
Abstract
Eosinophilic conditions are reviewed briefly, including the fact that early misunderstanding likely led to the now largely discredited idea that eosinophils are crucial to their the pathogenesis of these chronic allergic conditions. They can be relieved effectively by a range of herbal medicines—just a small selection of the large number of such medicines that have been studied, which are reviewed here.
Ephedra sinica
(ma huang) is discussed in some detail as one of the strongest traditional antiallergic agents in Chinese medicine. Many studies—including those involving ma huang-dominated formulas such as Dìng Chuăn Tāng (Arrest Wheezing Decoction) and Má Huáng Fù Ziõ Xì Xīn Tāng (Ephedra Aconite Asiasarum formula)—have shown ma huang to be effective for people with eosinophilic conditions.
Ammi visnaga
(khella) and a semisynthetic medication made from its compound khellin, cromolyn, are reviewed in depth. Yù Píng Fēng Săn (Jade Windscreen Powder) has been shown to be synergistic with cromolyn.
Quercetin, a flavonoid in wide clinical use by natural practitioners for patients with allergies, and a related flavonoid, luteolin, are discussed as potentially effective antieosinophilic compounds.
Finally, the immunomodulating herb Astragalus membranaceus (astragalus; huáng qí) is reviewed as a very different and effective agent directed toward T-cell problems underlying eosinophilic diseases.
Introduction
A number of diseases share in common excessive eosinophilia and other features of type I hypersensitivity reactions without anaphylaxis (see sidebar, Eosinophilic/Chronic Allergic Conditions). Some of these conditions (such as hayfever and atopic dermatitis) are well-established; others are just starting to be recognized. For example, eosinophilic esophagitis was formerly regarded as a rare condition but, once gastroenterologists started biopsying macroscopically normal-appearing esophageal tissue in more patients with apparent noninflammatory gastroesophageal reflux symptoms, these researchers found that the condition is actually quite common. 1 Reports of the rarity of other eosinophilic diseases should also be treated cautiously until researchers actually start looking for these conditions specifically to determine their true incidence and prevalence. Some patients have multiple symptomatic eosinophilic diseases at one time, although, again, most patients with symptoms in one area are not routinely assessed for other conditions, but it may be that systemic eosinophilia/type 1 hypersensitivity problems are systemic in many of these patients. 2
Although eosinophils are important in the pathophysiology of many of these diseases, it is likely that eosinophils are not the only—or even the most important—cells involved in these diseases. 3 The association and naming of some eosinophilic diseases appears to have resulted from early identification of eosinophils of tissues of experimental animals with features of these conditions but, now, it is understood that other immune cells play even more important roles. These immune cells include Th2 lymphocytes, mast cells, basophils, and B-lymphocytes. Note that nonallergen factors can stimulate mast-cell and basophil degranulation, including physical injury (mediated by damage-associated molecular pattern molecules or DAMPs), infection (mediated by pathogen-associated molecular pattern molecules or PAMPs), complement proteins, stress-related compounds including corticotropin-releasing factor and substance P, and activation of a range of G protein–coupled receptors including μ-opioid receptors (which results in itching as a common adverse effect of opioid drugs).
A growing awareness of the multiple chronic inflammatory processes behind the conditions listed in the box entitled Eosinophilic/Chronic Allergic Conditions has led to a change in understanding of what can cause at least some subsets of these conditions, and also led to a change in their nomenclature. This change, however, is still inaccurate; for naming the conditions, for example, the term eosinophilic does not capture the clearest and most complete picture of these conditions, but the terms used are the common ones currently in use. These conditions should perhaps be called, for instance, chronic allergic cystitis or chronic allergic esophagitis, and not eosinophilic cystitis or eosinophilic esophagitis.
