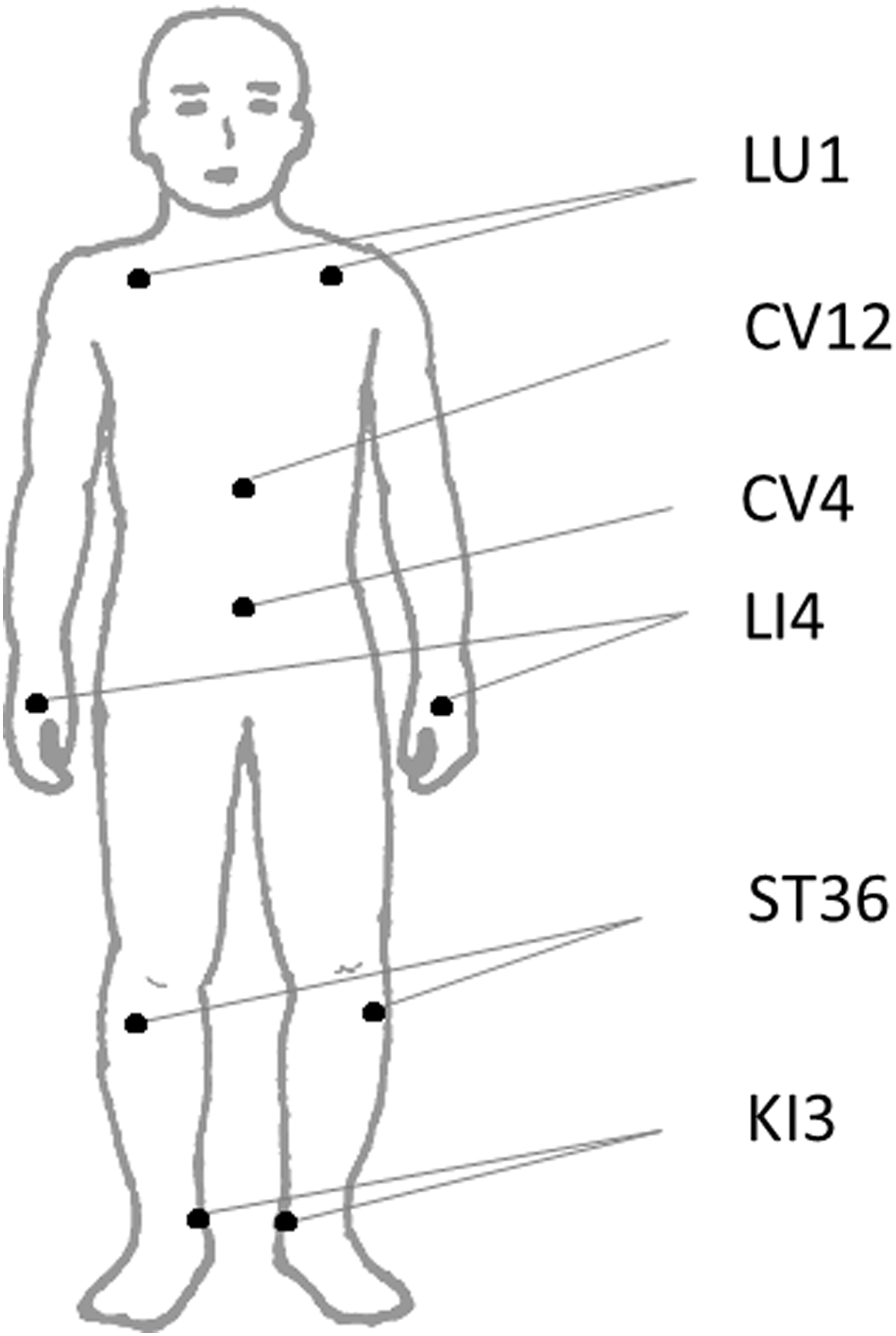
Mainly used acupuncture points.
In addition to the standard acupuncture points, the following supplementary points were used: GV20, Ex-HN3, CV 17, SP9, ST19, CV6, LI11, and LR3. CV6 was used instead of CV4 when CV4 was hiding under clothes and diaper. SP9 was used for modifying the sputum according to the TCM theory in cases of severe edema, sputum production, and pleural effusion. LI11 was used when fever developed. GV20, Ex-HN3, and Liv3 were added for patients who were agitated because these points have been used for mental disorders and sedation according to the TCM theory, previous reports, 23,24 and the authors' clinical experiences. 25 GV20 was also used for increasing qi energy based on the TCM theory. CV17 was used for modifying qi energy. ST19 was used for attenuating hypertonus and fatigue of the rectus abdominis muscle, which is an accessory respiratory muscle. Acupuncture points used were also chosen based on the posture of the patients, with the avoiding of catheters or intravenous feeding tubes and the locations of burns and operative scars.
