
Abstract
Objective:
The term “Mauve factor” (pyrroluria) dates back to 1958 when Dr. Abram Hoffer defined the condition as elevated levels of pyrroles in the urine, currently called hydroxyhemepyrrolin-2-one (HPL). It was suggested that the raised pyrrole levels lead to depletions in zinc and vitamin B6, which, in turn, were hypothesized to result in a range of psychiatric disorders, such as schizophrenia, anxiety, and depression. Treatment implications are supplementation with zinc and B6. This article aimed to review the scientific literature associating pyrroluria with psychiatric symptoms, explore the validity of HPL testing, explore the role of nutrients as treatment options for pyrroluria, and discuss future research directions.
Methods:
A PRISMA review was conducted using search results from electronic databases PubMed, MEDLINE, PsycINFO, EMBASE from inception to February 2020 using the following keywords: hydroxyhemepyryrrolin (HPL), kryptopyrrole (KP), mauve factor, pyroluria, pyrroluria, monopyrroles. Article reference lists were also scanned and included where relevant.
Results:
Seventy-three articles were identified of which only three studies identified significantly higher HPL levels in a psychiatric population compared with controls, and there were no placebo-controlled treatment trials directed at pyrroluria. The other 13 clinical studies either showed no association or did not provide adequate data to show group differences in HPL levels. Despite an extensive history of practitioners diagnosing and treating a wide variety of mental health conditions associated with pyrroluria as well as clinical observations of elevated HPL being associated with psychiatric disorders, there was no clear research that showed the following: (1) elevated HPL is robustly associated with increased mental health symptoms, (2) elevated HPL in urine is associated with increased urine excretion of zinc and B6, and (3) high-dose zinc and B6 are an efficacious treatment for mental health problems associated with elevated HPL.
Conclusions:
Elevated HPL is a clinically observed, but poorly researched biomarker with unclear associations with mental disorders. Based on current evidence, HPL testing is not recommended as a screening or treatment tool. Further research is required in the following areas: establishment of which specific clinical populations exhibit elevated HPL, validation of the chemistry and validity of testing, and controlled trials to establish efficacy of high-dose zinc and B6 as treatment of elevated pyrroles.
Introduction
Pyrroluria (also known as kryptopyrrole [KP], pyrrole, or mauve factor-disorder) is a controversial condition defined by the presence of elevated levels of pyrroles in the urine believed to increase urine losses of zinc and B6, through binding with the pyrrole.
Currently, clinicians and laboratories worldwide are testing and “treating” tens of thousands of psychiatric patients with high-dose nutrient therapy, often utilizing zinc and B6, based on urine metabolite results identifying elevated “pyrroles.” Indeed, as of 2016, one laboratory in Australia had tested over 20,000 patients for pyrroluria, typically using 20 mcg/dL as the arbitrary cutoff point for determining elevated pyrroles (V. Dahlia, Personal Communication, 2016). Many hundreds of psychiatrists and other medical professionals in Australia have been trained to diagnose and treat this condition via a training course run by Bio-balance Health Australia and the Walsh Research Institute (A. Harrington, Personal Communication, 2017).
References to “pyroluria” are ubiquitous on the internet, with various subjective questionnaires developed to assist a person to “diagnose” or provide “treatment” for the condition. For example, in early 2020, a Google search for pyroluria/pyrroluria produced over 64,000 results. One Facebook support group named “pyroluria” has over 9300 followers. 1 In contrast, a PubMed search of pyrroluria produced only two hits, and its alternative spelling, pyroluria, produced just a single hit. Considering that thousands of people are being identified with this condition and treated with high doses of nutrients, it is essential that the scientific merit of this condition is investigated.