Allergic asthma
Allergic rhinitis/conjunctivitis, hayfever
Atopic dermatitis
Eosinophilic esophagitis
Eosinophilic gastritis (Russell body gastritis)
Eosinophilic duodenitis (Russell body enteritis) a
Eosinophilic colitis
Eosinophilic cholecystitis b
Eosinophilic cystitis c
Eosinophilic prostatitis d
Nwokediuko SC, Ijoma UN, Obienu O, et al. High degree of duodenal inflammation in Nigerians with functional dyspepsia. Clin Exp Gastroenterol 2013;7:7–12; bMuta Y, Odaka A, Inoue S, et al. Acute acalculous cholecystitis with eosinophilic infiltration. Pediatr Int 2015;57:788–791; cLi G, Cai B, Song H, Yang Z. Clinical and radiological character of eosinophilic cystitis. Int J Clin Exp Med 2015;8:533–539; dLiu S, Miller PD, Holmes SA, et al. Eosinophilic prostatitis and prostatic specific antigen. Br J Urol 1992;69:61–63.
Figure 1 presents an overview of the pathophysiology of type 1 hypersensitivity including late/chronic effects that are common to these conditions. In some cases, eosinophils develop large globules of immunoglobulins (Igs) that can actually displace their nuclei, which are known as Russell bodies. 4 Some conditions not classically thought of as eosinophilic are now known to involve eosinophils, mast cells, and basophils at least somewhat, including inflammatory bowel diseases, interstitial cystitis, and celiac disease. 5 Thus, the herbal treatments for these problems may have even wider applicability.
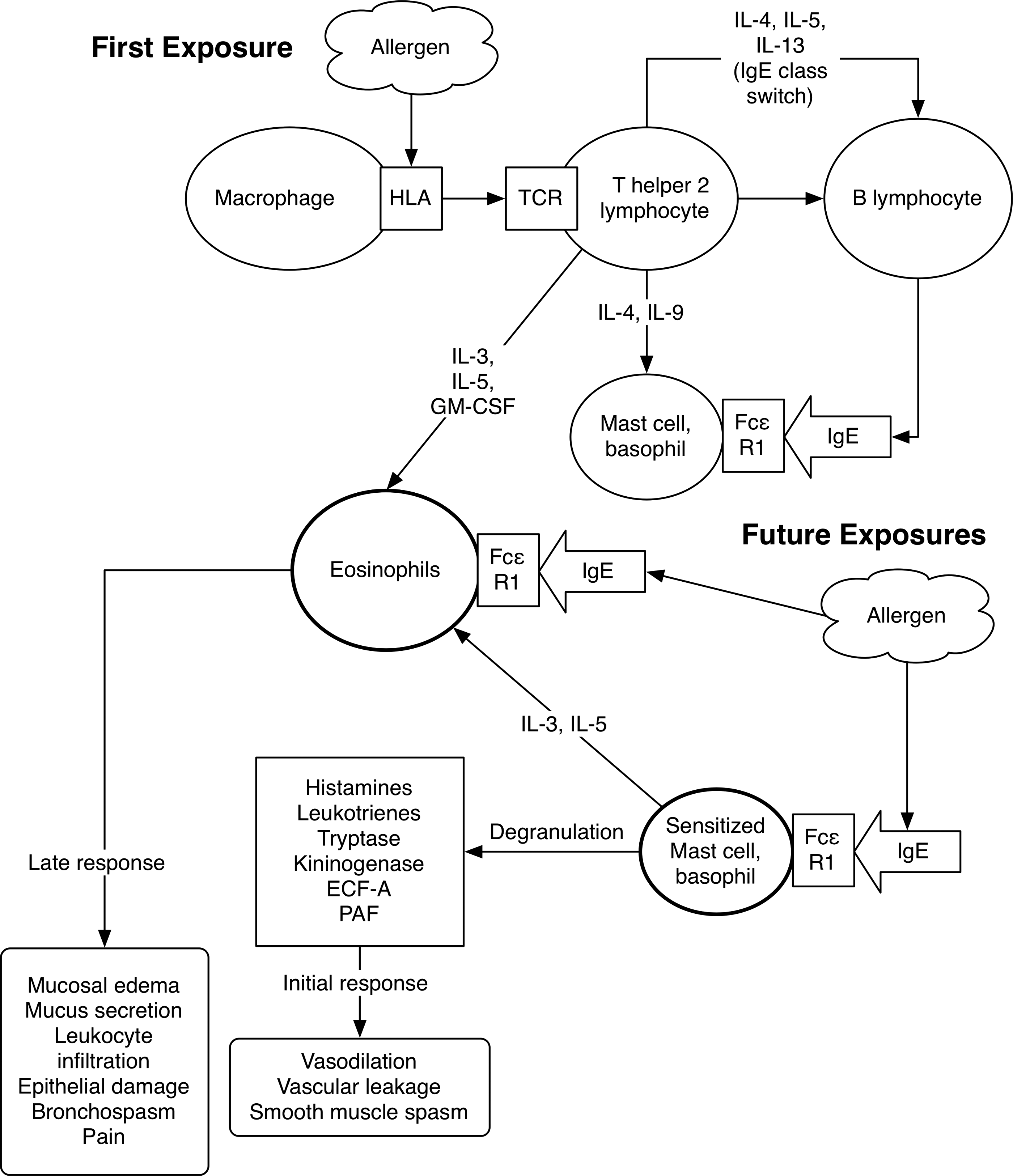
Pathophysiology of eosinophilic/mast-cell/basophilic/type I hypersensitivity conditions. IL, interleukin; Ig, immunoglobulin; HLA, human leukocyte antigen; TCR, T-cell receptor; GM-CSF, granulocyte-macrophage colony-stimulating factor; FcɛR1, high affinity IgE receptor; ECF-A, eosinophil chemoctactic factor A; PAF, platelet-activating factor.
Herbs can act against the eosinophilic/mast cell/basophilic chronic type 1 hypersensitivity process in many ways, as is shown with multiple examples in this article. Herbs can do the following: • Inhibit migration of the inflammatory cells to the site of a problem • Block degranulation of mast cells and basophils • Block activation of immune cells, including by shifting the Th1/Th2 lymphocyte balance toward greater Th1 predominance • Block various inflammatory pathways and receptors, including blocking histamine, leukotrienes, platelet-activating factor, and many others.
