
Abstract
Abstract
Acupuncture originated in ancient China but is used around the world to treat a variety of diseases. Research has not provided conclusive evidence proving the existence of meridians, or the lines along which acupuncture needles are inserted. Currently, some members of the scientific community recognize the existence of acupuncture points but not of the meridians. Thus, when acupuncture is accepted, it is regarded as a suitable treatment for some symptoms and diseases, but its effectiveness is ascribed directly or indirectly to the nervous system. Gross anatomy is the discipline upon which scientific biomedicine is based, and the author uses juxtaposition to compare the shapes of the 12 main meridians with the anatomical shapes of their related organs; this comparison has revealed similarities that are worthy of consideration. This article discusses similarities between the shape of the Large Intestine and Kidney acupuncture meridians and the anatomy and embryology of the colon and urogenital tract in humans and other animals. Verification of these and other morphological similarities by human and comparative anatomists, geneticists, and biologists would support the hypothesis that meridians are involved in embryonic morphogenesis, extrauterine development, and the conservation of health. Such a possibility should increase scientific interest in the biophysical existence of meridians and prompt research that applies this new perspective to novel experimental projects.
Introduction
This disconnect has generated an intellectual divide between traditional Chinese acupuncture and medical acupuncture, whose rationale has been outlined in the form of a manifesto by White and the editorial board of Acupuncture in Medicine. 1
Gross anatomy is the historical and factual basis of scientific medicine. It encompasses everything in the human body that is visible to the naked eye as well as areas that are visible through instrumental and surgical exploration and in cadavers through anatomical dissection; that is to say, gross anatomy includes all organs, structures, and portions thereof. The branches into which anatomy is divided, such as cytology and histology or radiology and endoscopy, have their roots in gross anatomy. These branches involve the study of organs with microscopy and make normally invisible cells and tissues visible by means of dyes and contrast media. Other disciplines, such as physiology, biochemistry, and genetics, also have their origins in the study of gross anatomy.
The Acupuncture Meridian System
Acupuncture involves the insertion of metal needles into the skin at specific points located on the superficial paths of meridians, which are also known as channels or vessels. It is the best known therapeutic method used in Traditional Chinese Medicine (TCM) for the treatment of meridians; other methods include manual or instrumental massage, heating, cupping, bleeding, herbal therapy, and electrical stimulation.
According to the TCM sources discussed by both Chinese authors—such as Deng and colleagues 2 and Li 3 —and Western authors—such as Maciocia 4 and Deadman and colleagues 5 —the meridians are organized into a circuit through which blood and Qi flow in variable proportions. Qi is a multipurpose principle having no analogue in modern scientific and biomedical terminology; the term is translated using expressions such as vital energy or vital force. The acupuncture meridians form a network that is distributed throughout the body. In this perspective, the current author considers only the main or regular meridians that, according to TCM, depend on specific organs. When necessary, details are provided for two of the eight Extraordinary or “Curious” meridians. The names and alphanumeric abbreviations used in this article to identify acupuncture meridians and points are those established by the Standard International Acupuncture Nomenclature source. 6 Table 1 shows a schematic of the subdivisions of the meridian system.
There are 12 main meridians that form the basis of the aforementioned circuit. Each of them is linked to a specific thoracic or abdominal organ; to a specific coupled organ; a specific area of the head, trunk, or upper or lower limb; and a specific finger or toe. For example, the Lung meridian depends on the Lung organ, and it is coupled with the Large Intestine organ. In the head, the meridian path spreads into the throat, nasal, and frontal regions, then runs along the anterior-lateral side of the upper limb and thenar eminence and ends at the lateral angle of the thumb. Only the 12 main meridians and two of the eight Extraordinary meridians, the Governor Vessel (Dumai) and the Conception Vessel (Renmai), have their own points. The remaining six Extraordinary meridians and all secondary meridians have their paths organized along the points of these main meridians.
The 12 main meridians continue, one after another, in the circuit outlined above; Qi “flows” through this circuit following the circadian rhythm, with maximum and minimum peaks lasting 2 hours for each meridian and organ. Published timetables have identified the organs from which the 12 main meridians derive their names: Lung (LU), Large Intestine (LI), Stomach (ST), Spleen (SP), Heart (HT), Small Intestine (SI), Bladder (BL), Kidney (KI), Pericardium (PC), Triple Energizer (TE), Gall Bladder (GB), and Liver (LR).
It must be said that, among the 12 main acupuncture meridians, the Triple Energizer is the only one whose name does not correspond to the name of an anatomical organ. However, it can be reasonably linked to the Duodenum, an organ that objectively has three interconnected functions: (1) the production and excretion of alkaline duodenal fluid; (2) the collection and excretion of bile produced by the gall bladder; and (3) the collection and excretion of enzymatic fluid produced by the exocrine pancreas.
Table 2 shows the circuit with the corresponding time of each meridian, the finger or toe, and the regions of departure and arrival. Based on this daily circuit, the 12 meridians are paired according to two different criteria: the Yin–Yang (or Solid-Hollow; see below) reciprocity of the corresponding organs and the notion that two successive meridians of the same nature, Yin or Yang (or Solid or Hollow), in the arm and in the leg form a Yin or Yang Great Meridian (GM). With this pairing, the 12 meridians are reduced to 6 meridians.
Notes: Arrows represent passage from one meridian to another meridian. Time units are shown for 24-hour cycle. Yang meridians are shown in italics.
Topography of the Meridians
The 12 main meridians are named after the organs to which they belong and are classified by TCM into groups of three according to the position of the paths in the superior and inferior limbs, taking as a reference an adult in the orthostatic position of topographic anatomy. There are three meridians on the anterior aspect of the forearm (Lung, Pericardium, and Heart), three meridians on the posterior aspect of the forearm (Large Intestine, Triple Energizer, and Small Intestine), three meridians on the medial aspect of the leg (Liver, Spleen, and Kidney), and three meridians on the lateral aspect of the leg: Stomach, Gall Bladder, and Bladder). The current author prefers to use the anterior–posterior and medial–lateral anatomical terms rather than the “Yin and Yang of hand and foot” terms traditionally used in Chinese medicine, because these traditional terms are alien to scientific biomedical nomenclature (Table 3). Alternatively, we could adopt the negative and positive terms derived from electromagnetism; however, at the moment, there is no basis for defining the Liver as negative (Yin) or the Gall Bladder as positive (Yang), although the two organs are strictly connected anatomically and physiologically. A fortiori, this is also true for other pairs of organs, including the Lung/Large Intestine and the Heart/Small Intestine pairs, which have neither an anatomical contiguity nor an apparent physiological complementarity. It should be noted that, while Chinese tradition distinguishes the 12 main meridians as being Yin or Yang, this tradition classifies the 12 organs as Solid (Zang) or Hollow (Fu), which corresponds more rationally to their intrinsic anatomy; an exception to this is the case of the Pericardium (Table 4). However, while the Solid–Hollow criterion is adequate for organs, it is not appropriate for meridian lines. If the Yin–Yang criterion did not have a strong metaphysical connotation, it would be suitable for both meridian lines and their related organs.
Yang meridians are shown in italics; thus, for clarity Yin Chinese names are not in italics.
int., at the ulnar/peroneal side; ext., at the radial tibial side.
There is some question regarding whether or not the Pericardium is solid; it is an exception to the normal classifications used.
Research in Acupuncture
As reported by Hsu, 7 the first significant detailed description in Latin of the meridian system and acupuncture points was written by ten Rhyne. 8 This work was preceded by dissertations written by De Bondt 9 and Cleyer, 10 and followed by an extensive article written by Kaempfer. 11 While these works were all written in Latin, Heister12,13 soon included a major chapter on acupuncture in two of his German language books on surgery. More than half a century later, the first volumes entirely dedicated to this subject appeared in French, 14 Italian, 15 and English. 16
Interest in acupuncture in the scientific literature coincides curiously with the publication of the article “Case of Anasarca Successfully Treated by Acupuncturation [sic]” in the debut issue of The Lancet. 17 According to a recent statistical review, 18 current research in acupuncture is primarily clinical. Such research aims to assess the effectiveness of acupuncture in patients with specific diseases and includes double-blinded methods and placebo needles.19,20 Conceptually, this research is distinguished from that performed in the past because it is supervised through effective, if debatable, Cochrane reviews. 21 Such clinical research can affirm or deny the usefulness of acupuncture as a therapy, but it adds nothing to our knowledge of the meridian circuit in terms of anatomy.
Beginning with a study by Nakatani 22 * and a scientific doctoral thesis by Niboyet, 23 and ending with the final review of electroacupuncture (EA) by Voll, 24 extensive studies on the electrical characteristics of acupuncture points and meridians have been performed; moreover, dozens of devices have been developed to diagnose the healthy and pathological status of these points and meridians. There has been criticism of these developments as well, especially with regard to the skin electrodiagnosis of allergies (see Lewith and colleagues, 25 and Semizzi and colleagues). 26
Colbert and colleagues 27 meticulously summarized the history of the electrical measurement of acupuncture points and launched a project to build a device for the optimal recording of the electrical activity of these points over 24 hours.
In addition to EA, many other experiments have been conducted by researchers from the Soviet bloc and widely documented by Dumitrescu, 28 who went so far as to use electronography, an astronomy technique, to obtain images of acupuncture points and measure their dimensions. Unfortunately, these works are no longer easily available to interested readers because they are written in Russian or other Eastern European languages or are out of print and not indexed by PubMed. However, beyond the real or presumed objectivity of the electrical properties of acupuncture points and meridians, this research focused on physiology and never provided indirect anatomical evidence for the existence of meridians.
