
Abstract
Abstract
Background:
The third lumbar transverse process syndrome (TLTP syndrome) is one of the common causes of low back pain. There are few articles relating to TLTP syndrome published in English databases, and these few papers lack standards in outcome measurement.
Objective:
To compare outcomes for electroacupuncture (EA) vs classical acupuncture.
Design and Setting:
A prospective, randomized, controlled, patient-blinded clinical trial was conducted at M. Modern Traditional Chinese Medical Clinic in Victoria, Australia.
Participants:
Eighty patients with TLTP syndrome were entered into the study: 40 patients were randomly allocated to receive EA and 40 patients were randomly assigned to receive classical acupuncture.
Intervention:
A new method of EA was administered: local acupoints EA using the G6805- I EA stimulator. The other group of 40 patients received classical manual acupuncture. There was only 1 professional acupuncturist involved in all the treatments, using a very restricted unique treatment protocol.
Main Outcome Measures:
The pressure point pain intensity test, which was conducted by the examiner in an objective manner on each individual, was used to obtain the outcome measurement. This objective method is possibly equivalent to the blinding of assessors.
Results:
A Ridit analysis was used for this study. At the P < 0.001 level, an overall improvement occurred in 81% of people in the EA group vs an overall improvement in 42% of the control (classical acupuncture) group.
Conclusions:
The new EA method described in this study is more appropriate relative to other methods as a form of effective treatment for TLTP syndrome. Because a follow-up study could not be completed, prognosis for patients in this study with chronic TLTP syndrome was largely unknown.
Introduction
TLTP syndrome is described as muscular injuries in the third lumbar transverse process region without fracture of the transverse process. Low back pain (LBP) is the dominant symptom of TLTP syndrome. The similar clinical symptoms of protrusion of the lumbar intervertebral disk, lumbar spondylitis and spondylarthritis, and other low back conditions appear in severe cases of this syndrome. Thus, an accurate diagnosis to distinguish between such conditions would be helpful in treatment outcomes.
The conservative medical treatment is local steroid injection. 1 To understand the current status of treatments for TLTP syndrome, an updated literature search was conducted through Medline/PubMed, EMBASE, Web of Science, Cochrane Library, OVID Medline, Scopus, ScienceDirect, AMED, SpringerLink, ScienceLink Japan, J-stage, and Open J-gate. Although there were thousands of articles published on LBP, only 4 were related to TLTP syndrome in these English-language databases. Of these 4 articles, 2 were in Chinese and 2 in English, and all were published in mainland China.4-7 The literature search was also extended to Chinese databases CNKI, VIP, and Wangfangdata. There were hundreds of articles published in these Chinese databases in relation to TLTP syndrome. However, few articles met Consolidated Standards of Reporting Trials (CONSORT) or Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) standards.8–10 The existing evidence is not rigorous enough to reach a definitive conclusion in acupuncture for the treatment of TLTP syndrome.
Our aim was to conduct a quality prospective clinical study to investigate the efficacy of electroacupuncture (EA) treatment for TLTP syndrome. We also assessed whether there was a difference between this specially designed EA treatment and the classical observational experiences-based acupuncture treatment. 11
Methods
Oral consent was obtained from every patient. This study was approved by the clinic, which means that this study met all the legal requirements in Australia.
Eligibility Criteria
The preset eligibility criteria were to meet the study requirement that controls be similar to the cases. 12 The eligibility criteria were based on the descriptions by Shi 1 and Wu and Ma. 13
Inclusion Criteria
Patients had to be adults aged 18-40 years with chronic LBP on one or both sides for more than 6 months. Some patients had leg pain; however, Lasegue's sign and Bragard's sign were both negative. Patients had to have an apparent pressure pain point located in the third lumbar transverse process region; a firm soft tissue knot can be located in this pressure point region in some cases.
X-ray plain film or computed tomography scan showed that the third lumbar transverse process was longer or inclined in shape compared with the other lumbar transverse processes. Readings of x-ray films were conducted by a consultant with a senior diagnostic radiology background. Detailed quantitative data (e.g., descriptions using mm for length) for further description of the lumbar transverse process was not necessary for this study.