Most herbs studied to date have multiple actions and thus work on multiple fronts to help mitigate the pathophysiology and symptoms of eosinophilic/mast-cell/basophilic diseases. The amount of research on herbs and relevant pathways is so large that there is no way to review it all in this article; only some illustrative examples are discussed. However, most patients have underlying food or aeroallergen sensitivities, and identification and removal of these triggers is a high priority for achieving cures. 6,7
Ma Huang
Ephedra sinica (ma huang) stem is a useful antihistamine and antiallergy agent. It has a strong historical use for helping people with allergic diseases, including asthma and hayfever. 8 While clinical trials on the herb in isolation are lacking, some studies on herbal formulas featuring ma huang support its efficacy. In clinical practice, this herb is one of the most effective short-term symptom relievers in patients with eosinophilic/mast-cell/basophilic conditions and this effect is not limited to problems in the respiratory tract. 9
Ma huang is rich in pseudoalkaloids (also known as methylxanthines), notably theophylline, ephedrine, and pseudoephedrine isomers. They are pseudoalkaloids because the nitrogen occurs outside of a ring structure, unlike true alkaloids. These pseudoalkaloids are nonspecific α- and β-adrenergic agonists. Clinically, this makes ma huang helpful as a bronchodilator because of its β2 agonist effects to relieve acute attacks of the chronic allergic disease asthma, although the herb can cause hypertension and tachycardia because of β1 agonist effects. 10 Clinical trials have shown isolated ephedra pseudoalkaloids effective for relieving exercise-induced asthma and for chronic treatment of asthma in children who are already taking theophylline. 11,12 Unfortunately, research on the mechanisms of action of ma huang on mast cells, basophils, and eosinophils is limited but, nonetheless, is clinically useful.
An analysis of 1,000,000 randomly chosen Taiwanese people who used the national health care system of Taiwan showed that 85.7% of people with asthma (20,627 of this group) used Chinese herbal medicine for the condition.