A Japanese-style gentle needle technique was employed. Disposable sterilized stainless steel acupuncture needles (0.16 mm in diameter, 40 mm in length; SEIRIN, Shizuoka, Japan) were gently inserted to a depth of 4–20 mm, depending on the thickness of the skin and subcutaneous fatty tissue, and were left for 10 min without manipulation. At LU1, the acupuncture needle was inserted up to 3–7 mm almost horizontally to avoid the possibility of pneumothorax. Acupuncture treatment was conducted in four sessions per week by an experienced acupuncturist who had a Masters degree in acupuncture and clinical experience of at least 8 years.
Outcome measures
The data related to weaning from MV were extracted from medical records. The data regarding diagnosis; reasons for admission to ICU and MV therapy; Acute Physiology and Chronic Health Evaluation (APACHE) II score, which is a severity of disease classification system 26 ; duration of MV therapy; MV settings, including MV mode, fraction of inspiratory oxygen (FIO2), positive end-expiratory pressure (PEEP), pressure support (PS) before acupuncture initiation, and success or failure of weaning after acupuncture initiation; VT; RR; heart rate (HR); oxygen saturation as measured by pulse oximetry (SpO2); dynamic lung compliance (Cdyn), calculated as VT/(peak inspiratory pressure − PEEP); and RSBI ( = RR/VT), which was measured during 1-min observation before and immediately after 10 min of acupuncture treatment were also extracted. The values of these variables before and after 10 min of acupuncture treatment were extracted from the data of the day when the patient was receiving MV, and the maximum change in VT was observed within the first week after the commencement of acupuncture treatment (i.e., within the first four acupuncture sessions). The data of the days when the ventilation settings, medications, or patients' posture were changed during an acupuncture session were excluded from data collection because these changes might have influenced the patients' respiratory status. The data of the days when ventilation was removed for spontaneous breath trials (SBTs) during an acupuncture session were also excluded because the data of MV parameters were unavailable.
For secondary analysis, the participants were divided into two groups based on weaning success or failure. Weaning success was defined as the discontinuation of MV for >24 h in an SBT. In the weaning success group, the number of days and acupuncture sessions needed to wean a patient from MV after the initiation of acupuncture was also extracted. Differences in VT, RR, Cdyn, HR, and RSBI before and after acupuncture in the weaning success group were compared with those in the weaning failure group. The length of ICU stays after acupuncture between both groups was also compared.
Statistical analyses
The primary variable was the change in VT and RR. The Shapiro–Wilk test was used to assess normal distributions. Parametric variables are expressed as mean and standard deviation (SD) or mean and 95% confidence interval (CI), whereas nonparametric data are reported as median and quartile (first and third). When the data were parametric in nature, the paired t test was used to compare variables before and after acupuncture or the unpaired t test was used for comparison between the weaning success and failure groups. When the data were nonparametric in nature, the Wilcoxon signed-rank test was used for the comparison between variables before and after acupuncture, and the Mann–Whitney U test was used for comparison between groups. For categorical variables, chi-square test or Fisher's exact test was used for comparison between groups. The statistical analyses were performed using SPSS ver. 22 for Windows (IBM SPSS). The strength of the findings regarding the differences between the weaning success and failure groups in terms of the changes from baseline values and between before and after acupuncture was determined by calculating the effect size r (
Results
Participants' characteristics at baseline
Twenty-six patients with MV received acupuncture treatment during the study period. Ten patients had to be excluded because their MV periods before acupuncture were <20 days. Accordingly, 16 patients were selected for this study, and their data were statistically analyzed. Patients' characteristics before acupuncture initiation are shown in Table 1. These patients received MV therapy for 31.0 (24.3, 40.7) [median (first, third quartile)] days before the commencement of acupuncture. Ventilation parameters before the commencement of acupuncture were as follows: FIO2, 0.30 (0.30, 0.35); PEEP, 5.4 ± 1.4 cmH2O; and PS, 7 (5, 7) cmH2O.