Patients had to have had no treatments for LBP for at least 2 weeks prior to attending the clinic. Patients could have no other identifiable diseases or causes associated with LBP. They could be receiving no ongoing treatments or intend to start other treatments such as back exercises, non-steroidal anti-inflammatory drugs (NSAIDs), or analgesics.
Exclusion Criteria
Individuals were excluded if they had LBP for less than 6 months. Patients with leg pain and positive Lasegue's or Bragard's sign were also excluded.
Those without pressure pain points located in the third lumbar transverse process region and those in whom x-ray plain film, computed tomography scan, or magnetic resonance imaging showed protrusion of the lumbar intervertebral disk, lumbar spondylitis, spondylarthritis, spondylolysis, spondylolisthesis, or other conditions that may be associated with LBP were not eligible.
Patients with other identifiable diseases or causes that might be associated with LBP were excluded, as were obese or overweight patients because the depth of penetration of needles required for treatment would differ between these patients and other patients. Therefore, the depth of needles would not be uniformly estimated for all individuals.
Also excluded were those who had any prior treatments for LBP within the 2 weeks before commencing this clinical study or patients taking NSAIDs for other conditions. Individuals with a history of acupuncture treatment were not eligible.
Procedures
The location of the clinic for this study was M. Modern Traditional Chinese Medical Clinic in Victoria, Australia. Patients who walked in to the clinic or made appointments for LBP consultations were asked to complete a simple questionnaire at reception. The simple questionnaire outlined main complaints/conditions that the patient wished to be assessed during the consultation; how long they had the condition; a brief description in the patient's own words about the condition for consult; whether they had prior treatments; and whether they had undergone x-ray or other examinations related to their condition. Selected to be examined were patients who had LBP for 6 months without a formal diagnosis, had not had acupuncture treatment previously, had not had treatment 2 weeks prior to the consultation, had not taken any NSAIDs, and met the age requirement.
A total of 172 individuals were examined; 83 of these patients met the inclusion criteria for this study. For the simplification of manual concealment of allocation, 80 patients were included in the study: 40 men and 40 women (Figure 1). Two sets of 40 envelopes numbered 1 to 40 were used, 1 set for the female patients and the other set for the male patients. The 80 envelopes were shuffled randomly. One envelope was randomly allocated to each individual in the study. Individuals allocated odd-numbered envelopes were placed in the EA treatment group (n = 40), while those with even numbers were placed in the classical acupuncture treatment group (n = 40).
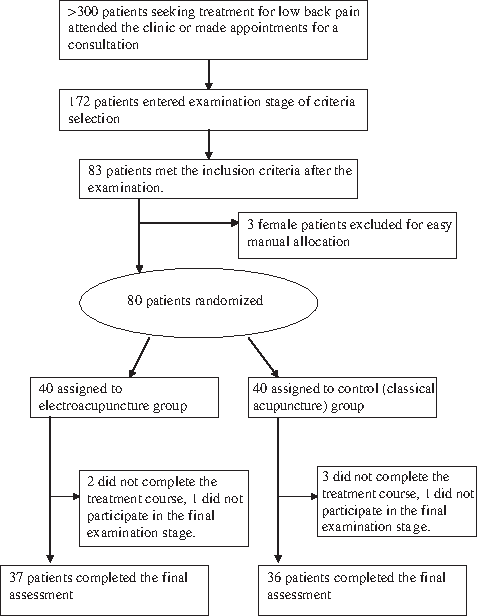
Flow chart of the study.
Treatment Protocol
The treatment protocol was developed based on expert opinion 11 and the first author's expertise. A standard treatment procedure was used for both the EA and the control group. Single-use, standard plastic guiding tubes were used for normal quick insertion. Treatment duration was 30 minutes every session, and 2 sessions were conducted per week for 6 weeks. All needles were 40 mm in length and 0.25 mm in diameter. All the needles were punctured perpendicularly with the same depth, 30–38 mm. Needles were KUN LUN, Chinese needle style, Australian Registered Therapeutic Goods (ARTG) number 148643.