13
Dìng Chuăn Tāng (Arrest Wheezing Decoction) was the most prescribed Chinese herbal formula in Taiwan for asthma. This formula originated in the Tài píng huì mín hé jì jú fāng (Formulary of the Pharmacy Service for Benefiting the People in the Taiping Era), compiled by the Imperial Medical Bureau ∼1100
A similar analysis of children (ages≤18) in Taiwan identified 45,833 with asthma, of whom 58% were using Chinese herbal medicine. Arrest Wheezing Decoction was once again the most prescribed formula in this population. 14 In a randomized, double-blinded trial, researchers compared 6 g of Arrest Wheezing Decoction to placebo in 52 children, ages 8–15, with mild-to-moderate persistent asthma. 15 The formula was decocted then dried to a powder and encapsulated. After 12 weeks, medication use, symptom severity, and airway hyperresponsiveness were all significantly reduced in the Arrest Wheezing Decoction group, compared to the placebo group.
The Má Huáng Fù Ziõ Xì Xīn Tāng (maō bushi saishin tō in Japanese; Ephedra Aconite Asiasarum formula in English) formula contains ma huang, Asiasarum sieboldii (Chinese wild ginger; xì xīn) root, and Aconitum carmichaelii (Sichuan aconite; fù ziõ) heat-processed lateral root. The formula originated in the Shāng hán lùn (Treatise on Cold Damage Disorders), written by Zhāng Zhòng-Jiõng in 220
Sensitized rats given Ephedra Aconite Asiasarum formula had a significant reduction in IgE-mediated anaphylactic reactions. 17 This was shown to result almost entirely because of the ma huang component of the formula, and it was, in part because of the inhibition of histamine release from IgE-stimulated cells by increasing cyclic adenosine monophosphate (cAMP) levels in the cells. Ephedrine pseudoalkaloids were not responsible for these effects.
However, ephedrine itself is an important part of ma huang's rapid actions against provoked type I hypersensitivity reactions. 9 The formula also reduces inflammation by blocking histamine and bradykinin release from mast cells and macrophages. 18 The formula has been shown to decrease eosinophilic infiltration, decrease plasma IgE levels, and block IL-4 and IFNγ production. 19 IL-4 produced by Th2 lymphocytes is critical in mast-cell and in IgE-secreting B-lymphocyte cell recruitment. One rat study found that administering the formula 1 hour before allergen exposure was significantly more effective than giving the formula after allergen exposure for preventing anaphylactoid reactions. 20 The formula, primarily because of its ma huang content, but also, in part, because of Chinese wild ginger, inhibits prostaglandin formation and thus inflammation. 21
A combination of ma huang and gypsum (calcium sulfate dihydrate; shí gāo) reduced eosinophilia in ovalbumin-sensitized rats and reduced asthma in them. 22 There is some evidence that gypsum may offset unwanted effects of ma huang. 23 Similar results were seen in ovalbumin-sensitized rats with a formula known as má huáng tāng (maō-tō in Japanese), which combines ma huang, Cinnamomum cassia (cassia cinnamon; guì zhī) bark, apricot pit seed, and Chinese licorice prepared root. 24 This formula originated in the Treatise on Cold Damage Disorders. The formula also clearly inhibited proinflammatory Th17 lymphocytes. 25
A typical dose of ma huang tincture (1:3 w:v) is 0.5–1 mL t.i.d. or as needed. A typical dose of the crude herb, powder, or granulation is 1–3 g t.i.d. At these doses, ma huang is generally completely safe. It is contraindicated in people with hypertension, coronary thrombosis, glaucoma, active hyperthyroidism, and benign prostatic hyperplasia (the herb worsens urethra blockage), and might cause or aggravate insomnia or anxiety in some people.