Researchers have also attempted to verify, at the microscopic level, the existence of meridians and points whose existence remain uncertain at the macroscopic level. Kim 29 published research that was especially controversial. With the aid of an optical microscope and following a special staining protocol, he described certain threadlike ducts, subducts, and corpuscles possessing new histological and cytological characteristics that were distinct from those of blood and lymphatic capillaries, and that he identified as being equivalent to meridians and acupuncture points. The body of structures he claimed to have disclosed is called the Bonghan System, after Kim's first name. Despite its importance, the author kept the staining formula a secret, and it was only after more than 40 years that the ducts and corpuscles corresponding to his descriptions were highlighted using alcian blue and especially trypan blue staining and could thus be confirmed by other researchers in rats and rabbits. These works, with extensive bibliographies and detailed descriptions of the materials and experimental methods, were reported in a study by Shin and colleagues 30 and in an exhaustive review by Soh. 31 In agreement with Kim's data, 29 these authors found a network of threadlike transparent ducts (diameter ∼ 20 μm) punctuated with larger corpuscles (d ∼ 100 μm) and located everywhere in the body: outside and inside the skin; in blood and lymphatic vessels; and in various internal organs, such as the brain, spinal cord, and nerves. Corpuscles and ducts are linked either to one end or to both ends of these systems. Anatomically speaking, they are relevant to no specific organ or apparatus. Strangely, they can be stained by trypan blue, a dye that is commonly used to discriminate between alive and dead cells.
The first announcement of proof of the existence of meridians following the experimental injection of the radioactive tracer TCm-99 into an acupuncture point was made by De Vernejoul, et al. 32 This was resoundingly discredited by Bader 33 in the pages of Science et Vie, a popular leading French scientific journal, and later by the work of Simon and colleagues. 34 Other studies that featured the same and different radioactive tracers followed over the years, but none of them reported a conclusive or consistently repeatable discovery of the studied meridian paths.
In addition to the diffusion of radioactive tracers, the propagation of light along the meridians has been studied. For example, Choi and colleagues 35 measured the propagation of light emitted from a tungsten halogen lamp between two points of the Pericardium meridian and between one of these points and another point outside of the meridian—all situated on the forearm. The light propagation was found to be 20% greater between the two points of the same meridian, compared to the propagation between the meridian and the nonmeridian point.
In close connection with the recently republished fundamental research of Pischinger 36 on the extracellular matrix of connective tissue, Heine37–39 studied the microscopic anatomy of acupuncture points and found that points located on the meridians had different histological and morphological characteristics than points located outside the meridians. In the tissues underlying the acupuncture points, Heine 37 found that the neurovascular bundle crossed the fascia carrying a cylinder of proteoglycans from the extracellular matrix. Physical shock and pressure absorption are among the many functions of connective tissue mentioned by Heine, and these functions may depend on the cylinder of proteoglycans. This hypothesis is consistent with that of one study that examined the points and meridians with respect to the connective-tissue planes 40 and of another that equates meridians with myofascial chains. 41 In addition, the synchrotron is now being used in acupuncture research: Yan and colleagues 42 examined the elemental composition of acupuncture points and demonstrated that points along the meridians have a different mineral content than nonmeridian points and that the shape of meridian points is elliptical, with the major axis oriented along the direction of the meridian.
Other research has focused on the effects of basic acupuncture, 43 EA,44,45 and infrared laser stimulation with placebo 46 on the activation of specific brain areas using (functional magnetic resonance imaging (fMRI). Despite criticisms of the experimental design 47 and procedures 48 of these studies, the use of fMRI falls within the field of neurophysiology. While fMRI is useful for clarifying the links between specific points of the skin and the functions of specific brain areas, fMRI does not connect the acupuncture system with visceral anatomy.
Another area of research has examined the application of moxa (mugwort; Artemisia vulgaris) and infrared lasers to the meridians, followed by observation with an infrared camera. The experiment performed by Schlebusch et al., 49 who claimed to have the first reported evidence of the structure of acupuncture meridians in the human body, was subsequently proven wrong by Litscher. 50 Two years later Yang et al. 51 claimed to have identified, again using an infrared camera, the paths of the 12 main meridians plus the Governor and Conception Vessels corresponding to the warm lines spontaneously emitted from the bodies of healthy volunteers without the application of any external heat source. These findings have not been contradicted by other researchers. In the same study, these authors outlined steps for the improved management of such experiments.
Finally, it is worth mentioning the simplest experiment that, when repeated on a large scale and confirmed by other authors, could provide strong evidence for the biophysical existence of acupuncture meridians. Narongpunt and colleagues 52 manually stimulated point BL 2 of the Bladder meridian, which is located at the tip of the medial eyebrow. After a few seconds of stimulation, an infrared camera revealed the warming of point BL 67 of the same meridian, located at the ungueal outer side of the fifth toe in the ipsilateral foot. The authors stated: “Unknown neurovascular effects of the organism may explain the high-speed thermal activity on the dorsum foot point BL 67. The mechanism is unknown but measurable.” 52
We may conclude that no result has thus far allowed scientists to identify meridians with specific anatomical structures. Meridians do not correspond to the nerves of the central nervous system or to the autonomic nervous system, although Quaglia Senta 53 produced an interesting work with regard to the latter. Moreover, meridians cannot be identified as being identical to either the blood or lymphatic vascular structures. No repeatable routine test, such as an ultrasound scan or magnetic resonance imaging scan, has yet been able to certify that the thumb is related to the arm and thus to the lung; in contrast, the primary thumb artery is anatomically related to the brachial artery and thus to the heart.
Therefore, acupuncture lacks the unquestionable evidence of gross anatomy to which, according to the medical Chinese tradition, the meridian system makes explicit reference, namely “channels” deriving from specific organs and connecting specific regions and starting from or ending at the medial or lateral side of a specific finger or toe. For this reason, the current author has initiated a morphological comparison between the paths of individual meridians and the gross anatomy of the referred organs.
Comparison of Meridian Paths and Gross Anatomy of Referred Organs
The general morphological characteristics of the 12 main meridians of acupuncture were studied and described with a focus on changes in paths (i.e., lateral deviations, inversions, and crossings or intersections). The images of the changes in the meridian paths were compared, through a juxtaposition with the findings of gross anatomy, to images of the organs to which the meridians are said to pertain. Images were placed side-by-side on a desk or computer screen. The normal human gross anatomy of an adult individual and an embryo were used; for comparative anatomy, the anatomy of domestic animals and a cetacean were used. The study material was not designed precisely for this work; the descriptions, drawings and figures used for this purpose had been previously published.
The drawings of adult human figures were taken from the following books: An Outline of Chinese Acupuncture, 54 Chinese Acupuncture and Moxibustion, 2 and Acupuncture, Meridian Theory and Acupuncture Points. 3 These drawings were used to study the acupuncture meridians, whose paths were reconstructed with the vectorial tools of the drawing software Macromedia Fireworks, version: 8.0.0.777. This reconstruction of the hand-drawn meridian paths was necessary to reveal the uniformity of all lines and points. Drawings were created by tracing the lines and points of the meridian figures.
The books, atlases, and other resources used for the juxtaposition of the drawings of the meridians and the anatomical images were the following: Anatomia Umana (Human Anatomy, vol. 2) 55 ; Atlante di Anatomia Descrittiva Dell'uomo (Atlas of Descriptive Anatomy of Man, vol. 2) 56 ; Atlas of General Zoology 57 ; The Development of Animal Form: Ontogeny, Morphology, and Evolution 58 ; Anatomy, Descriptive and Surgical 59 ; Hyman's Comparative Vertebrate Anatomy 60 ; Vertebrates: Comparative Anatomy, Function, Evolution 61 ; Color Atlas of Veterinary Anatomy: The Dog & Cat, vol. 3 62 ; Whales, Dolphins, and Porpoises 63 ; Atlas and Dissection Guide for Comparative Anatomy 64 ; Principles of Comparative Anatomy of Invertebrates: Promorphology 65 ; and Invertebrate Zoology: A Functional Evolutionary Approach. 66
Results of Exploration
General Morphology of the Superficial Path of the 12 Main Meridians
Each of the 12 main meridians consists of a right and a left symmetrical branch and a superficial and a deep path. The superficial path is drawn as a solid line with a starting point, an end point, and intermediate points. The deep path is drawn as a dashed or dotted line. It can be an extension of the superficial path and can precede the starting point or follow the end point. In addition, the deep path is detached from the superficial path through one or more branches, starting from a certain point and entering the body, while the superficial path resumes its trajectory. The deep path can terminate within the body or may re-emerge to rejoin the superficial path. Unlike superficial paths, deep paths either do not have acupuncture points or are not represented, possibly because of the danger involved in treating these points with needles. In ancient and modern texts, descriptions of superficial paths are more detailed than those of deep paths, which are minimal and include no specification of their distribution in the organs.
Generally, the main meridian pathways are straight or curved lines that trace the forms of the covered anatomical regions. Each meridian is composed of a single line, with the exception of the Bladder meridian on the back. Instead, in passing from the neck to the chest, the Bladder meridian splits into two lines, medial and lateral, which descend parallel to the spine up to the level of the fourth sacral foramen. From here, the two lines diverge, then cross at the posterior and inferior third of the thigh, and finally meet at the popliteal fossa. The paths of different meridians can remain parallel to each other, diverge or converge to meet or cross. The best-known crossing is that of Spleen point SP 6, whose Chinese name is Sanyinjiao (Meeting of the Three Yin), on the internal face of the lower third of the leg, where the meridians of the Spleen, Liver, and Kidney approach until they touch each other. The only case of crossing between the right and left branches of a meridian is that of the Large Intestine. Coming from the shoulder and reaching the cheek, each branch crosses the medial line and arrives at the opposite side of the nose. In all other meridians, each branch runs along a single side of the body. According to the time circuit described above, the direction of the main meridians alternates from centrifugal (from head or trunk to a finger or toe tip) to centripetal (from a finger or toe tip to trunk or head).