Pyrroluria was historically named by the Hoffer Group in 1958 after the discovery of a “lavender” (mauve) color appearing on the chromatographic paper containing the urine of psychiatric patients, specifically people identified with schizophrenia, a color not observed in controls. 2 –4 They were searching for a biochemical origin for schizophrenia and wondered whether the cause of the “lavender” color was associated with the psychiatric symptoms in some way. The mauve color was later discovered to be caused by the presence of elevated levels of a pyrrole, hydroxyhemepyrrolin-2-one (HPL), leading to the naming of the presence of these pyrroles in the urine as “pyrroluria.” 5 This biomarker discovery then led to 60 years of documentations in the scientific and popular literature of how this biomarker might be associated with psychiatric disorders.
Aims and Methods
This review aimed to systematically document the research behind the clinical observations between HPL and psychiatric diagnoses, the validity of HPL testing, and treatment of pyrroluria. Utilizing PRISMA guidelines (Fig. 1), electronic databases PubMed, MEDLINE, PsycINFO, and EMBASE were searched from inception to February 2020 using the following keywords: “hydroxyhemepyryrrolin” or “kryptopyrrole” or “mauve factor” or “pyrroluria” or “pyroluria,” or “pyrolluria” or “monopyrroles.” 6 Article reference lists were also scanned and included where relevant. After eliminating unrelated results (n = 3), protocols (n = 2), and duplicates (n = 99), 73 journal articles were identified covering clinical observations between HPL and mental health disorders (n = 16), biochemistry and toxicology (n = 30), validity of HPL and HPL testing (n = 16), and treatment (n = 11).
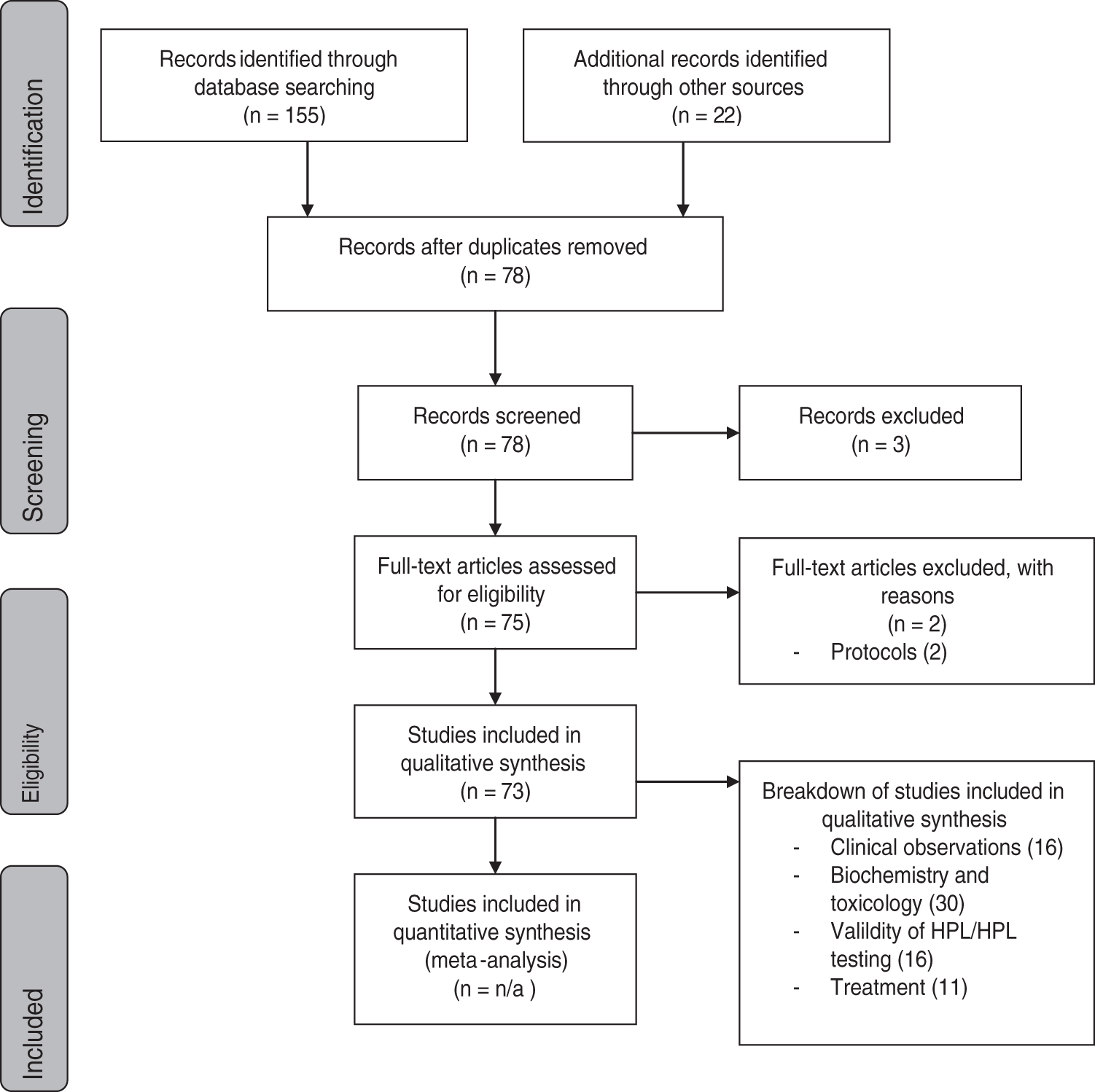
PRISMA flowchart indicating identification, screening, eligibility and inclusion articles.
Results
Clinical observations
Given the long history of identifying HPL and clinical use, below the authors systematically and chronologically describe the empirical research supporting the association between psychiatric disorders and elevated HPL.
As mentioned, pyrroluria was first associated with schizophrenia by Hoffer's Group, with estimates of pyrroluria ranging from 36% in one sample of 222 individuals with schizophrenia to 69% of 39 individuals with schizophrenia, 7,8 while Hoffer reported in a review that 75% of persons diagnosed with schizophrenia showed elevated HPL. 3
In 1965, O'Reilly, Ernest and Hughes published results from HPL testing done within a hospital setting. 9 They tested 850 children and adults with a range of mental and physical health disorders. Twelve percent of 411 individuals with physical disorders returned an elevated HPL test and 52.3% of 86 individuals diagnosed with schizophrenia had a positive HPL test; however, no statistical comparisons of the groups were performed. 9