Ma huang was banned by the U.S. Food and Drug Administration (FDA) for weight loss and some American states (such as Illinois) banned the herb altogether or limited its used to adults only. Note that the FDA did not ban the use of the herb as a Traditional Chinese Medicine for treating allergies, though this agency has increasingly restricted supplies, making ma huang almost impossible to obtain. This is an unfortunate case of abuse of a legitimate herb in the marketplace leading to overregulation. It is particularly notable because the doses of ephedrine (60–90 mg) associated with hypertension, tachycardia, and various serious illnesses, including myocardial infarction and death, are at least three times higher than the doses necessary to address allergic disorders (10–15 mg, the amount available from the doses of whole herb recommended here). 25 Use of even purified ephedrine (including when combined with caffeine) under a practitioner's care, as opposed to people purchasing and using products from health food stores or online without guidance, has also been shown to be associated with no increased risk of harmful cardiovascular events. 26
Of 140 reports to the FDA of ma huang–associated problems, only 31% were found to be “definitely or probably” related to the herb. 27 A review of American poison control center data from 1996 to 2002 showed that, of 21,925 calls involving ma huang in some way, only 1% involved major toxicity, or ∼219 cases over 7 years (31 cases per year on average). 28 There were only 2 reported deaths, and none of the total reports assessed if ma huang was the definitive cause of the problem. Thus, while any severe outcome is terrible, the magnitude of ma huang toxicity has been vastly overstated. The level of harm from acetaminophen (with hundreds of deaths, at least 30 cases of acute liver failure requiring transplantation, thousands of hospital admissions, and hundreds of cases requiring mechanical ventilation every year in the United States), is significantly higher than that of ma huang; yet, acetaminophen remains available as one of the most commonly used and available over-the-counter medications in the world. 29,30
Ma huang had no interaction with the CYP1A2, CYP2D6, CYP3A, xanthine oxidase, or N-acetyltransferase 2 pathways of drug detoxification in one trial in healthy adults. 31 For greatest safety, this herb should not be combined with monoamine oxidase inhibitors or sympathetic stimulants.
Khella, Cromolyn, and Yu Ping Feng San