Starting from a given point, the meridian path can deviate with a variable angle, from a few degrees (for example, between Kidney points KI 21 and KI 22) to 45° and 90° (between Bladder points BL 57 and BL 58 and between BL 39 and BL 40, respectively) or higher (between Small Intestine points SI 18 and SI 19). The direction inverts twice in the leg path of the Stomach meridian (between points ST 39 and ST 40 and between ST 40 and ST 41; Fig. 1) and four times in the Gall Bladder meridian path on the lateral aspect of the skull (between GB 2 and GB 3, GB 4 and GB 5, GB 12 and GB 13, and GB 14 and GB 15). The Small Intestine meridian presents four consecutive deviations in opposite directions, forming a zigzag path over the shoulder region between the upper margin of the trapezius muscle and the posterior axillary fold (SI 10 and SI 11, SI 11 and SI 12, SI 12 and SI 13, and SI13 and SI14; Fig. 2).
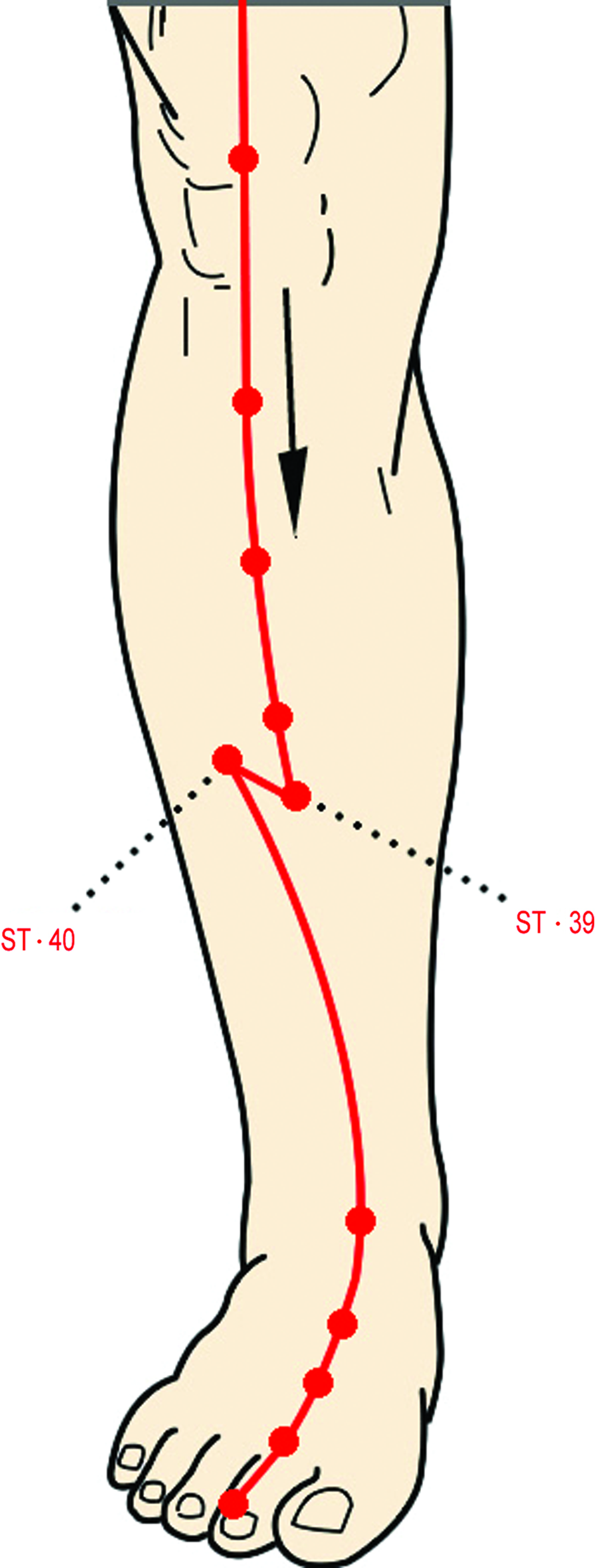
Double inversion of the Stomach meridian path in the leg. This occurs at points ST 39 and ST 40, and ST 40 and ST 41. This may be interpreted as a motion vectorial representation for flexion-extension of the foot on the leg. Color images available online at www.liebertpub.com/acu
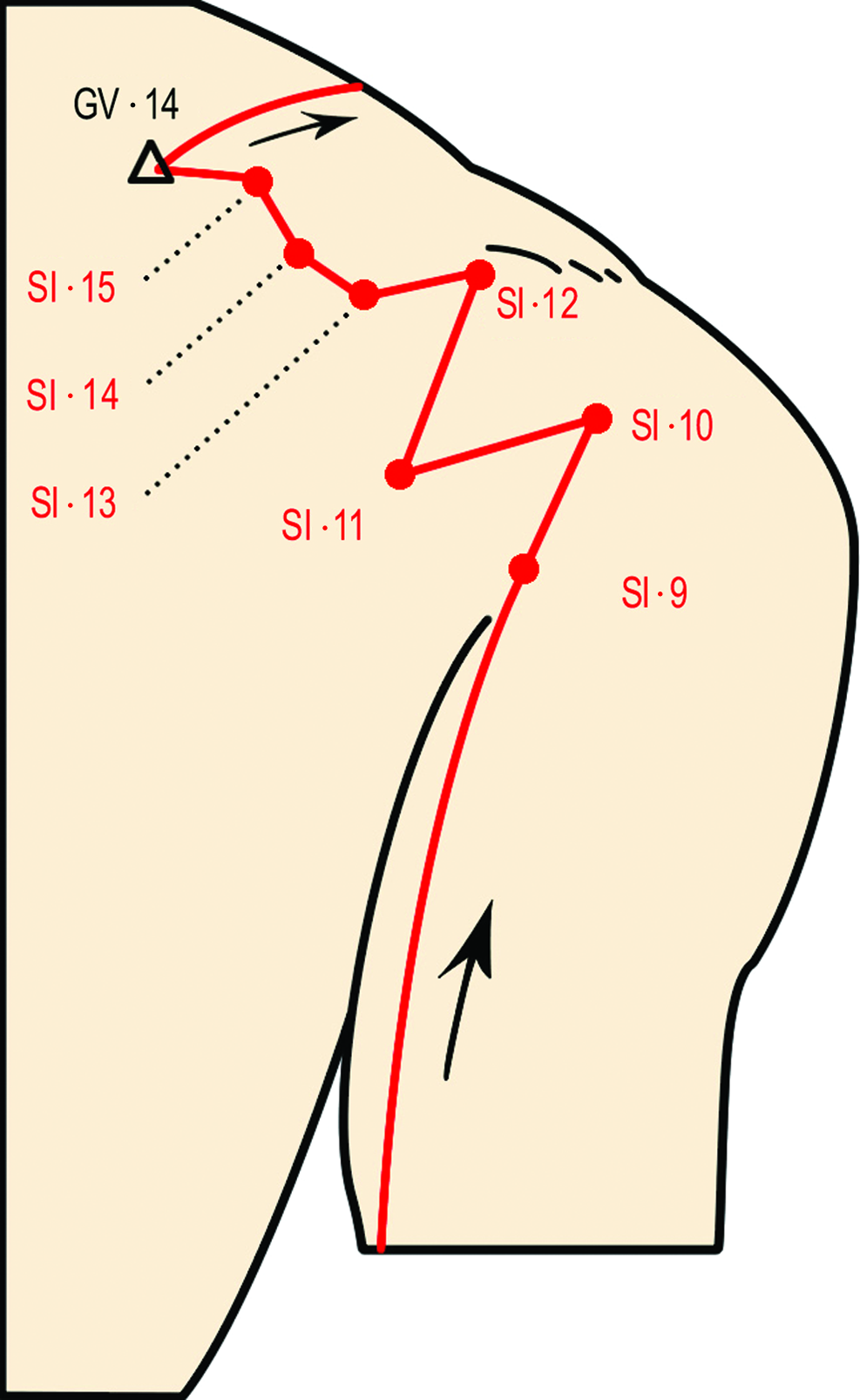
Four consecutive path inversions of the Small Intestine meridian on the shoulder, forming a zigzag path. Color images available online at www.liebertpub.com/acu
The path of the Kidney meridian is unique in shape. In the transition from the sole of the foot to the medial side of the leg, this meridian makes four successive deviations (between points KI 3 and KI 4, KI 4 and KI 5, KI 5 and KI 6 and KI 6 and KI 7; Fig. 3). Here, and in any other meridian, all of the deviations occur in the same direction, clockwise for the right foot and symmetrically counterclockwise for the left. The fourth and last deviation crosses the meridian segment from which the first deviation occurs, restoring the upward direction. Thus, the shape of a circle or of an irregular quadrilateral polygon is formed.