Data indicate the number of patients, mean ± SD, or median (first, third quartile). p-Value: p-value between weaning success and failure groups.
APACHE, Acute Physiology and Chronic Health Evaluation; APRV, airway pressure release ventilation; CPAP, continuous positive airway pressure; FIO2, fraction of inspiratory oxygen; HR, heart rate; MV, mechanical ventilation; P/F ratio, PaO2/FIO2 ratio; PEEP, positive end-expiratory pressure; PS, pressure support; RR, respiratory rate; RSBI, rapid shallow breath index ( = RR/VT); SD, standard deviation; SIMV, synchronized intermittent mandatory ventilation; SpO2, oxygen saturation as measured by pulse oximetry; VT, tidal volume.
The reasons for admission were acute myocardial infarction (AMI; n = 3), trauma (n = 7), acute heart failure (AHF; n = 2), burns (n = 2), and aortic dissection (AD; n = 2). The reasons for initiating MV were pneumonia (n = 1), trauma (n = 7), AHF (n = 2), burns (n = 2), AMI (n = 2), and AD (n = 2).
All patients underwent the conventional weaning process, including pulmonary rehabilitation and reduction of PS and PEEP in MV settings. Twelve patients did not fulfill the criteria for SBT. In four patients, attempts were made to discontinue MV for just a few hours in the daytime for several days, using high-flow oxygen therapy or T-tube (T-piece) oxygen therapy through tracheostomy; however, they had to continue MV due to increased dyspnea, tachypnea, and desaturation. Five patients received biphasic cuirass ventilation therapy (RTX respirator; Medivent Ltd., London, United Kingdom) for 1–14 days. However, this therapy was discontinued after the second treatment session due to nausea and discomfort during the therapy in two of four patients in the weaning success group and after the tenth treatment session due to hypertension in one patient in the weaning failure group. One patient in the weaning failure group received anabolic steroid therapy for curing the weakness of the respiratory muscles.
The mainly used ventilator was Evita-4 (Drager Medical AG & Co. Lubeck, Germany). The Puritan Bennett 840 ventilator system (Puritan-Bennett Corporation, Pleasanton, CA) was used in two patients, and Servo–i Universal ver. 3.0 (SIEMENS ELEMA AB, Solna, Sweden) was used in one patient.
As supplementary acupuncture points, GV20 was used in 12 patients, EX-HN3 in 3 patients, CV17 in 6 patients, SP9 in 6 patients, ST19 in 3 patients, CV6 in 3 patients, LI11 in 2 patients, and LR3 in 1 patient.
Characteristics of participants in the weaning success and failure groups
Eleven patients were weaned from MV after acupuncture initiation. Five patients could not be weaned because one patient died due to acute respiratory distress syndrome and pulmonary fibrosis and the other patients were transferred to another hospital while receiving MV. Patients in the weaning success group received 6 (4, 6) sessions of acupuncture over 10.5 ± 4.8 days until weaning from MV. The weaning failure group received 12.4 ± 7.0 acupuncture sessions over 25.2 ± 15.0 days until they were moved from the ICU or died. The characteristics and physiologic data before acupuncture was started in the weaning success and failure groups are also shown in Table 1. There were no significant differences in the variables of participants' characteristics except for RSBI (Table 1). RSBI was smaller in the weaning failure group than in the weaning success group (p = 0.049), although the values in both groups were <105 breaths/min/L, which is a useful value for weaning.
The length of ICU stays after acupuncture started tended to be shorter in the weaning success group than in the weaning failure group. This difference was not statistically significant [15 (9, 20) vs. 23 (22, 30) days; p = 0.196] although it presented a medium-sized effect (r = −0.35).
The reasons for hospitalization in the weaning success group were AMI (n = 2), trauma (n = 3), AHF (n = 2), burns (n = 2), and AD (n = 2) and for that in the weaning failure group were AMI (n = 1) and trauma (n = 4). The reasons for initiating MV in the weaning success group were trauma (n = 3), AHF (n = 2), burns (n = 2), AMI (n = 2), and AD (n = 2) and for that in the weaning failure group were pneumonia (n = 1) and trauma (n = 4). There were no significant differences in the reasons for admission (p = 0.423) and initiating MV (p = 0.218) between both the groups.