Ammi visnaga (khella) is an Apiaceae family plant native to the Mediterranean basin, North Africa, and the Middle East. The fruits are used as medicine, although they are often incorrectly called “seeds.” Khella has a history of use for treating asthma but has been used more as a bronchodilating agent. 32 This effect is attributed primarily to furanocoumarins in khella, notably khellin, visnadin, and visnagin, which act as smooth-muscle relaxers including via calcium-channel blockade. 33
In the 1950s, Roger E.C. Altounyan, MD (1922–1987
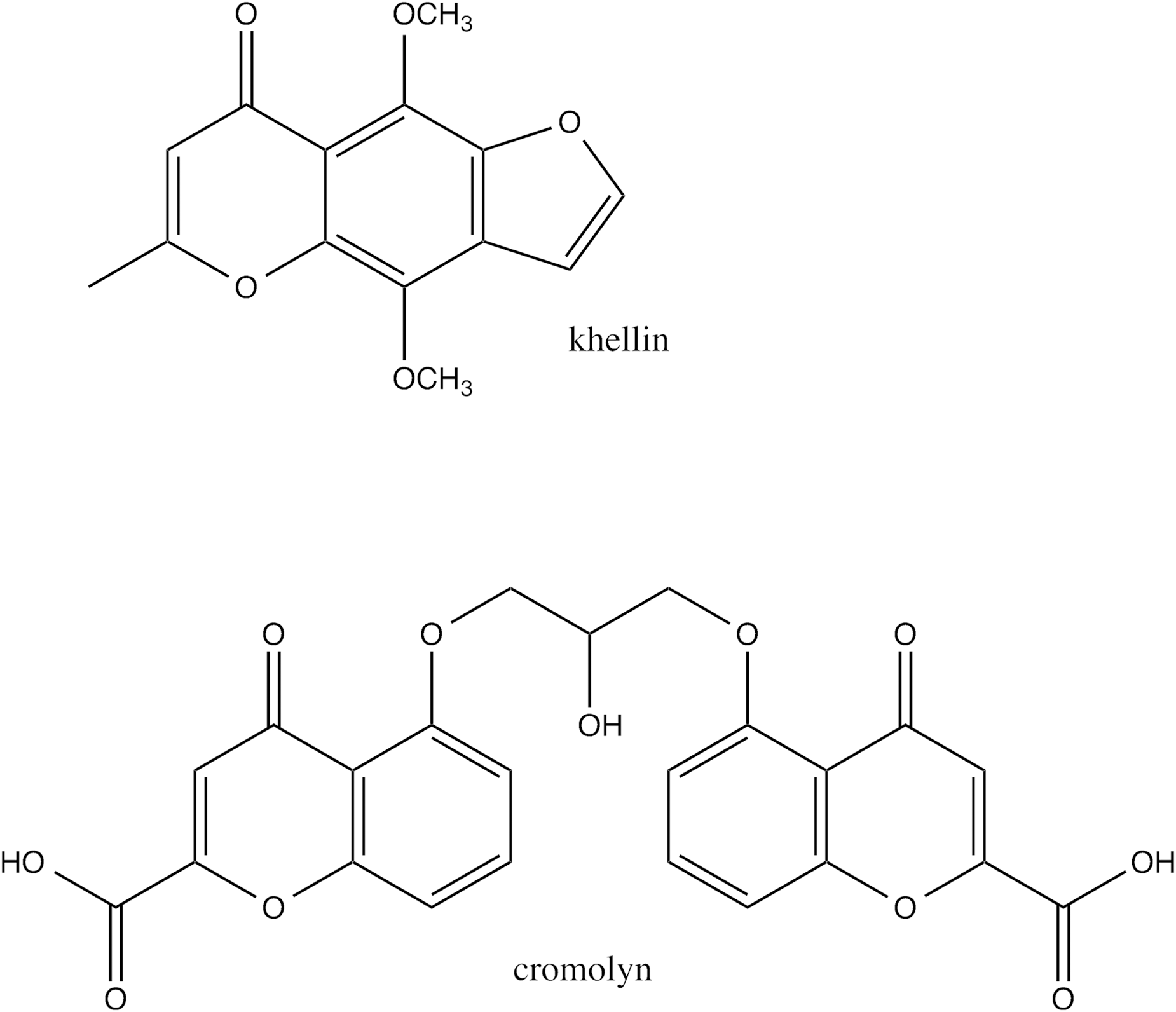
Cromolyn and khellin chemical structures.
Cromolyn can prevent symptoms caused by food allergy and so-called eosinophilic esophagitis (although this involves mast cells and basophils among other immune mechanisms). 41,42 The exact means by which mast cells are inhibited from degranulating despite incoming triggers that would normally cause degranulation is unknown, but may involve inhibition of tachykinins, inhibition of tumor necrosis factor–α (TNF-α), or G protein–coupled receptor 35 effects. 43
A further synthetic variant of cromolyn, known as nedocromil, is also available, at least as eyedrops to treat allergic conjunctivitis. Combining topical honey eyedrops with cromolyn and flurometholone 1% eyedrops for patients with allergic conjunctivitis was superior to conventional drugs alone in one randomized trial. 44 The Chinese herbal formula yù píng fēng săn (Jade Windscreen Powder), which contains Astragalus membranaceus (astragalus; huáng qí) root, Atractylodes macrocephala (white atractylodes; bái zhú) cooked root, and Saposhnikova divaricata (ledebouriella; fáng fēng) root, is famous for treating asthma and allergies. In an open, randomized trial, 118 Chinese adults with allergic rhinitis all used cromolyn eye drops and half of the patients also used oral Jade Windscreen Powder (doses could not be determined). 45 Symptomatic improvement was significantly better in the combination group than the cromolyn-only group.
Jade Windscreen Powder was significantly more effective than placebo for alleviating allergic rhinitis symptoms in a randomized, double-blinded trial. 46 The methylated isoflavones calycosin and formononetin from astragalus are particularly crucial to the antiallergic properties of Jade Windscreen Powder. 47 The potential immunomodulating benefits of astragalus in this formula is discussed later.
The main problem with cromolyn remains the necessity of dosing four times daily, as this substance has a short half-life. Cromolyn has also become available only through compounding pharmacies for oral use in the United States. It is thus relatively expensive. Typical oral doses are 400 mg q.i.d. Topical preparations are more readily available. A major benefit of cromolyn is its extremely low risk of adverse effects.