The selection of acupoints for the group who received EA treatment was as follows: Ah Shi point located near the L3 transverse process; the second point was 2 cm vertically below the Ah Shi point; the third point was 2 cm horizontally away from the Ah Shi point toward the center/spine; the fourth point was 2 cm horizontally away from the second point toward the center/spine, with the 4 points approximately forming the corners of a square. A uniform approach was used for each individual in the treatment group. De Qi was not required during any of the treating sessions. EA was applied to each needle (using G6805-I, an EA stimulator: Shanghai Medical Instruments High-TECH. Co). The EA device delivered a square pulse wave with a negative-going pulse on the posterior border. The frequency used for each patient was 50 Hz with continuous waves. 14 The device's periodic time consists of 9 settings and the seventh setting was used. There are 4 different intensity settings on the device (numbered 1 to 4). The first intensity was used for all patients.
The selection of acupoints for the control group were as follows: shenshu (BL 23), qihaishu (BL 24), dachangshu (BL 25), shangliao (BL 31), yanglingquan (GB 34), and Ah Shi point, which was located near the L3 transverse process. 11 A uniform approach was used for each patient in the control group. Regardless of whether De Qi was obtained, the standard entwisting maneuver was used 8 times every 5-6 minutes in a 30-minute session for each treatment session. In a professional acupuncture consultation room in M. Modern Traditional Chinese Medicine Clinic, each electric acupuncture equipment trolley always stands near a treating bed, ready for use. This may evoke patient assumption that EA devices are to be used for their treatment.
Therapist Background
One professional acupuncturist delivered the treatments for both the EA and control group. The acupuncturist has a bachelor's degree in acupuncture and has had working experience in related fields. In theory, the therapist should be blinded. This therapist was not blinded in the true sense but because he provided uniform treatment to each individual during the treatment sessions, the uniform treatment protocol and procedures applied can be considered equivalent to the blinding of the therapist (the aim of blinding being also to ensure uniform treatment).
Assessment of Pain Intensity
An objective assessment of pain intensity was used as an outcome measurement method in this study. This objective assessment was measured through a standard orthopedic physical examination. Pain intensity assessment required patients to report the degree of severity of induced pain or severity of tense feeling during the clinical examinations, the pain being objectively induced by the examiner. These patients were asked to indicate the pain severity after feeling the pressure induced by the examiner's finger in a 4-degree/scale pain intensity test. Tests were repeated 3 times in the same area/point for results to be more reliable, and a final score was recorded. If the patient indicated the same pain degree of pain 2–3 times, this score was recorded as the final score. This final score was not a mean or median score, meaning that those pressure pain points that could not be repeatedly induced were excluded. These objectively induced, subjectively recorded pain scores were recorded once during the first and again during the last consultation. The scores were recorded before the commencement of treatment and after the 12-session course of treatment finished, with the results compared. The details of the 4-grade pain test used to compare the pain status before and after treatment is as follows:
The first grade: since before treatment, whether the pressure pain point has disappeared–yes or no The second grade: since before treatment, whether the degree of the pain of the pressure pain point has improved–yes or no The third grade: since before treatment, whether there have been changes in pain in the pressure pain point– yes or no The fourth grade: whether the pain in the pressure pain point is more intense than before treatment–yes or no.
Statistical Analysis
Ridit (relative to an identified distribution) analysis was used for this study (Table 1 shows detailed data listings and calculations).
R, ridit in progress.
Results
At the P < 0.001 level, 57% of participants in the group who received EA indicated that the pain of the pressure pain point had disappeared, 21% of participants indicated that the pain of the pressure pain point had improved, with an improvement in around 81% of participants overall. In contrast, only 11% of those in the group receiving classical acupuncture indicated that the pain point had disappeared, 31% indicated improvement, with an improvement of around 42% overall.
Discussion
A Practical Method for the Assessment of Pain
The visual analog scale (VAS) and the Numerical Pain Rating Scales (NPRS) are commonly used in almost all clinical trials on LBP to assess patient pain because they are subjective pain outcome measurements that emphasize patients' subjective feelings. VAS and NPRS may be less accurate as clinical outcome indicators for TLTP syndrome and thus were not used in this study. Instead, another method was used, the objective pain intensity test. The pain intensity test has a clinical advantage in assessing clinical outcomes because we found a direct association between pressure pain point and clinical pain symptoms in TLTP syndrome. The more severe the pain symptoms, the more induced pain was felt when pressure was applied to the pain points and also, the less severe the pain symptoms, the less induced pain was felt when pressure was applied to the pain points.