Immediate effects of acupuncture
The immediate effects of acupuncture on VT, Cdyn, RR, HR, SpO2, and RSBI are shown in Figure 2. These data were extracted after the second (first, third) [median (first, third quartile)] session of acupuncture treatment. On the day when these data were extracted, some MV settings were changed compared with those before acupuncture initiation; although these changes were not statistically significant they are as follows: 13 patients (weaning success, n = 10; weaning failure, n = 3) with continuous positive airway pressure mode; 3 patients (weaning success, n = 1; weaning failure, n = 2) with synchronized intermittent mandatory ventilation mode; FIO2, 0.32 (0.30, 0.35); PEEP, 5.0 ± 1.1 mmHg; and PS, 6 (5, 7) mmHg.
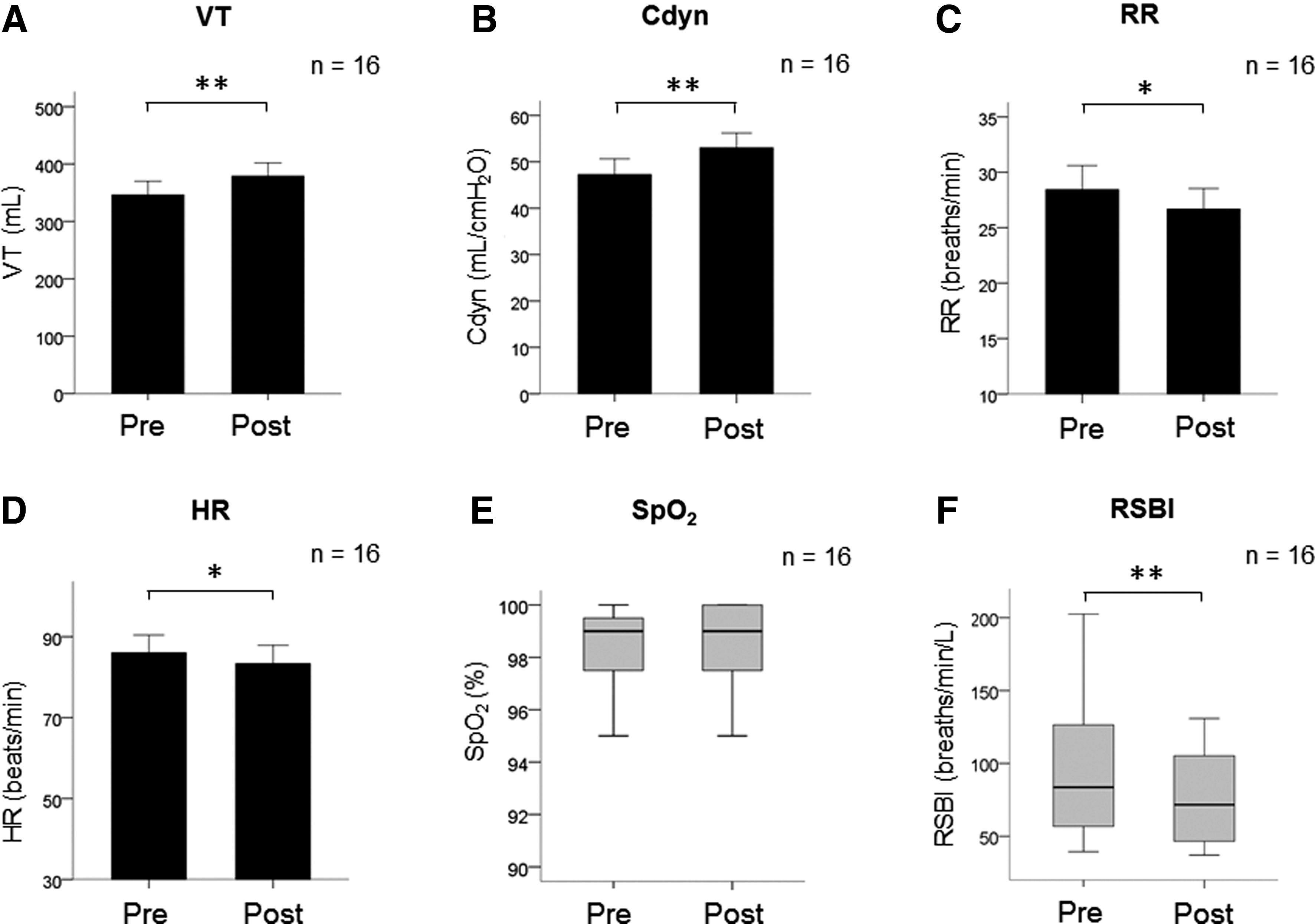
Immediate effects of acupuncture on VT
VT and Cdyn were increased significantly immediately after acupuncture [before vs. after, mean ± SD, 346.2 ± 95.0 vs. 379.0 ± 92.0 mL; mean difference (95% CI), 32.8 (18.9–46.7) mL; p < 0.001; r = 0.79 and 47.3 ± 13.5 vs. 53.0 ± 12.7; 5.7 (3.3–8.2) mL/cmH2O, p < 0.001, r = 0.79, respectively], whereas RR [28.4 ± 8.6 vs. 26.7 ± 7.4 breaths/min; −1.8 (−3.4 to −0.1) breaths/min; p = 0.035, r = 0.51] and HR [86.1 ± 17.4 vs. 83.4 ± 18.0 beats/min; −2.7 (−4.7 to −0.7) beats/min; p = 0.011, r = 0.60] were significantly reduced. There was no significant change in SpO2 [median (first and third quartile), 99% (98%, 100%) vs. 99% (98%, 100%); p = 0.750, r = −0.18]. RSBI was reduced significantly after acupuncture [83.6 (55.7, 128.4) vs. 71.6 (46.4, 105.5) breaths/min/L; p < 0.001; r = −0.80].
Comparison of changes in variables after acupuncture between both groups
MV settings and VT, Cdyn, RR, HR, and RSBI values before and after acupuncture in each group are shown in Table 2. There were no significant differences in VT, Cdyn, RR, HR, and RSBI immediately before acupuncture (p = 0.055, 0.418, 0.136, 0.660, and 0.052, respectively; Table 2). VT and Cdyn increased significantly after acupuncture in the weaning success group (p = 0.001 and 0.002, respectively), whereas the values in the weaning failure group did not change significantly (p = 0.137 and 0.125, respectively; Table 2). RR, HR, and RSBI were reduced significantly in the weaning success group (p = 0.028, 0.023, and 0.008, respectively), whereas these values were not significantly changed in the weaning failure group (p = 1.000, 0.313, and 0.313, respectively; Table 2).