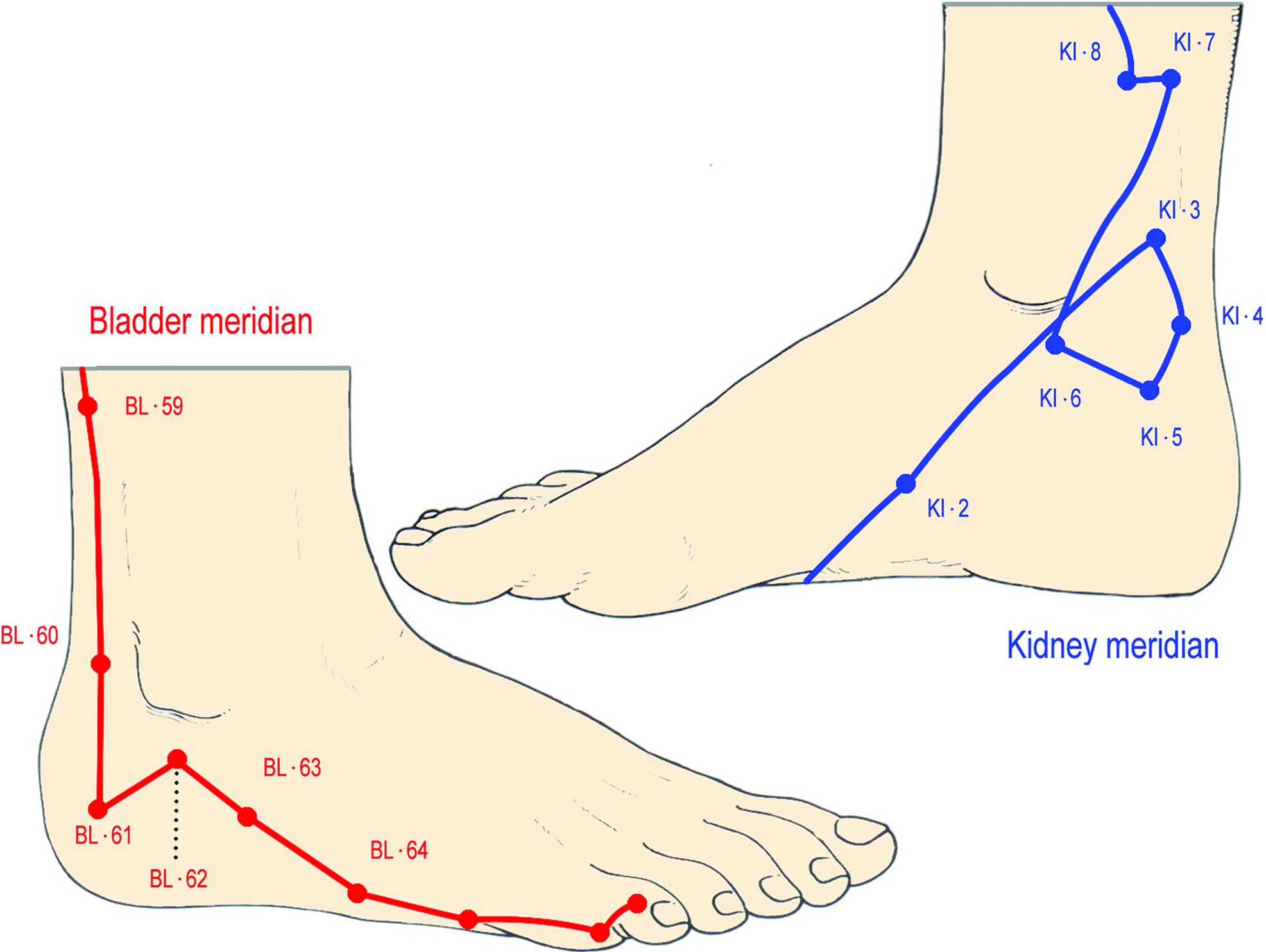
Four consecutive path deviations of the Kidney meridian on the foot medial aspect. They occur all in the same direction and forming a shape of circle or irregular quadrilateral polygon, which the Bladder meridian on the lateral aspect does not show. Color images available online at www.liebertpub.com/acu
Crossing of the Two Large Intestine Meridian Branches and Decussation of the Pyramids
The crossing of the right and left branches of the large intestine meridian occurs between the upper third and the lower two-thirds of the philtrum, or nasolabial groove. Figure 4A shows the final portion of the Large Intestine meridian on the neck, jaw, and upper lip. Each branch moves to the opposite side to finish at the wing of the nose (point LI 20). The point where the two lateral branches intersect belongs to the Dumai or Governing Vessel (point GV 26), which is one of the eight Extraordinary meridians whose superficial path follows the posterior midline from the apex of the coccyx upward along the spine and the skull up to the mucosa between the two maxillary central incisors, where this meridian terminates (Fig. 4B).
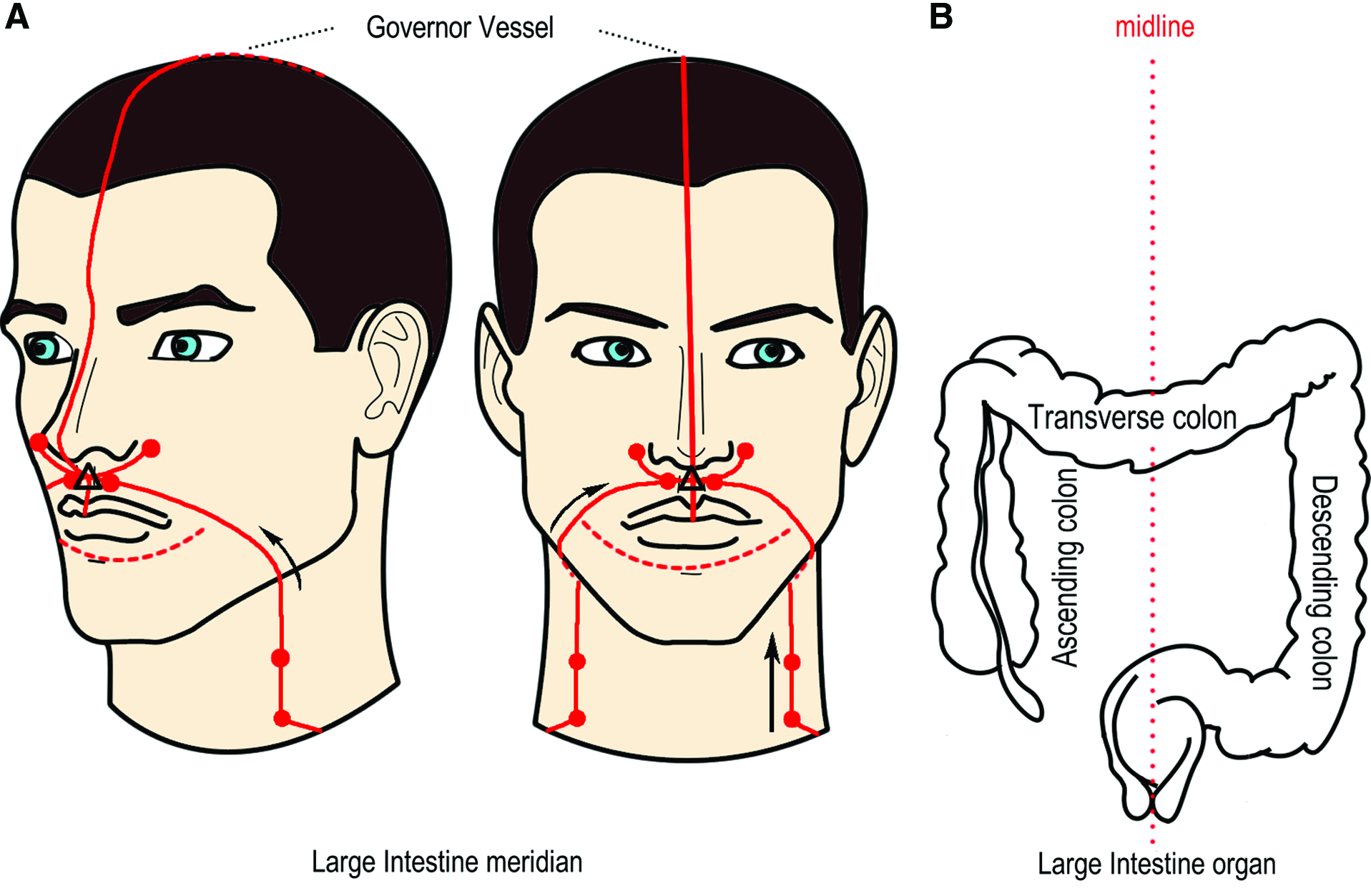
The meridian of the Large Intestine on the face and the anatomy of the colon.
With the skull in the position of the Frankfurt plane, the philtrum (with the crossover point between the aforementioned branches) corresponds to the decussation of the pyramids of the medulla oblongata at the level of the second cervical vertebra (Fig. 5). Therefore, the only intersection between the lateral branches of one of the twelve meridians matches two of the three anatomical planes, sagittal and transverse, to the decussation of the pyramids (i.e., the only intersection macroscopically visible in that portion of the nervous system).
