
Abstract
Abstract
Objective:
Patients with chronic disorders of consciousness (DOC) frequently develop chronic constipation. This study evaluated the effects of acupuncture on bowel movements (BMs) in patients with DOC and chronic constipation resulting from severe traumatic brain injury (TBI).
Materials and Methods:
This retrospective observational study took place in the Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, of Kizawa Memorial Hospital, in Minokamo, Gifu, Japan. The study included 25 patients with chronic DOC resulting from TBI, who received acupuncture treatment. The patients received 2 sessions of acupuncture treatment per week. Information on frequency of defecation, number of days during which patients had BMs, and use of laxatives prior to the acupuncture treatment and after 10 weeks of treatment was extracted from medical records and compared.
Results:
The median (first quartile and third quartile) frequency of defecation increased significantly after 10 weeks of acupuncture from 3.0 (2.5, 3.5) to 3.5 (2.5, 4.5) times/week (P = 0.038). The number of days on which defecation occurred also increased significantly, from 2.0 (2.0, 2.5) to 2.5 (2.0, 3.5) days/week (P < 0.001). The use of bisacodyl suppositories decreased significantly from 1.5 (1.5, 2.0) to 1.5 (0.5, 2.0) times/week (P = 0.041). The mean ± standard error use of sodium picosulfate for 10 patients decreased significantly, from 20.4 ± 3.5 to 14.3 ± 3.3 drops/week (P = 0.004).
Conclusions:
Acupuncture treatment could be beneficial for chronic constipation in patients with DOC caused by TBI. A large prospective cohort study with a control group is warranted.
Introduction
Patients with neurologic diseases or injuries affecting the central nervous system (CNS) often develop bowel dysfunction, including chronic constipation and fecal incontinence. 1 Delayed colon transit times have been reported in brain-injured patients with constipation. 2 The severity of constipation has been reported to increase with greater disability poststroke in patients. 3 Patients with chronic disorders of consciousness (DOC) resulting from severe traumatic brain injury (TBI) can experience prolonged immobilization and bedrest; this can lead to chronic constipation, because physical inactivity plays a role in the etiology of functional constipation. 4 Pharmacologic agents, such as stimulants or lubricant laxatives, can relieve the constipation for these patients, but can induce abdominal pain, bloating, watery stools, and fecal incontinence. In addition, long-term use of stimulant laxatives can result in adverse effects, such as melanosis coli and cathartic colon.5,6 A nonpharmacologic approach to constipation is needed for this patient population.
Acupuncture has been reported to be effective for treating chronic constipation.7–9 In the current authors' previous clinical experience, occasional bowel movements (BMs) or flatus were noted in patients with chronic DOC who received acupuncture treatment during and after the treatment. This occurred even when the treatment was not administered for constipation but rather for brain activation and for relieving spastic muscle overactivity. However, to the best of the current authors' knowledge, there have been no reports investigating the effects of acupuncture on constipation in patients with DOC. The aim of this retrospective study was to evaluate the effects of acupuncture treatment on BMs in patients with DOC resulting from severe TBI.
Materials and Methods
Design, Setting, and Ethics
This retrospective observational study was based on a comparison of medical chart data before and after a period of acupuncture treatments. The study was conducted at a specialized institution for treating and rehabilitating patients with DOC following severe TBI due to motor vehicle accidents, the Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, of Kizawa Memorial Hospital, in Minokamo, Japan. The study was approved by the ethics committee of Kizawa Memorial Hospital (approval number: 29026) and was conducted in accordance with the principles of the Declaration of Helsinki.
Patients
The study included 28 patients with chronic DOC who received acupuncture treatment during a study period between April 2008 and December 2014. Of these 28 patients, 1 patient was excluded whose laxatives were changed within 1 month before initiation of the study acupuncture treatments, 1 patient who experienced daily BMs, and 1 patient who experienced bloody stools suggesting the existence of nonfunctional colon disease. Thus, the study included data for 25 patients (mean age: 35 years; median duration since injury: 19 months) with chronic DOC resulting from severe TBI. These patients' characteristics are shown in Table 1. All of the patients in the study had been brain-injured in motor-vehicle accidents.
Patients' Characteristics
Note: Data are presented as the number of cases, the mean ± standard deviation, or the median (first quartile, third quartile).
yrs, years; DOC, disorders of consciousness; VS, vegetative state; UWS, unresponsive wakefulness syndrome; MCS, minimally conscious state; DAI, diffused axon injury; tSAH, traumatic subarachnoid hemorrhage; ICH, intracerebral hemorrhage; mos, months; CNS, central nervous system.