Data indicate the number of patients, mean ± SD, or median (first, third quartile). After: immediately after 10 min of acupuncture treatment; before: before acupuncture.
p < 0.05, ** p < 0.01, versus before weaning success.
Cdyn, dynamic lung compliance; CPAP, continuous positive airway pressure; FIO2, fraction of inspiratory oxygen; HR, heart rate; MV, mechanical ventilation; PEEP, positive end-expiratory pressure; PS, pressure support; RR, respiratory rate; RSBI, rapid shallow breath index (= RR/VT); SD, standard deviation; SIMV, synchronized intermittent mandatory ventilation; VT, tidal volume.
The changes in VT, Cdyn, RR, HR, and RSBI in both groups are shown in Figure 3. The increases in Cdyn among patients who could be weaned were significantly larger than those among patients who could not be weaned [mean ± SD, 7.4 ± 4.7 vs. 2.2 ± 1.8 mL/cmH2O, mean difference (95%CI), 5.2 (0.5–9.9); p = 0.033; r = 0.53]. The increases in VT tended to be larger among patients who could be weaned than among those who could not; however, this difference was not statistically significant [37.8 ± 25.7 vs. 21.8 ± 26.2 mL, 16.0 (−13.9 to 45.9) mL; p = 0.269], although it presented a small-sized effect (r = 0.29). The reduction in RR tended to be larger among those who could be weaned than among those who could not be weaned; however, this difference was not statistically significant [median (first and third quartile), −1.0 (−3.5, 0) vs. 0 (0, 1.0) breaths/min; p = 0.054], although it did present a medium-sized effect (r = −0.48). There was no statistical difference between the reductions in HR between the weaning success and failure groups [−2.5 ± 3.2 vs. −3.0 ± 5.1 beats/min; −0.5 (−4.9 to 4.0); p = 0.830; r = 0.06]. The reduction in RSBI showed a tendency to be larger in the weaning success group than in the weaning failure group. This difference was not statistically significant [−13.8 (−18.9, −10.1) vs. −2.0 (−2.8, 0.6); p = 0.090], although it presented a medium-sized effect (r = −0.44).