Patients were blinded in this study. All the patients were aware that they would receive one of the forms of acupuncture treatment (no details of treatments were given). Because all patients involved in this study had no previous acupuncture treatments, patients did not have knowledge about detailed manual or EA treatments nor the sorts of feeling that should or should not be produced from such treatments. All the patients lay face down with their head resting on massage/treatment beds and could only see the floor and thus would be oblivious to the detailed treatment process on their back during treatment sessions. An EA equipment trolley stood near every treating bed ready to use; patients did not know whether any of the devices on the trolley would be used in any treatment sessions. In addition, clips and wires used with the G6805 EA device are light, almost 3–4 times lighter than the smallest clips and wires commonly used with most EA devices. Thus, patients were not aware of whether clips and wires were attached to needles located in their back. For this study to better match the standard of drug studies, we tried to blind patients in the study design. However, this study involved physical treatments, for which complete blinding is more difficult than for pharmacological studies. Nevertheless, this blinding method is better or at least equivalent to blinding methods published in current acupuncture papers.14,15 However, the assessor was not blinded because blinding the examiner was not possible since the examiner needed to perform the pain intensity assessments, which were physical examinations. The main aim of blinding assessors is to avoid the Rosenthal effect. Because of the designed objective nature of the pain intensity test, the Rosenthal effect involved in pain data recording is highly unlikely to have occurred.
Rational Design of Pressure Pain Points-Based Assessment
In addition to its practicality in clinical settings, the application of pressure pain point assessment is based on anatomy and pathophysiology and most importantly, the biomechanical characteristics of TLTP syndrome.
Generally, the third lumbar transverse process is the longest transverse process compared with the rest of the lumbar transverse processes. This is the likely reason that radiologists usually do not report specifically about the third lumbar transverse process. In addition, there is a lack of English literature in this area, which discourages radiologists' reports. If we review the definition of TLTP syndrome, it is about soft tissue injuries and radiologists do not usually describe soft injuries in their reports. Our main aim of x-ray examinations was to exclude fractures of the transverse processes and other conditions such as spondylarthritis that may be associated with LBP.
There are many blood vessels and nerve bundles crossways at the extremity of this process. Also, there are many lumbar myofascial tissues attached to this process (i.e., myofascial tissues of sacrospinal muscle, lumbar quadratus muscle, and abdominal external and internal oblique muscles). The third lumbar is in the center (center of the arc line) of the physiological forward alignment of lumbars. Repeated bending and lifting results when one side of the lumbar muscles contract while the other side of the lumbar transverse processes act as a lever, which results in a large range of movement, especially in the longest process, the third lumbar transverse process. 1 To avoid injuries to muscles and fascia tissues attached to the transverse process, the surrounding muscles have to act as supports. However, the supports may sometimes be compromised and injury occurs as a result. In addition, the third lumbar transverse process has a unique anatomic structure: “lumbar quadratus muscle-lumbar sacrospinal muscle-branches of lumbar nerves.” This structure consists of the “lumbar quadratus muscle and lumbar sacrospinal muscle,” “branches of lumbar nerves,” and “the extremity of the third lumbar transverse process.” Such a structure is identified as the “muscle-nerve-skeleton junction” and can cause more clinical symptoms including pain when injury occurs. 1
That the pressure pain point exists in the third lumbar transverse process area is direct clinical evidence because it is closely linked to the nature of the injury. Thus, to measure the pressure pain point directly and objectively is the key for outcome measurement.
Interpretation of the Results
The results showed that there was statistically and clinically significant differences between the group that received EA and the group that received classical acupuncture (the control group). Chronic injuries and inflammation around the third lumbar transverse process region is the fundamental cause of TLTP syndrome. EA relieves inflammation and promotes local tissue blood flow. 16 The direct EA treatment in the third lumbar transverse process area had such effects, providing effective inflammation relief and possibly prompted the progress of local soft tissue healing. In contrast, the classical method used in the control group was different; most acupoints were far from the injury site and only one needle was directly applied to the third lumbar transverse process region. Such selections are likely to provide more pain relief.17,18 However, these selections might be less likely to provide effective local soft tissue healing.