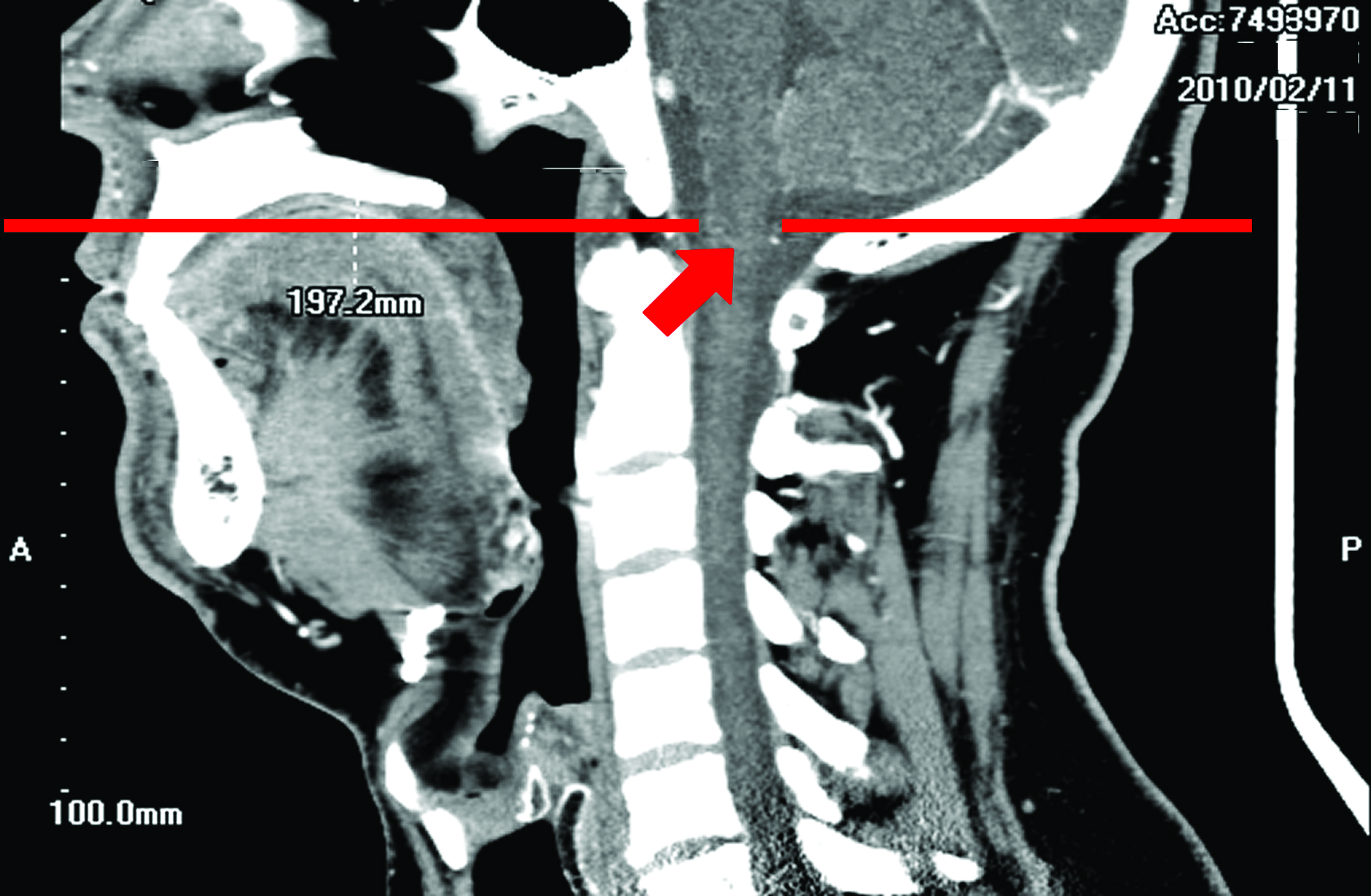
A magnetic resonance imaging lateral scan of the head. It shows the coincidence of the sagittal and transverse planes between the philtrum and the decussation of pyramids. Image courtesy of Giuseppe Sperandeo, MD, Radiology Unit, Casa Sollievo della Sofferenza, San Giovanni Rotondo (FG), Italy. Color images available online at www.liebertpub.com/acu
The Circle in the Kidney Meridian and the Shape of the Male Urogenital Apparatus
The morphological peculiarity of this alteration, unique in the many meters that make up the acupuncture meridian system, had long raised the following question: “Why is there a circle only in the Kidney meridian?” The teachers of traditional acupuncture either did not respond or responded dogmatically with: “Because that's what texts say.” The search for a rational, even if not definitive, explanation led the current author to compare pictures of the Kidney meridian, as indicated by An Outline of Chinese Acupuncture, 54 a chapter in Chinese Acupuncture and Moxibustion, 2 and Acupuncture, Meridian Theory and Acupuncture Points, 3 with pictures of the male and female urogenital anatomy, selected from works that were best adapted to an effective and schematic comparison (such as the book by Gray). 59
The current authors juxtaposition of the line forming the circle in the Kidney meridian (Fig. 6A) with the male urogenital apparatus in the sagittal section (Fig. 6B–D) revealed that the first identifiable circle is that of the spermatic path (Fig. 6B), which is composed of the vas deferens and the prostatic and penile urethra (heavy dotted line). The vas deferens begins in the epididymis, descends around the testis, proceeds straight upward, entering the inguinal canal and bypassing the pubic bone, then runs backward laterally to the bladder, past the medial insertion of the ureter into the bladder, meets the vas deferens of the opposite side and enters the prostate, where it forms the ejaculatory duct. Finally, it continues to the urethra and terminates at the urethral opening. An angle of no more than a few degrees is formed by the initial section of the vas deferens with the penile urethra when the penis is flaccid and opens by over 90° when the penis is erect (light dotted line).
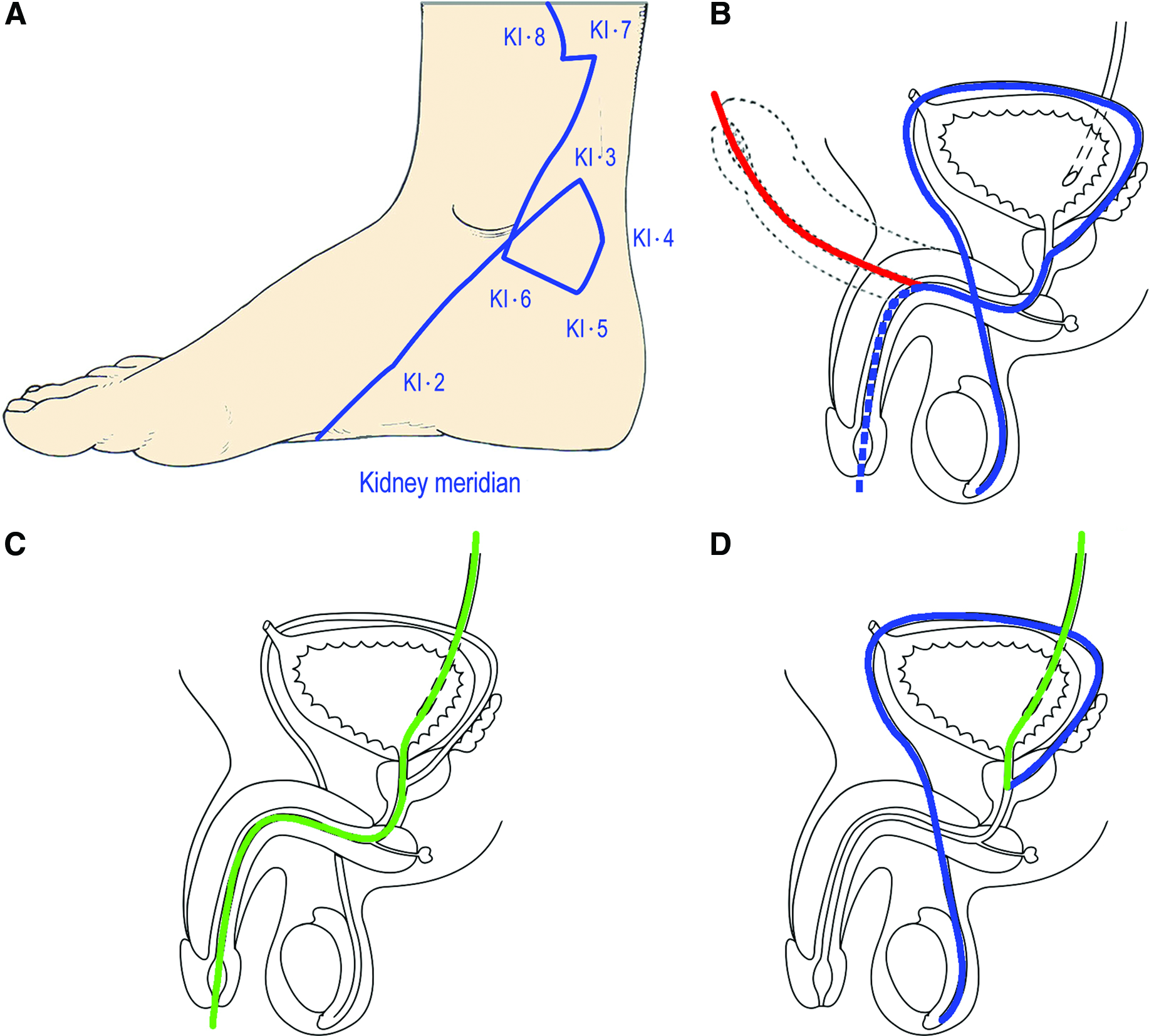
A second circle can be created artificially by combining the initial part of the spermatic path, from the testicle to the entrance to the common urethra, with a portion of the urinary path (Fig. 6C) and by drawing a line that runs against the tide of the vesicle urethra, enters the bladder, the ureteral opening, and proceeds upward along the ureter (Fig 6 D).
Although it is not as definite or as long as that of the spermatic path, a circular pattern can also be detected in the female genital apparatus in humans and other mammals (see below). It must be mentioned that the female genital apparatus is quite different from its male counterpart because it does not need to make use of the urinary path to move an unfertilized egg or unborn child from the ovary to the outside of the body, passing through the sites where menstruation and fecundation, development, and delivery occur, namely the Fallopian tubes, uterus, and vagina. In contrast, the sperm must flow through most of the urethra, which also serves as the urinary path.
Discussion
Preliminary Remarks
The need to obtain direct or indirect macroscopic evidence from acupuncture research pertains to the relationship between the meridians and their related internal organs, and the specific areas of the body from which they start or where they finish. On the contrary, it is easy to see how the meridians correspond to the gross anatomy of intermediate paths. For example, the Large Intestine meridian in the forearm is defined by the groove formed by the brachioradialis and the extensor carpi radialis longus and brevis muscles; and the Stomach meridian in the abdomen follows the intramuscular raphe of the rectus abdominis muscle. This meridian continues in the lower leg with the intramuscular groove which is found in the tibialis anterior muscle. The Lung meridian in the forearm could be represented by the radial artery and nerve, the Pericardium meridian by the median nerve and artery, and so on. It must be said that gross anatomy cannot explain some of the peculiar aspects of acupuncture therapeutics, such as the radiation of sensation along the meridian trajectory often caused by vigorously working the needle, possibly because it pertains to nerve physiology. Of course, gross anatomy provides proof of past or present existence, but not of existence as a whole.