In 1967, Sohler et al. showed significantly higher HPL excretion in individuals with schizophrenia (n = 20) compared with laboratory staff (n = 20) from the New Jersey Neuro-psychiatric Institute. 10 In 1973 and 1974, Carl Pfeiffer primarily studied people with schizophrenia in sanatoriums. 11,12 Pfeiffer observed that pyrroluria was present in 30%–40% of those with schizophrenia compared with 5%–10% of people without schizophrenia, using a urine cutoff of 20 nmol/L. 12 Pfeiffer also observed a nonsignificant decrease in zinc excretion in individuals with schizophrenia compared with controls when given high-dose B6. 12 While increased excretion of zinc and B6 was cited by Pfeiffer, no other studies replicated this claim. 5
Other studies have not documented this association between high HPL and psychiatric illness. 13 –16 For example, Gorchein found no significant differences in the concentration of HPL in people with schizophrenia (n = 146) compared with general medical patients (n = 42). 17 Cruz and Vogel compared HPL levels in urine samples of healthy individuals (n = 10) versus individuals diagnosed with schizophrenia (n = 9) and found no significant differences between groups, but with a very small sample size, this is not unexpected. 18
Through the mid-1980s to 2008, very little research and clinical observations were published on pyrroluria. The Hoffer group published an editorial, but no further evidence could be drawn from it. 3 Walsh at al. studied data from 8000 patients treated at the Pfeiffer Treatment Center over a 10-year period for a variety of psychological disorders (including attention-deficit/hyperactivity disorder, conduct disorder, oppositional-defiant disorder, and other behavioral disorders). Elevated HPL was observed in 32.9% of the study population. 19 Issacson et al. performed a retrospective study of 41 autistic children treated through the Pfeiffer Treatment Center, finding nearly 50% to have elevated pyrroles; however, due to multiple treatment options exercised, no significant treatment results can be determined for pyrroluria. 20
In 2010, Stuckey et al. published their pilot clinical findings on HPL testing. Their study investigated targeted nutritional therapy in 567 patients with a range of mental illnesses receiving medical treatment, interviewed them, and followed them for 12 months, of which 382 complied for 1 year. HPL was measured at baseline and used to direct treatment to increase zinc and B6; however, treatment involved a range of targeted and personalized nutritional programs depending on the results from a number of biomarkers measured. The article indicated associations between high HPL (>20 mcg/dL) and psychiatric symptoms, including nervousness, moodiness, worries, hallucinations, and aggression; however, how these associations were determined was not described. Forty-five percent of the sample noted major improvement, via a verbal consultation, after 12 months. The team did not look to see whether HPL predicted treatment response. 21
In 2015, Mikirova published data mined from the Riordan clinic and found that 65% of 119 ADHD patients had pyrrole levels higher than 20 mcg/dL. 22 Again in 2015, Mikirova published data based on 148 patients with schizophrenia, 135 with bipolar disorder, 97 with depression, and 119 with ADHD. 23 Their HPL levels were evaluated relative to individuals with nonmental health conditions and healthy volunteers (unknown number), but not statistically compared. Forty-eight percent of those with ADHD, 22% of those with schizophrenia, 30% of those with mood disorders, and 26% of those without a specific diagnosis were identified as having elevated pyrroles (>20 mcg/dL).