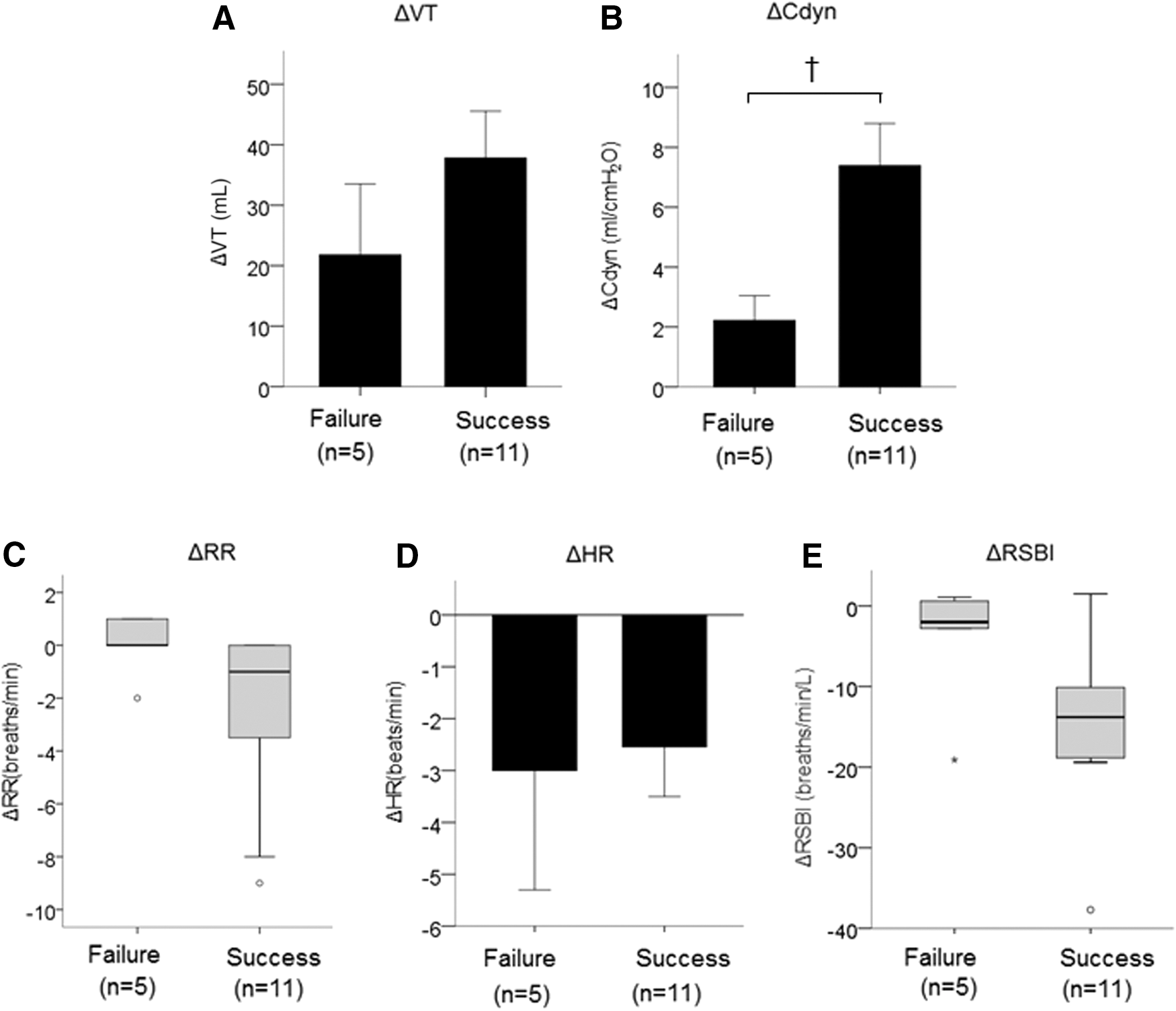
Comparison between the weaning success (n = 11) and failure (n = 5) groups in terms of the changes in VT
Adverse events
There were no adverse events due to acupuncture that required medical treatment.