Drawings of the Meridians as Motion Vectors
From a first analysis of the shapes of the drawn meridians, a novel idea led the current author to wonder if most changes in path direction could be the result of motion-vector representations of the limbs on which they are located. For example, the double reversal in direction in the meridian of the Stomach in the leg (Fig. 1) might be the vector of flexion–extension of the foot on the leg. This hypothesis is partially supported by the zigzag path of the Small Intestine meridian in close proximity to the shoulder joint (Fig. 2), which is the joint with the greatest range of motion). Similarly, the circle in the Kidney meridian on the foot underlines its likeness to a motion-vector representation. In fact, this circle is located between the foot and the leg in the anatomical region where the ankle behaves as a second-class lever for the actuation of extensions of the lower limb during jumps and rebounds. The fulcrum of the lever is the tip of the foot that stands on the ground; power is derived from the contraction of the gastrocnemius muscle applied to the heel via the Achilles tendon; and resistance is derived from the weight of the body acting on the toes via the ankle joint. Thus, this circle shape can be seen as a torsion coil spring with a single loop. Modern prosthetic legs that lack any sort of circles, but whose mechanisms would act similarly to those that led the sprinter Oscar Pistorius to seek admission to competitions for athletes with natural limbs, have the point of greatest tension in the elastic curve “replacing” the heel and ankle.67,68 This hypothesis does not conflict with the following hypothesis; rather, they complement one another.
Drawings of the Meridians as Morphogenetic Paths
The results of the analysis of the drawn meridians of the Large Intestine and Kidney revealed a similarity between the path shapes of the acupuncture meridian system and those of the macroscopic anatomy of relevant organs, supporting the possibility, which has never been abandoned by the majority of researchers working in this field, that meridians are real, biophysical entities.
As described above, the only intersection between the right and left branches of a meridian matches two of the three anatomical planes, sagittal and transverse, with the only visible junction of the medulla oblongata. The shape that the same meridian assumes in the nasolabial region (Fig. 4A) strongly resembles the shapes described by the dynamics of the embryonic development of this region: The bud of the right colon, or cecum bud, which lies in the medial plane of the abdomen, rotates counterclockwise and bypasses the physiological invagination of the intestinal loop into the umbilical cord, reaches the right side and descends to the right iliac fossa, where together with the transverse and left colon, it stretches and grows (Fig. 7). The large intestine is the only abdominal organ that consists of two lateral portions, ascending (right) and descending (left) colon, connected by a cross portion, the transverse colon (Fig. 4B). It could be argued that the urinary tract has a similar composition because the right and left kidneys and ureters are connected by the bladder and urethra, which are located along the midline. However, unlike the kidney, bladder and urethra, the right, transverse and left colon constitute a morphological and functional continuum.
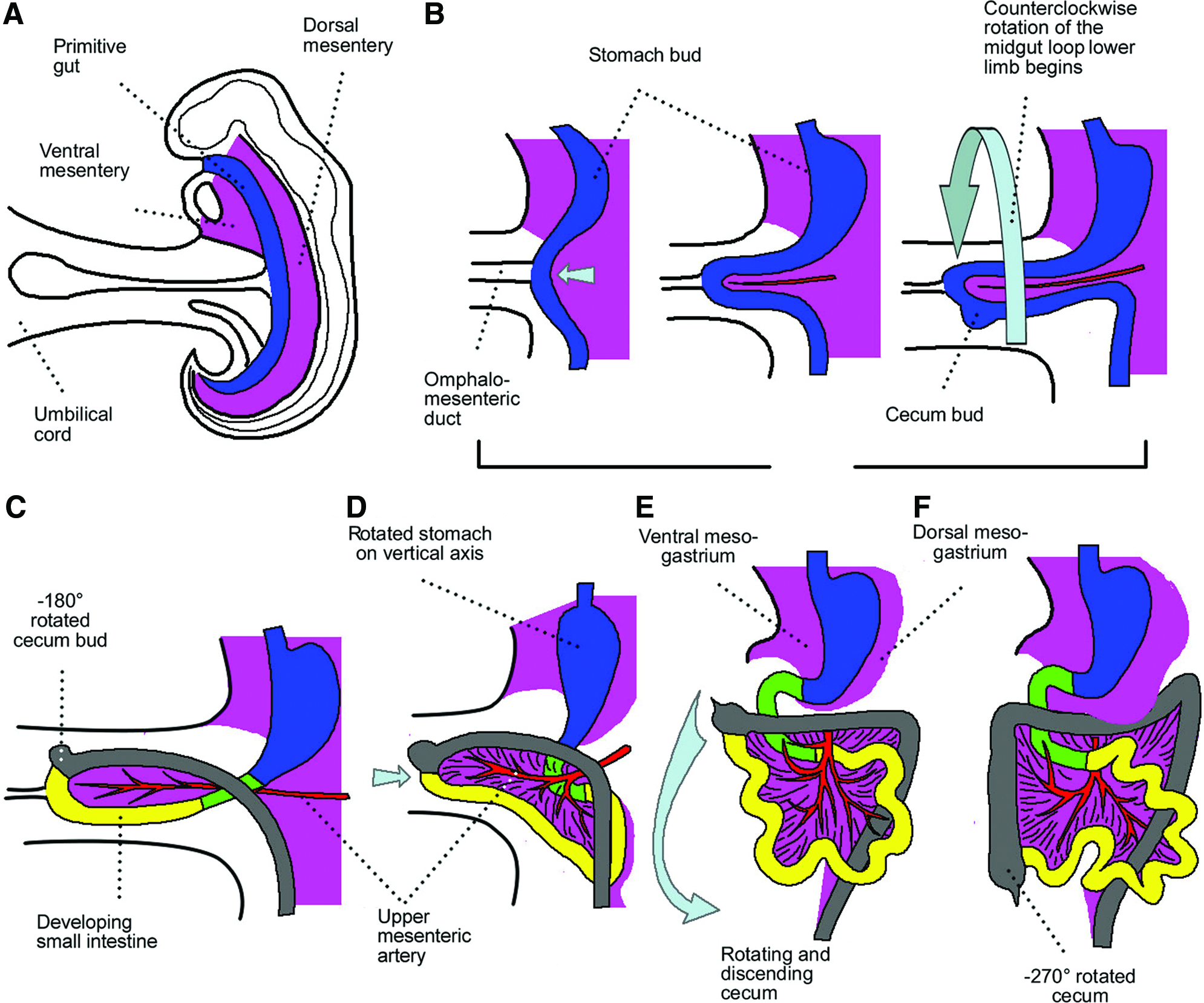
Human embryonic development of the large intestine. The cecum bud
The most original figure of the whole system of acupuncture meridians (i.e., the circle in the Kidney meridian; Fig. 3), corresponds very precisely to the circular spermatic path in humans and in terrestrial and aquatic mammals. As shown in Figure 7, concerning the intersection between the right and left branches of the Large Intestine meridian, this meridian similarly follows the forms of embryonic development. In the human embryo and neonate, because of their positions in utero, the area of the foot on which the circle in the Kidney meridian is drawn is very close to the external genitalia, namely the buds of the scrotum in males and the labia majora in females. In fact, between the 20th and 50th days of embryonic development, during which the primitive tail regresses (Fig. 8A), the knees form and fold, and the feet are defined and supinate (while the hands pronate). At this point, the knees are folded, so the heels and the medial aspect of the ankle directly face the labia majora and the scrotum, into which the testes will descend later (Fig. 8B).