Advantages and Disadvantages of Simplification of Treatment Procedures
For the purpose of the reduction of variables, uniform treatment methods were applied in treatment procedures for all cases by 1 therapist only that greatly reduced the impact of the lack of blinding of the therapist. In the group receiving EA, a uniform treatment procedure was used. A similar standard applied to the group receiving classical acupuncture. There was no De Qi effect obtained in either group because to obtain De Qi, the therapist would have had to perform manipulative techniques, which would have resulted in variations between patients in terms of the differences in the sorts of manipulations, the frequency, length of time of manipulation, or the depth and angles required to achieve the status of De Qi in each individual. Moreover, with regard to the EA group, because of the characteristics of EA, De Qi does not need to be obtained routinely in this particular therapy, as documented by Wang. 12 For the group receiving classical acupuncture, an alternative method instead of obtaining De Qi was used, producing almost no variations in treatment between patients. The therapist involved in this study applied a uniform and simplified twisting method 8 times every 5-6 minutes regardless of patients' response or De Qi status obtained. The disadvantage of this approach was that in some patients, the status of De Qi may not have been achieved through twisting the needles 8 times, which may have produced lower effectiveness in treatment. Conversely, twisting may produce too much stimulation for some, producing more effective treatment. However, the advantages outweigh the disadvantages. This uniform treatment method was fit to the purpose of this study well and likely enhanced the generalizing ability.
Limitations
Most studies use a range of supplementary subjective indicators such as the Short-Form 36 health scale score to compare baseline characteristics such as race, age, etc. Only a description of patient age was given in the method section, and no further detailed study about baseline characteristics was conducted because this study was based on ''pay for service' Australian acupuncture clinical settings and there were no further resources or time available to broaden the scope of this clinical study. This was one of the limitations of the study.
Low back pain is one of the main symptoms of TLTP syndrome. Patients with chronic LBP symptoms were selected for this study. Since it is a condition that lasts over 6 months, ongoing or recurring symptoms are characteristics that reflect the uncertainty of chronic TLTP syndrome. To achieve better outcomes, a follow-up at least 6 months after symptoms resolve is needed. For a typical clinical study conducted in clinical environments in the State of Victoria, Australia, and based on a health services–regulated status (especially user-paid service consultations), there were difficulties in scheduling follow-up appointments 6months after the completion of a 12-session treatment course to examine pressure pain points in participants. In addition, a 6-month follow-up consultation was not approved by the clinic manager because a follow-up consultation may not be needed by all patients from a medical viewpoint and thus, requesting a paid follow-up consultation for each participant would not be justified. Therefore, follow-up studies were not conducted. This was a limitation of the study; for example, some uncertainties were present, such as whether there would be any differences in treatment outcomes between groups 6 months after the completion of treatment; the length of time that the outcome achieved by acupuncture might last; whether recurrences would occur within 6 months after treatment; the rate of recurrences; and whether there was any association between recurrence and a new episode of another condition of LBP or a newly developed episode of TLTP syndrome.
Another limitation is that this study is unable to provide further details in the area of “knot” and the clinical symptom of pain. Some patients had a firm soft tissue knot located in the pressure pain point region. This soft tissue knot might be a form of chronic soft tissue inflammation in which local soft tissues try to maintain function by limiting the spread of the inflammation, resulting in the knot phenomenon. There is lack of information in the literature about the association between the soft tissue knot and clinical pain symptoms. Thus, this study ignored the knot phenomenon in clinical outcome measurement. However, whether the existence of the knot would play a role in the rate of recurrence in the future remains unstudied.
Low back pain is a dominant symptom of TLTP syndrome. Although there are thousands of papers published in the area of LBP research in English databases, few consider that one of the causes of LBP is TLTP syndrome. The few already published were lacking in standards in terms of outcome measurement in the study of TLTP syndrome. This study adopted objective measurements, pain (pressure pain point) intensity test as a clinical outcome measurement method, which is more advantageous due to accuracy, and which is at least equivalent to the method of blinding assessors for VAS or NPRS subjective measurements.
From this randomized clinical study, there was a statistical and clinical difference between EA treatment and classical acupuncture treatment after the completion of a 12-session treatment course. Thus, the new method described herein is more appropriate than classical methods as a form of effective treatment for TLTP syndrome. Because a follow-up study could not be completed, the prognosis for patients with chronic TLTP syndrome is largely unknown.
Footnotes
Disclosure Statement
No competing financial interests exist.