Fryer-Williams and Strobel, in a search for a biomarker for schizophrenia, conducted a retrospective case/control study comparing 67 Diagnostic and Statistical Manual (DSM) IV-R diagnosed patients with schizophrenia and schizoaffective psychosis with 67 control participants who were volunteers recruited from the same hospital catchment and subject to the same inclusion criteria except that they did not meet the criteria for a DSM diagnosis. 24 This study represents the most robustly conducted assessment, and unlike many of the other studies provided explicit details of the testing methodology. Fifteen biomarkers emerged as predictors for schizophrenia and schizoaffective disorder on a receiver operating curve analysis, of which high HPL/creatinine was one. HPL levels were also significantly correlated with low serum zinc. Elevated HPL was also significantly correlated with symptoms of anxiety. 24 Like the clinical observations, the study indicates a possible relationship among HPL, nutrient levels, and psychiatric symptoms, but requires further exploration and replication.
Two years later, Heitzman et al. investigated HPL in 36 extremely aggressive males diagnosed with a serious mental illness (schizophrenia, psychosis), using a matched subject design, with 22 controls matched for age without a mental disorder or history of aggression. 25 Like Fryer-Williams and Strobel, the methodology of measuring HPL was described. No significant difference was found between groups for HPL levels; however, when the results were adjusted for creatinine, a significant group difference was found, identifying that the participants with aggression showed higher HPL/creatinine levels compared with the controls. As the concentration of the urine can have a significant effect on the sample concentration, using creatinine as a marker of concentration and adjusting accordingly is now a common analytical technique for correcting the sample concentration levels. While Heitzman et al. developed a proprietary method for the synthesis of HPL for the purpose of this study, the methodology is yet to be published.
Overall, despite the fact that pyrroluria has been described since 1958, the authors found only 16 publications that reported on the association between HPL levels and a psychiatric disorder, the majority of the observations being made within psychiatric inpatient wards and only five statistically comparing people with and without a psychiatric condition. Three of these five studies showed higher HPL levels in the psychiatric sample compared with controls. Inconsistencies across the publications in data reporting made comparison of the studies challenging and highlight the need for structured and systematic reporting in this field.
Biochemistry and toxicology of HPL
There were many articles exploring the origins of the “mauve” color and the articles revealed an interesting evolution in the understanding of what might be causing the color. The earliest articles from 1969 to 1970 misidentified mauve factor as a KP.
26,27
In the 1970s, the research isolated mauve factor as HPL, an oxidized form of KP.