Quercetin and Luteolin
The flavonoid quercetin, ubiquitous in the plant kingdom, is a mast-cell stabilizer. 48,49 Quercetin was more effective at stabilizing mast cells than cromolyn in at least one in vitro study. 50 This flavonoid has many other antiallergic actions relevant for patients with eosinophilic (chronic allergic) diseases, including inhibition of: overexpression of the histamine-1 receptor; 5-lipoxygenase; cyclo-oxygenase; abnormal/excessive dendritic cell activity; excessive mucus production (without inhibiting ciliary motility); and many other actions. 51 –55
It is therefore surprising that no clinical trials were found by the current author on the effect of quercetin on any eosinophilic/mast-cell/basophilic disease. However, a trial in women with rheumatoid arthritis showed that quercetin had no effect on inflammatory or oxidative markers. 56 This trial was hampered by the low dose—just 500 mg daily—of quercetin. More typical doses are 500–1000 mg three times per day. Trials that have shown success with quercetin, including one double-blinded trial in men with chronic bacterial prostatitis, used at least 500 mg twice daily. 57 Another double-blinded trial showed that single doses of 1095 mg of quercetin could lower blood pressure in men with hypertension. 58
What complicates the clinical picture with quercetin supplementation is its complex pharmacokinetics. How an individual person processes quercetin could influence its effects dramatically, and high variability in absorption and metabolism among people makes generalizations about quercetin's efficacy challenging without considering pharmacokinetic parameters. 59 Metabolism of quercetin to quercetin-3′-O-sulfate maintains its 5-lipoxygenase inhibitory effects, while metabolism to quercetin-3-O-glucuronide abolishes it. 60 Concomitant food intakes can alter absorption of quercetin significantly; dietary fat and apple pectin both increase its absorption. 61,62 The benefits of apple pectin on quercetin absorption might result, in part, to alterations pectin induces in the gut flora, which appear to play a major role in absorption of quercetin. 63
Intake of 1000 mg per day of quercetin for 3 months has been shown to cause highly variable changes in its metabolism in healthy adults, possibly thereby altering quercetin's effects. 64 Most quercetin occurs as glycosides in food, and several studies have suggested that these glycosidic forms are absorbed better than pure quercetin. 65 This calls into question using isolated quercetin as a supplement; glycosides such as rutin may be superior.
Luteolin is another extremely common flavonoid that is very close to quercetin in structure with mast-cell stabilizing effects, both when mast cells are triggered by immune and nonimmune mechanisms. 66 –68 Luteolin is a moderately potent 5-lipoxygenase inhibitor. 69 A tetramethoxylated form of luteolin was a more potent mast-cell inhibitor than luteolin or cromolyn in vitro. 70 Not much is known about optimal dosing or clinical use of luteolin. No clinical trials in eosinophilic diseases were identified, but a small open trial in children with autism spectrum disorders who took 100–400 mg per day of luteolin combined with quercetin had modest reductions in symptoms with no obvious adverse effects other than transient mildly increased irritability. 71 Luteolin is another agent that is ready for further study for treating eosinophilic/mast-cell/basophilic hypersensitivity disorders.
Immunomodulators
A completely different set of herbal medicines, known as immunomodulators, address eosinophilic diseases by altering T-lymphocyte function, which is key to regulating the entire type I hypersensitivity/eosinophilia/mast-cell system. A well-researched example, supporting traditional use of an herb, is astragalus root, already mentioned regarding the Jade Windscreen Decoction formula. This Fabaceae family herb contains polysaccharides and triterpenoids that are believed to be crucial for modulating T-lymphocyte activity. 72
In one randomized clinical trial, Chinese children with asthma were given astragalus by itself (dose and form unknown), inhaled corticosteroids, or a combination of the two for 1 year to try to reduce recurrent attacks. 73 Astragalus and corticosteroids by themselves were equally effective; the combination of the two was significantly more effective than either in isolation for preventing attacks. Interferon-γ IFNγ levels increased and IL-4 levels decreased significantly in all three groups, compared to baseline.
A double-blinded trial on Chinese children with steroid-dependent asthma compared the effects of placebo to a nontraditional combination of equal parts astragalus, Ophiocordyceps sinensis (cordyceps; dōng chóng xià căo) thallus, Stemona tuberosa (stemona; băi bu) root, Fritillaria cirrhosa (Himalayan fritillary; bèi muõ) bulb, and Scutellaria baicalensis (baical skullcap) root in granulated form. 74 The dose was 600 mg of the formula daily by mouth, and the trial lasted 6 months. There were no differences between the herbal formula group and placebo group at the end of the trial. The low dose of the herbal formula may have played a role in its failure. However, not all combinations with astragalus are necessarily effective.