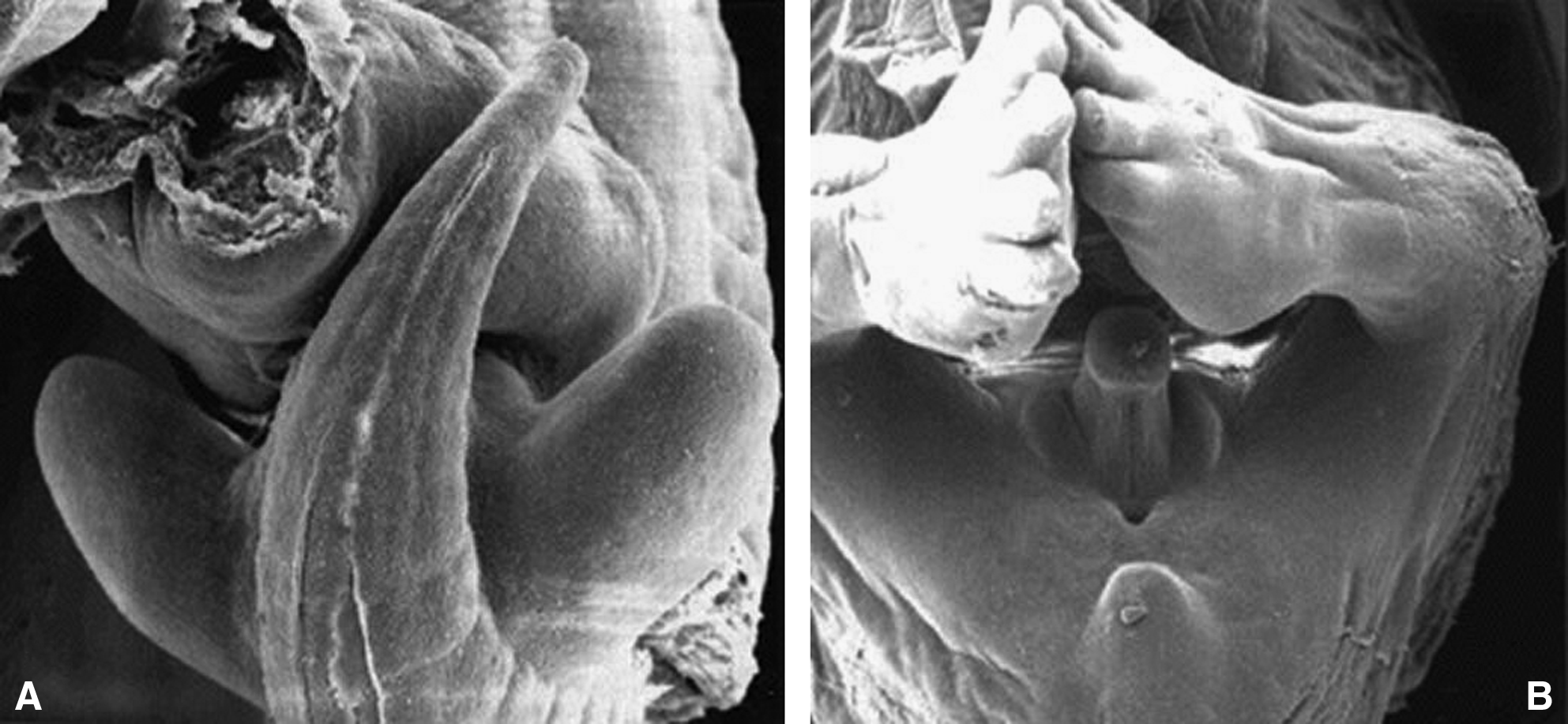
The forming external genitalia. They are not visible
The current author also looked at images of the anatomy of the urogenital apparatus of three mammals and a marine mammal: a male dog (Fig. 9); a cow and a bull; female and male goats; and male cetaceans (Fig. 10). With regard to the male genital morphology of cetaceans, Slijper wrote:
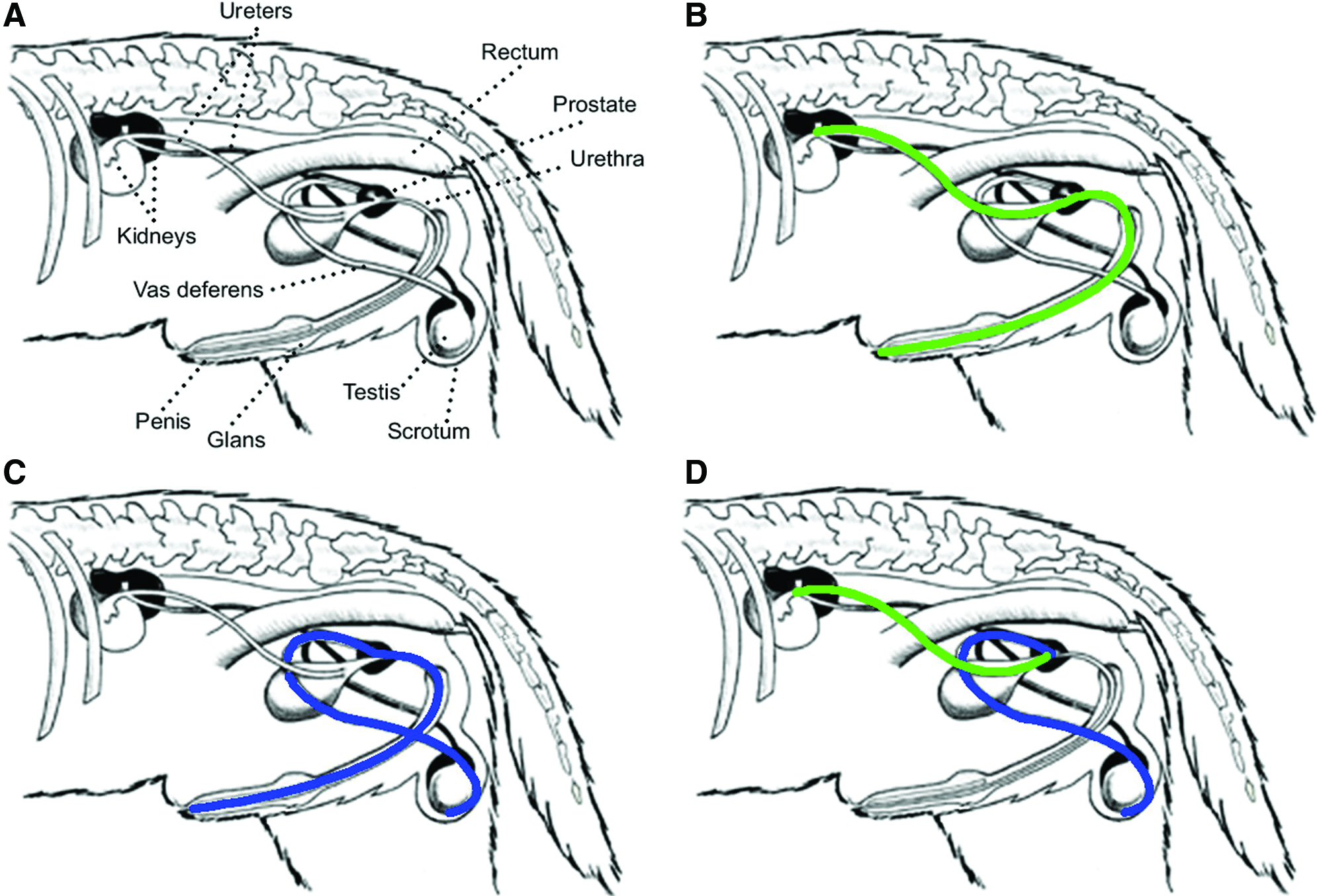
Male canine urogenital apparatus.
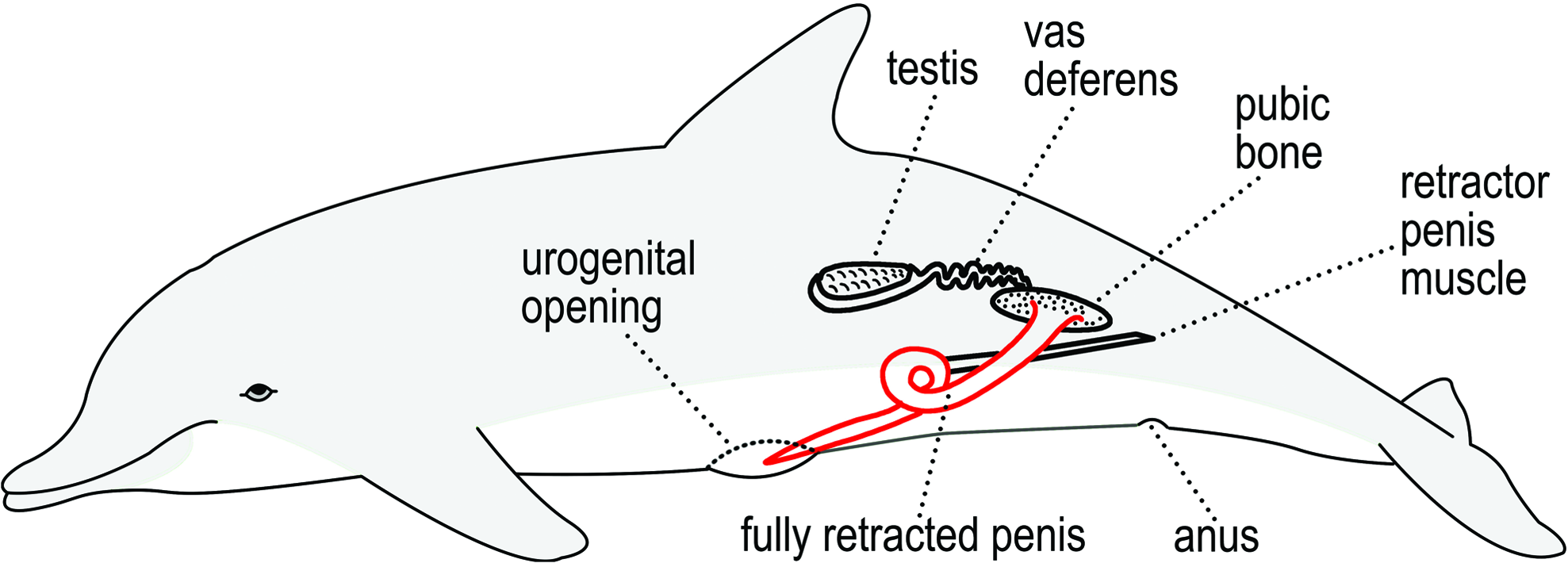
Position of the penis and surrounding anatomy in a cetacean. In the dolphin, the penis itself, rather than the spermatic path, is circle-shaped because the cetacean penis is a tendon and not a muscular structure. Color images available online at www.liebertpub.com/acu
Immediately caudal to the terminal cone, the retracted penis shows (depending on the stage of retraction) a curve, varying from an S-shaped loop to a curve of 360°, lying in the horizontal plane. Because in erection the thick, tough tunica albuginea of the penis permit only a little stretching by filling of the cavernous spaces with blood, this curve enables the animal to protrude the organ. 69
The juxtaposition of the image of the circle in the Kidney meridian with the images of the urogenital tract of these animals reveals features that are similar to those of humans. Furthermore, in female terrestrial mammals, because of their quadrupedal position, the circle of the ovarian path that partially overlaps with the circle in the Kidney meridian is more evident than in the human female.
It must be remembered that the feet of terrestrial mammals are anatomically different from human feet, and, in dolphins, one refers to fins rather than feet. The current author also recognizes that cetaceans are highly evolved, having descended from artiodactyls, so their inclusion here as a comparative group is not fully appropriate. In addition, in veterinary medicine, the meridian pathways of human acupuncture have been arbitrarily adjusted to the shapes and bodies of animals. In the absence of proof to the contrary, the ancient books of traditional medicine quoted by Bossut, 70 and Birch and Felt, 71 appear to indicate points of acupuncture for the treatment of many domestic animal diseases, although these sources do not mention or illustrate the meridians.
Because skepticism is an essential tool of scientific knowledge, the current author acknowledges the possibility that all of the similarities that were found are nothing but coincidences. However, there are at least two reasons to view these similarities as correlations. These reasons, which support the hypothesis that the acupuncture meridian system is a morphogenetic structure, though of an unknown type, are as follows:
(1) The four acupuncture points forming the circle of the Kidney meridian (points KI 3 to KI 6) and the two near ones (points KI 2 and KI 7) have traditionally been indicated to treat diseases of the urogenital tract. Although the Chinese tradition provides the same indications for points of other meridians, these others are points on the abdominal or dorsal skin, on which the symptoms depending on those organs are projected. In contrast, the points belonging to the Bladder meridian, which are situated on the lateral aspect of the foot and therefore are opposite the points forming the circle of the Kidney meridian, have no indications for genitourinary disorders (Fig. 3; Table 5). (2) The meridian system does not appear to be a random collection of lines. On the contrary, its organization is complex and significant. Each meridian consists of an internal organ, a paired organ, an area of the head and a particular zone of the hand and foot, and as a sensory organ. The circadian flow of Qi or vital energy in the circuit provided by the succession of all meridians is worthy of speculative and experimental attention.