16,28
–39
Despite most of the studies agreeing on HPL as the cause of the “mauve” color, other researchers such as Gendler et al. suggested that it was neither KP
The structural similarity of the two compounds (KP and HPL) resulted in confusion, and interchangeability of the terms remains common today. HPL is currently the standard in the colorimetric assay; but the term KP is still used in some testing suites. 41 Testing for these pyrroles evolved over the years from using a chromatography paper to using a colorimetric assay to measure HPL levels. 5 Around the same time, a number of hypotheses developed about various pink spots appearing on chromatographic paper. As an aside, it is important to note that both KP and HPL should not be confused with other chromatogram results where “pink spots” may appear. 42,43 These spots had not been precisely differentiated and are thought to represent a different set of molecules than those associated with pyrroluria and HPL. 4,15,35,44
A number of studies were also identified that investigated whether injecting animals with HPL or KP had any effect on their behavior. For example, Walker 36 injected 10 rats with 2,4-dimethly-3-ethypyrrole, a molecule with similar structure to HPL, and observed marked behavioral changes in the animals, including ataxia, hyperventilation, locomotor depression, and catalepsy together with major central nervous system dysfunction. 36 Behavioral changes were also observed by Wetterburg. 38 Somogyi et al. observed increased brain activity in cats injected with KP. 45 In contrast, Cutler et al. found minimal behavioral changes. 46 Graham et al. showed increased heme metabolism in rats injected with HPL (KP). 47 Gorchein et al. found that injected KP inhibited rat and guinea pig digestive function. 48,49 Brodie et al. showed increased pyrrole production when rats were injected with KP. 37 Other animal studies have looked at the association of elevated HPL with the human hereditary hepatic porphyria, where increased pyrroles of a different nature are produced. 37,38,50,51 Findings indicate a complex and unknown relationship between the two types of pyrroles. 37,38,52 To the best of knowledge, no other animal studies have been conducted. Animal studies indicate that high levels of HPL appear to have mixed effects, symptoms appearing to be nonspecific and unrelated to symptoms described in humans, but biochemically similar to the hepatic porphyria.
Validity of HPL and HPL testing
Irvine, a renowned chemist, published in 1961 the “apparent” relationship between the mauve positive test relating to mental illness. 2 Despite all the clinical observations between HPL and psychiatric symptoms, the origin of HPL is still unknown. Pfeiffer suggested that HPL originates from the breakdown of heme. 42,53 Others have pointed to dietary sources such as porphobilinogen, porphyrins, and bile pigment. 5,42,52,54 –57 The relationship with porphyrins remains close, with porphyria being a genetic disease, suggesting there may be a genetic component to increased HPL excretion. 57,58
Not only is the biochemical source of HPL unknown, the mechanism for increased excretion remains unknown. The most often proposed mechanism of action is that the pyrrole binds to vitamin B6 and zinc and thereby depletes the body of these essential nutrients. However, although the binding of B6 and zinc to the HPL is plausible, Sohler et al. suggested that similar molecules have also been shown to complex (bind) with zinc. 42
Others suggested that increased HPL is a marker for increased oxidative stress. 5,42,58,59 Indeed, Pfeiffer referred to pyrroluria as a stress-induced disorder, the symptoms of which he believed diminished when the degree of stress lessened, raising the possibility that high pyrroles in the urine may not be static. 60 More recently, HPL has been associated with gut dysfunction with elevated urinary HPL being associated with increased levels of indicans (a marker of intestinal bacterial overgrowth). 23 Antibiotic use has also been associated with higher levels of HPL. 5 Interestingly, Durko et al. showed that hemodialysis decreased the excretion of mauve factor in schizophrenia. 61
It is also important to emphasize that despite all the clinical observations of elevated HPL being associated with psychiatric symptoms, a number of the studies reviewed identified significant challenges in the measurement and HPL thresholds, problems that tend to be overlooked in the clinical observations. One issue identified was a lack of specificity of the chemical assay used to measure HPL, with the assay being extremely sensitive to a number of other substances, possibly including a common metabolite in urine, urobilinogen. 42 The different levels of HPL may be due to variances in the chemical assay methodology and interference from other metabolites. For example, Pfeiffer stated above 16 mcg/dL, whereas Mikirova identified above 20 mcg/dL, as a cutoff for a clinical problem in need of treatment. 23,62 As an aside, clinically, while it is generally accepted that normal levels of pyrroles range from low levels: 4–10 mcg/dL, mild: 10–20 mcg/dL, moderate: 20–50 mcg/dL, and severe: above 50 mcg/dL, 5,63 –65 it is important to note that validation of these levels is yet to be published.