A trial involving 48 Croatian adults with seasonal allergic rhinitis randomized patients to take a combination of astragalus and calcium, magnesium, and other minerals or placebo for 6 weeks. 75 The astragalus/minerals group had significantly less rhinorrhea than the placebo group with no change in nasal eosinophil counts. This very–short-term study provided some additional support for efficacy of the immunomodulator astragalus in allergic disorders.
Typical doses of astragalus include 3–5 g b.i.d.–t.i.d. in granulated form or crude herb in a decoction, or 3–5 mL t.i.d. as a glycerite or tincture. The herb is extremely safe and tastes bland-to-mildly sweet; thus, it is very acceptable to most patients including children.
Numerous studies have shown that astragalus decreases cytokines such as IL-4 that promote Th2 lymphocyte differentiation, and this indeed leads to a shift toward higher levels of Th1 versus Th2 lymphocytes systemically in animal models of asthma. 76,77 Astragalus also has increased levels of beneficial Treg cells in a rat model of asthma, which is important, as the old model of Th2 dominance being the only lymphocyte abnormality in type 1 hypersensitivity/eosinophilic conditions is now known to be too simplistic. 78 Astragalus also inhibits nuclear factor–κB, reduces eosinophil levels, reduces goblet cell hyperplasia, and thus reduces asthma in mice. 79 Topical astragalus was effective for reducing atopic dermatitis in mice and decreasing Th2 cells and TNFα levels. 80
Other immunomodulators have shown promise in pilot clinical trials in patients with eosinophilic diseases. Cordyceps capsule has been shown to significantly reduce various inflammatory and allergic markers in patients with chronic asthma, including serum IgE, soluble intercellular adhesion molecule-1, IL-4, and matrix metalloproteinase-9. 81 Panax ginseng (red ginseng) fermented roots reduced symptoms of allergic rhinitis, compared to placebo, in a double-blinded, randomized trial. 82 A combination of Ganoderma lucidum (reishi mushroom), Chinese licorice (Asian licorice; gán căo) root, and Sophora flavescens (sophora; kuõ shēn) root was effective for reducing asthma symptoms, compared to placebo, in a double-blinded randomized trial. 83
Conclusion
Herbal medicines appear to be very promising for people with the whole range of eosinophilic/mast cell/basophilic diseases. Many herbs and herbal constituents, including those reviewed in this article, have strong evidence from traditional medicine and preclinical research that these agents will be helpful. Those that have been studied in clinical trials generally had favorable results, although not 100% uniformly. Many more agents show promise in preclinical studies (Table 1). More research is needed, but some herbal treatments should continue to be used clinically to help patients who have these difficult conditions, particularly while these patients work on eliminating or reducing exposure to triggers (mainly food allergens or aeroallergens).
Persia FA, Mariani ML, Fogal TH, Penissi AB. Hydroxytyrosol and oleuropein of olive oil inhibit mast cell degranulation induced by immune and non-immune pathways. Phytomedicine 2014;21:1400–1405; bKim HH, Bae Y, Kim SH. Galangin attenuates mast cell-mediated allergic inflammation. Food Chem Toxicol 2013;57:209–216; cKim MS, Na HJ, Han SW, et al. Forsythia fructus inhibits the mast-cell-mediated allergic inflammatory reactions. Inflammation 2003;27:129–135; dIkarashi Y, Yuzurihara M, Sakakibara I, et al. Effects of an Oriental herbal medicine, “Saiboku-to,” and its constituent herbs on Compound 48/80–induced histamine release from peritoneal mast cells in rats. Phytomedicine 2001;8:8–15; eKim DY, Lee SH, Kim WJ, et al. Inhibitory effects of Acorus calamus extracts on mast cell–dependent anaphylactic reactions using mast cell and mouse model. J Ethnopharmacol 2012;141:526–529; fKageyama-Yahara N, Wang X, Katagiri T, et al. Suppression of phospholipase Cγ1 phosphorylation by cinnamaldehyde inhibits antigen-induced extracellular calcium influx and degranulation in mucosal mast cells. Biochem Biophys Res Commun 2011;416:283–288.