Bolding indicates genitourinary disorders.
Although the investigation of the meridian system by means of morphological juxtaposition with the gross anatomy of the relevant organs is the current author's own original idea, there are some studies in the literature that both corroborate and are supported by the current author's observations.
Shang 72 hypothesises a relationship between acupuncture meridians and embryo morphogenesis. He suggests a role for the involvement of the meridian system in the regulation of growth, as follows:
Both organizing centers and acupuncture points have low electric resistance. The low electrical resistance is related to the distribution of gap junctions and thus intercellular communication. Some acupuncture points may be organizing centers. The meridian system is important in the coordination and regulation of morphogenesis. The properties of organizing and acupuncture points can be explained on the basis of the singular point. Coupling and oscillation may underlie the mechanism of acupuncture as well as growth regulation. 72
Li-Ling73–75 reported that complex genetic malformations be explained adequately by the theory of meridians, coupled organs, and the Five Elements. He stated: “By combining the theories of traditional Chinese medicine with modern medical knowledge we can infer the intrinsic mechanism of the various aspects of the phenotypic composition of the human individual, that is the phenomenal human being.” 74
Li-Ling and Wu, after studying congenital malformation syndromes that simultaneously affect the lung, the colon, and the skin, stated that the meridian system probably exists and, furthermore, added that “the theories of Chinese medicine can provide important explanations in the pathogenesis of major diseases, and directions for the development of a new treatment of lung-related diseases.” 76
Although Lee 77 specifically states that the meridian system is a neurophysiologic structure of the somatotopic type represented in the thalamus and other parts of the brain and not a gross anatomical entity, he incidentally provides another supportive argument for the current author's supposition that the meridians are an integral part of the genetic plan for embryological development and the maintenance of extrauterine health. In fact, Lee argues that:
the genetic information contained in the one-dimensional genome may be converted into a three-dimensional body plan for development. Prior to mitosis of the fertilized egg, the chromatids, after being unpackaged from the chromosomes, link up to form a giant circular loop which is then folded upon itself into a wired-frame structure that embodies the architectural embryological developmental scheme. 77
Yung 78 has developed an original model to explain the system of Qi and channels of acupuncture:
The concept of Qi and the concept of channel are so closely related that they must be defined and comprehended simultaneously in a coordinated fashion. Once the nature of Qi is established in terms of physics, we may be able to explain the functional role that the channels play, as well as explain other Chinese medical terminology with a language of modern science. Based on the low electrical impedance characteristics of acupoints, we propose that the meridian channel is equivalent to an electromagnetic transmission line and the Qi is the electromagnetic (EM) standing wave riding on the line, with acupoints as its nodes. 78
Abad-Alegria and Pomaran 79 demonstrate that points with traditional cardio-therapeutic activities, as described by TCM, have the same embryological origin as the heart (Fig. 11).
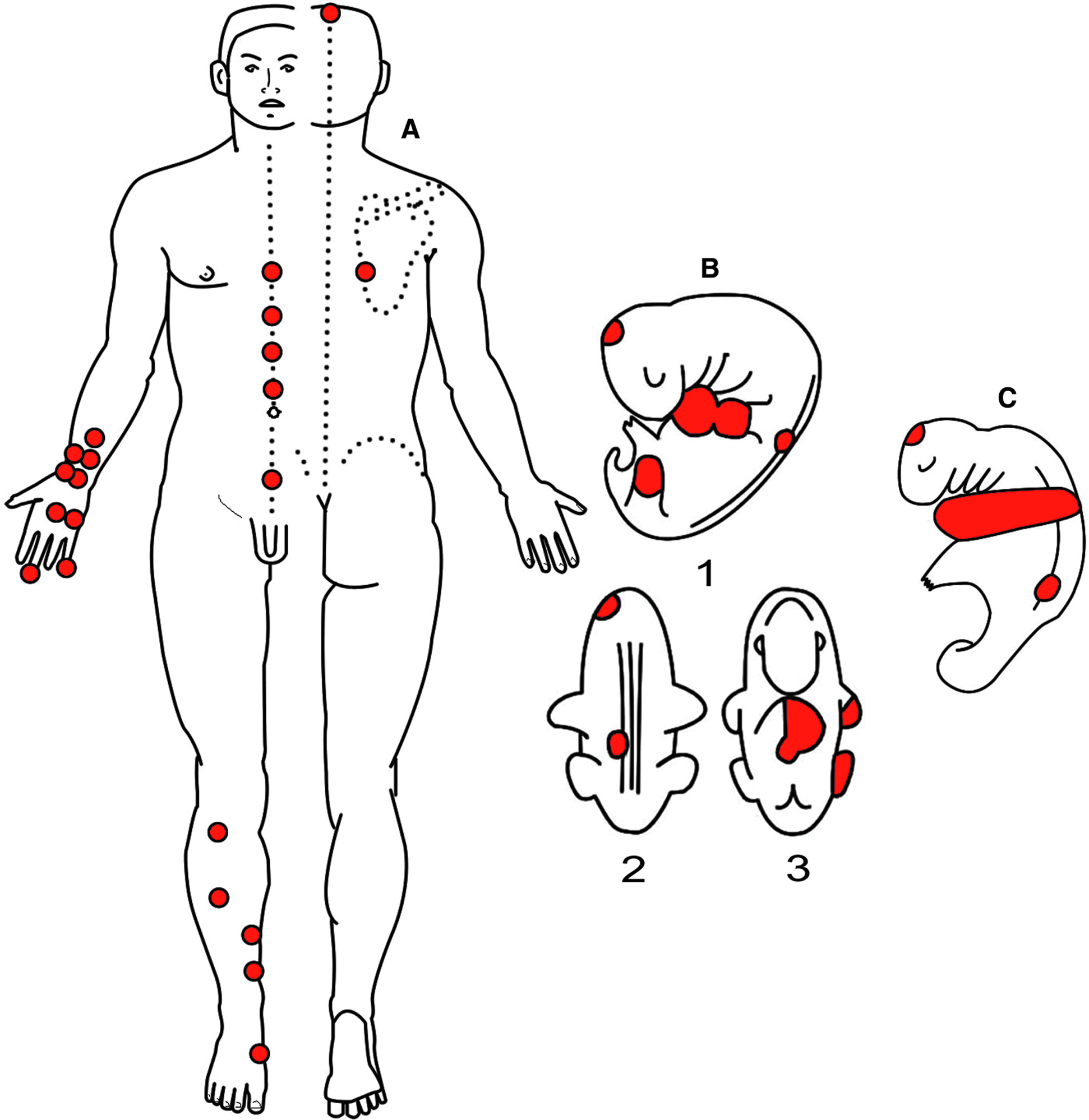
Acupuncture points with therapeutic effects on cardiovascular pathology in an adult
Finally, there is the previously mentioned work of Shin et al. 30 on the Bonghan system with the researchers' startling conclusion: “Furthermore, spherical granules of about one mm in diameter are detected in the subducts. These granules were well stained by using the Feulgen reaction, which implies that they contain DNA.”
As described above, a possible alternative explanation of the juxtaposition of the shapes of meridians with the shapes of organs is that they are vectors representing the movement of the limbs. With regard to this explanation, it must be noted that this comparison limited the extent of juxtaposition by examining only virtual images of the meridians over images of macroscopic organs; therefore, it is not a comparison between the meridian drawings and real human and animal bodies. Therefore, research on acupuncture must focus on demonstrating the existence of a biophysical relationship between the external paths of the meridians and the organs and portions of the limbs associated with them.
Conclusions
The debate on the physical existence of the meridian system is still current and the challenge for acupuncture to understand it and its benefits is likely to continue for some time because of the profound differences between Eastern and Western philosophies. If acupuncture meridians exist, the system they support could play a role in the morphogenesis of embryos and in the maintenance of the anatomical forms of the organs, with a long-term effect on adult health. According to Chinese tradition, the circulation of vital energy that occurs regularly in 2-hour cycles for each of the 12 main meridians from conception to death may affect, for example, the almost simultaneous morphogenesis of an organ (Kidney), its coupled organ (Bladder), a region of the head (root of the tongue and inner ear), and a portion of one limb (medial surface of the sole and little finger). Would it not be useful to embryologists, geneticists, and even to evolutionary and developmental biologists to investigate the possible existence of such a morphogenetic structure?
Footnotes
Acknowledgments
Thanks to Jamie Davies for giving the current author the opportunity to begin to write a scientific paper. For providing indispensable pictures the current author thanks Bradley R. Smith, PhD (The Multidimensional Human Embryo, http://embryo.soad.umich.edu/), Kathleen K. Sulik, PhD (MouseWorks, Inc., www.mouseworks.com), Edda H. Geirsdottir of Ossür (www.ossur.com), Race Foster, DVM, and Marty Smith, DVM (![]() ). For their support the author also thanks his colleagues Im Quah-Smith, MD, Francisco J. Abad-Alegría, MD, Gabriele Saudelli, MD, Marco Visconti, MD, Mohammad Natour, MD, Giuseppe Sperandeo, MD, Luca Arru, MD, and Angelo Mottola, MD, of Relative Truths Labs.
). For their support the author also thanks his colleagues Im Quah-Smith, MD, Francisco J. Abad-Alegría, MD, Gabriele Saudelli, MD, Marco Visconti, MD, Mohammad Natour, MD, Giuseppe Sperandeo, MD, Luca Arru, MD, and Angelo Mottola, MD, of Relative Truths Labs.
Disclosure Statement
No financial conflicts exist.
*
Cited by Hsu. 7