The review identified specific challenges associated with the standardization of the HPL testing, including sample collection and transport to the laboratory. The half-life of the HPL molecule is reported to be ∼10–12 h, and once excreted, 66 the HPL molecule readily interacts with light, 67 oxygen, and Ehrlich-reactive compounds, 42,58,66 quickly becoming unstable. Recommendations for overcoming these problems included treating the sample carefully to ensure that the molecule is collected correctly, and transporting the sample to the laboratory in tightly controlled conditions (frozen and protected from light). It is likely for these reasons that clinicians who regularly test for HPL in their patients often report high levels of false negatives. 68 Initial work with a high-pressure liquid chromatography/mass spectrometry (LC/MS) assay shows promising sensitivity and specificity. 5 Heitzman et al., using synthesized HPL, developed an LC/MS assay, but as there is no scientific documentation of the chemical method, the methodology cannot be validated. 25 Overall, the literature highlighted that the measurement techniques used for pyrroluria are highly problematic and likely contribute to the confusion and controversy.
Treatment for pyrroluria
Despite all these problems with measurement of HPL as well as mostly poorly controlled studies investigating the association between HPL and psychiatric symptoms, there is a body of clinical observations detailing the treatment of pyrroluria. The early Hoffer observations showed an association with elevated pyrrole and mental disorders. Both medications and vitamins were used as treatment, and a decrease in pyrroles was observed as individuals improved, with various explanations given. 8,69 –73 Pfeiffer documented that zinc and B6 would “rid the mind of schizophrenic symptoms within one to 7 days in the 30% of patients with schizophrenia that are pyrroluric” (p. 107). 74
Pfeiffer and Bacchi suggested that the dose of B6 needed by a patient with high HPL levels may be as high as 3000 mg per day to prevent psychopathy and keep the urine free from HPL although the authors found no controlled research to support this recommendation. 53 Other clinicians claim a quick response reporting that many of their patients completely recover with an amelioration of mood or anxiety symptoms, often within a number of months, although no information on overall effectiveness, how it was measured, and on who was provided. 75
Indeed, based on the known effects that these two nutrients, zinc and B6, can have on the brain, it makes some physiological sense to supplement with these nutrients. As background, pyridoxine (B6) plays a key role in the metabolism of sulfur-containing amino acids such as homocysteine as well as the formation of neurotransmitters such as epinephrine, norepinephrine, serotonin, and γ-amino butyric acid. 76 B6 deficiency has been implicated in multiple mechanisms in association with mental health disorders. 77 In turn, zinc plays a role in many diverse biochemical roles, including nucleic acid metabolism, neurotransmitter production, antioxidant activity, cell signaling, brain and immune function. 78 Plasma zinc is only a good marker of zinc status at the extremes of deficiency and excess, and for tracking supplementation. It is a poor marker for overall status due to blood levels of zinc being tightly maintained by homeostasis. 79 –81
However, despite 60 years of documented associations between elevated pyrroles and psychiatric disorders and the hypothesized mechanism of the pyrroles increasing urine losses of B6 and zinc, 11,12,82 as well as observations showing that high HPL levels may be associated with lower B6 and zinc levels, 5,22,83 the authors found no placebo-controlled studies using B6 and zinc in combination as a specific treatment for people presenting with elevated pyrroles.