Discussion
To the best of the authors' knowledge, this is the first study to indicate the beneficial effects of acupuncture on the respiratory status in adults with prolonged MV in ICU settings. VT and Cdyn increased significantly, whereas RR, HR, and RSBI decreased significantly immediately after acupuncture. Furthermore, these significant changes were observed in the weaning success group but not in the weaning failure group, and the increase in Cdyn was larger in the weaning success group than in the weaning failure group. Increase in VT and decrease in RR lead to a decrease in RSBI, and these indices were thought to predict weaning success because lower VT and higher RSBI were reported to be observed in ventilation-dependent patients. 18 In addition, not only VT and RR but also Cdyn, oxygenation, and maximum inspiratory pressure have been reported to be indices that predict weaning success. 28 According to these findings, acupuncture has beneficial effects on the respiratory parameters related to weaning from MV in patients with prolonged MV. Some of these findings were similar to the results of a previous study performed using acupressure. A reduction in dyspnea and RR, 14 increase in VT, and decrease in RSBI 15 after acupressure have been reported in patients with MV.
The increase in Cdyn after acupuncture might predict weaning success because a larger increase of Cdyn was observed in the weaning success group than in the failure group. Further prospective studies with a large sample size and homogeneous patient characteristics in each group are needed to establish the utility of this idea. Although the differences in increased VT and decreased RR and RSBI immediately after acupuncture between the weaning success and failure groups were not statistically significant, small- or medium-sized effects were presented. Thus, in future studies with a larger sample size, statistically significant differences might be found in these variables between both groups.
The mechanism of acupuncture effects could not be elucidated in this study. One of the important reasons for poor weaning outcomes is the weakness, as well as the fatigue, of respiratory muscles. 18,29 Furthermore, inspiratory muscle training has been reported to facilitate weaning from MV among patients in the ICU. 30 Acupuncture has been reported to increase respiratory muscle power in patients with COPD. 10,31 In addition, it was speculated that acupuncture induces the relaxation of accessory respiratory muscles because the rib cage range of motion and forced vital capacity were increased after acupuncture treatment in a previous report. 10 An increase of blood β-endorphin levels by using transcutaneous electrical nerve stimulation at acupuncture points has also been reported and is suggested to be associated with the reduction of dyspnea as well as the improvement of respiratory function, including FEV1. 13 Dyspnea and RR have also been reported to be decreased by the use of acupressure in ICU patients with prolonged MV. 14 Based on these findings, increased respiratory muscle strength, improved rib cage range of motion, and increased blood β-endorphin levels due to acupuncture might be associated with the reduction of dyspnea and increase of VT, which lead to a decrease of RR and weaning from MV. However, this is speculation because the authors did not measure the respiratory muscle strength, blood β-endorphin levels, and dyspnea levels in this study. Further study is required to elucidate the changes in these variables. HR was also statistically decreased immediately after acupuncture. Acupuncture has been reported to change the tone of the autonomic nervous system. 32,33 The reduction of the sympathetic tone or increase of the parasympathetic tone induced by acupuncture might be associated with the acupuncture effects observed in this study.
Acupuncture treatment might minimize the risks of several ventilator-associated events because of early weaning from MV. Additional controlled trials with no or sham acupuncture groups should be conducted to investigate the incidence of ventilator-associated events, including ICU-AW and VAP, and mortality rates.
Interventions for shortening the duration of MV therapy could lead to a reduction in total inpatient costs because MV has been associated with significantly higher daily costs for patients receiving ICU treatment. 2 Accordingly, acupuncture treatment for weaning from MV might be beneficial for cost reduction among inpatients requiring MV in the ICU setting. In the present study, the authors did not perform cost calculation. Further study of cost calculation for ICU stay should be conducted.
This observational study performed based on a retrospective chart review has several limitations in interpreting the results because of the small sample size and varied characteristics of the participants, including reasons for admission to the ICU and initiation of MV therapy. However, the findings of the present study suggest the beneficial effects of acupuncture treatment on the respiratory parameters of patients receiving MV in the ICU. Further prospective cohort studies with large sample sizes and homogeneous patient groups are required.
Conclusion
Adjunctive acupuncture therapy has beneficial effects on the respiratory status and may help in weaning patients from mechanical assistance in the critical care setting. Further prospective large cohort studies are warranted.
Footnotes
Acknowledgments
The authors thank all participants and staff in the Advanced Critical Care Center in Gifu University Hospital. They thank Dr. Shinsuke Ojio and Dr. Shusaku Miyata for the ideas and important advice for this study. A part of this report was supported by MEXT KAKENHI 25460894 (Grand-in-Aid for Scientific Research [C]).
Author Disclosure Statement
No competing financial interests exist.