Two research trials were found that directly investigated whether nutrients given to individuals with psychiatric symptoms resulted in changes in HPL levels, but the samples were not selected for high HPL. The first one studied 32 aggressive juvenile male participants in an open-label, 16-week micronutrient treatment trial. 84 Participants received high-dose zinc and B6 together with other nutrients based on body weight. The micronutrient therapy significantly improved parent-reported aggressive and violent behaviors. This was measured using the Children's Aggression Scale, with a medium to large pre-to-post effect size (Cohen's d = 0.7). Plasma zinc significantly increased and plasma copper significantly decreased. HPL was measured at baseline and endpoint, with baseline measurements ranging from 19 to 204.4 mcg/dL. Nevertheless, no significant difference was found between pre- and postintervention urinary HPL, suggesting that supplementation of zinc and B6 did not change HPL production and excretion.
The second study is the only double-blind experiment published investigating whether additional nutrients can modify psychological symptoms and HPL; however, this study did not use zinc and the children were not chosen based on elevated pyrroles. 85 The study investigated the introduction of vitamin C, B3, B5, and B6 with a low-carbohydrate, high-protein diet in 20 children with learning disabilities over a 6-month period. All children received the low-carbohydrate, high-protein diet with the experimental group receiving extra nutrients. No significant differences were found between groups receiving the nutrients or placebo, with both groups showing significant improvement in auditory discrimination and some behavioral measures. Urinary excretion of HPL was unrelated to participants showing any pre/post test improvements and therefore was shown to be invalid as a screening test.
Despite there being no placebo-controlled studies looking specifically at the use of vitamin B6 and zinc as a treatment of pyrroles, a number of resources found within the context of this review cite the use of zinc and B6 for treatment for pyrroluria. 12,75,59,86,87 However, often the information on what was done, on who, how effective it was, and for how long was not detailed enough to be described further. Independent of this systematic search, the authors are aware of the large literature using these two nutrients alone as treatments for psychiatric disorders in general but not pyrroluria specifically.
The interested reader could explore these single nutrient treatments, appreciating that the research is mixed with some studies showing a positive effect 88 –90 and others showing no effect. 91 –93 They should also be aware of the safety of these nutrients. Amounts of B6 given by practitioners seem to vary from 100 mg 94 up to 1000 mg B6 twice a day. 60 The primary concern of supplementing with high-dose vitamin B6 is nerve damage and peripheral neuropathy (loss of feeling in extremities). 95 –97 The National Institutes of Health cautions that this can occur when supplementing with 200 mg or more daily; however, such symptoms are reported to resolve when supplementation is stopped. 98,99 Overall, studies indicate a good short-term safety profile with doses ranging from 300 to 900 mg. 84,100
Studies suggest that zinc given in short trials lasting 2–12 weeks in doses of 100–200 mg zinc is reported to be well-tolerated, has a low risk of side effects, and provides no evidence of zinc toxicity. The clinician needs to be mindful of the potential for zinc toxicity that can occur in both acute and chronic exposure. Acute exposure can result in nausea, vomiting, loss of appetite, abdominal cramps, diarrhea, and headaches. 101 High doses of zinc have been shown to adversely affect copper status, iron function, immune function, and cholesterol. 102,103 While the recommended daily UL of zinc for adults is 40 mg, the safety of long-term zinc supplementation with “at need” individuals requires further research.
Summary and Future Directions of Research
This review has revealed that while pyrroluria remains a popular diagnosis within a certain segment of practitioners, its popularity is currently not supported by a solid empirical and independent body of research. Key aspects of HPL remain unclear, including a specific validated chemical assay, the affinity of HPL to zinc and B6, the prevalence of elevated HPL within individuals with mental health disorders as well as healthy populations, accuracy of current practitioner screening scales, optimal treatment protocols, treatment effect on levels of HPL in urine, long-term effects of treatment, and exact biochemical metabolic pathways that generate HPL.
Overall, the human studies conducted over the past six decades identify that the psychiatric symptoms associated with elevated HPL primarily come from clinical observations, they are highly variable, and it is unclear how reliable these observations are, given that many of the details of how the patients were identified and diagnosed were simply not provided. Clinical symptoms studied are broad including anxiety, pronounced mood swings, nervousness, low stress tolerance, depression, panic attacks, motion sickness, general loss of appetite, social withdrawal, and memory loss. 64,104 However, these associations have led to many questionnaires being developed and circulated on the internet and in books, claiming to be highly correlated with HPL testing. 105 One prominent laboratory claims that 80% of their patients who score high on its pyrroluria screening questionnaire also had elevated HPL urine test results (J. McGill, Personal Communication, 2016). At present, these questionnaires have no validation data.
It was also often unclear whether the HPL levels were measured before or after treatment. Only five studies directly compared psychiatric with nonpsychiatric patients, with three of these five showing that HPL is significantly more elevated in those with a psychiatric diagnosis compared with those without a psychiatric diagnosis. There are also no longitudinal studies to determine if high HPL precedes the psychiatric diagnosis or is a consequence of the illness. Furthermore, high HPL is clearly not specific to any one disorder although may be a biomarker of an underlying pathophysiology that could be common across all disorders, such as oxidative stress, intestinal bacteria, or inflammation. 23
The research on using zinc and/or B6 suggests that those nutrients may well have a place in psychiatry; however, it is important to note that none of the controlled researches has been conducted in association with HPL levels. Whether the pharmacologic effect is due to replenishing wasted nutrients is yet to be established, as no controlled studies confirm increased zinc and B6 excretion in persons with high HPL.
Considering the high prevalence of mental health issues in the population and the fact that current treatments do not always effectively meet the clinical needs of many people suffering from these conditions, 106 novel treatments do need to be explored. The clinical observations indicate that HPL may be a possible biomarker; however, without properly controlled studies, confidence in it continues to be severely compromised.
There are numerous future directions for further research of HPL, symptoms, and treatment. First, the chemistry of the molecule needs to be established and validated via liquid chromatography mass spectrometry (LC/MS) utilizing synthetic HPL. LC/MS could then become the gold standard for laboratory testing of this molecule. Second, the biochemistry of the origin of the molecule also needs to be investigated to establish potential treatment pathways. In vitro binding of HPL to zinc and B6 needs to be examined to validate the potential of high HPL to increase wasting of zinc and B6 via the urine. Third, HPL levels need to be established for both the background population and specific populations with both mental and physical health diagnoses. Elevated HPL then can be associated with specific health conditions and screening questionnaires created and validated. Finally, double-blind, placebo- controlled trials are required to establish efficacy of nutrient treatment. There is simply no evidence to back the current testing and treatment practices.
Clearly, there is clinical evidence of replicated observations of elevated HPL being associated with more mental health problems; however, without research to verify whether these observations hold up with robust and validated assessment of mental health symptoms, it is impossible to determine if pyrroluria is fact or fiction.
Footnotes
Author Disclosure Statement
J.S. has received presentation honoraria, travel support, clinical trial grants, book royalties, or independent consultancy payments from the following: Integria Healthcare and MediHerb, Pfizer, Scius Health, Key Pharmaceuticals, Taki Mai, Fiji Kava, FIT-BioCeuticals, Blackmores, Soho-Flordis, Healthworld, HealthEd, HealthMasters, Kantar Consulting, Grunbiotics, Australian Natural Therapeutics Group, Research Reviews, Elsevier, Chaminade University, International Society for Affective Disorders, Complementary Medicines Australia, SPRIM, Terry White Chemists, ANS, Society for Medicinal Plant and Natural Product Research, Sanofi-Aventis, Omega-3 Centre, the National Health and Medical Research Council, CR Roper Fellowship. B.W. is a practicing clinical nutritionist, clinical director of a natural health clinic, director and shareholder of a natural health company (BePure Health Group) that manufactures nutritional supplements for the public. No financial affiliation exists between the University of Canterbury and the BePure Health Group.
Funding Information
J.S. is supported by an NHMRC Clinical Research Fellowship APP1125000.