The DOC state of 12 patients was a vegetative state (VS; recently known as unresponsive wakeful syndrome); the DOC state of the other 13 patients was a minimally conscious state (MCS). VS is characterized by spontaneous arousal and sleep–wake cycles but with no evidence of self or environmental awareness; no interactions with other people; and no sustained, reproducible, purposeful, or voluntary behavioral responses to sensory stimuli. 10 MCS is a condition of severely altered consciousness characterized by inconsistent but clearly discernible behavioral evidence of consciousness. It can be distinguished from coma and VS by documenting the presence of specific behavioral features. 11
Furthermore, subcategorizations of MCS into MCS-plus and MCS-minus based on levels of complexity of observed behavioral responses have been proposed. 12 MCS-plus is characterized by the presence of high-level behavioral responses, such as command following, intelligible verbalizations, or nonfunctional communications. In contrast, MCS-minus is characterized by the presence of low-level behavioral responses, such as visual pursuit; localization of noxious stimulation; or contingent behaviors, including appropriate smiling or crying in response to emotional stimuli. In the current study, 9 patents were classified as MCS-minus and 4 patients were classified as MCS-plus.
All patients received polymeric enteral nutrition through nasogastric or gastrostomy tubes 3 times per day. Furthermore, all patients required adult diapers for BMs; their median (first quartile, third quartile) frequency of defecation was 3.0 (2.5, 3.5) times/week; and the number of days during which defecation occurred was 2.0 (2.0, 2.5) days/week.
All patients needed laxative medications, which were administered according to each patient's condition to achieve a BM at least once every 3 or 4 days on average to avoid abdominal distention or increase of the patient's systemic abnormal muscle overactivity due to straining prior to defecation, and to avoid watery diarrhea. Patients were given 10-mg bisacodyl suppositories to be used when there were no BMs for 3 or 4 consecutive days; 10 patients also received sodium picosulfate liquid, administered on 2.1 ± 1.0 days/week, 9 patients were given magnesium oxide, and 7 patients received pantethine. Additionally, 7 patients were given probiotics, including Bifidobacterium spp. (n = 6; 41 ± 14 mg/day) and Clostridium butyricum (n = 1; 120 mg/day).
The above medications and medications for the CNS (Table 1)—including anticonvulsant agents, antispastic agents, and antiparkinson agents (dopamine agonists)—were continued at the same doses for at least 2 months prior to the commencement of acupuncture treatment.
The patients' nutrition and water intakes were also continued at the same levels for at least 2 months prior to commencement of the acupuncture treatment. All patients received physical rehabilitation, including range-of-motion exercises and sitting training, from the time of hospitalization at the medical center.
Acupuncture Treatment
Acupuncture treatment was performed twice per week for 4 months, except on public holidays, by an experienced acupuncturist who had a bachelor's degree and a master's degree in acupuncture and who was involved in clinical practice for more than 7 years. The treatment was given to ameliorate each patient's DOC and to address spastic muscle hyperactivity. In this clinical situation, the acupuncture protocol was not strictly standardized as would be in a prospective randomized controlled trial (RCT). Acupuncture treatment was performed based on previous reports,13–16 Traditional Chinese Medicine (TCM) theory, and the current authors' previous clinical experiences. 17 At the start of the treatment, a small-stimulation dose of acupuncture was attempted, because the safety and methods of acupuncture treatment for chronic DOC are not yet established in Japan. The stimulation dose of acupuncture, including needle retention time and manipulation, as well as number of acupoints used, were gradually increased over several weeks while confirming the absence of adverse events.
Acupuncture was initially performed at bilateral LI 4 and ST 36, GV 26, and Ex-HN 3, with GV 20, GV 23, PC 6, KI 3, GB 20, and LR 3 added after a few weeks. These acupoints were used in previous studies of acupuncture for DOC and spastic hypertonia.13–16 ST 36, LI 4, GV 26, and Ex-HN 3 have been reported to increase the excitability of the corticospinal system 14 and reduce spinal motor-neuron activity 15 ; these points were used for activating the brain, increasing motor responses, and reducing spastic muscle overactivity. LR 3 was added for patients with severe spastic muscle overactivity because LR 3 is on the Liver meridian and can be used to tonify muscles and tendons, according to TCM theory. ST 36 has often been used in acupuncture studies on constipation 9 and had induced increased colon motility and transit in an animal study. 18 LI 4 has also been reported to be effective for treating constipation. 7 Acupuncture points were also selected based on the posture of the patients, avoiding regions with operative scars and the absence of skull bone. The locations of the acupuncture points were according to the World Health Organization's standard textbook. 19
A Japanese-style gentle-needle technique, using acupuncture needle-guide tubes, was used to insert the acupuncture needles. Disposable sterilized stainless-steel acupuncture needles (0.16–0.20 mm in diameter and 40 mm in length) were inserted to a depth of 4–20 mm, depending on the thickness of each patient's skin and subcutaneous fatty tissue. If a voluntary movement of a limb or the neck was observed during the acupuncture treatment, the needles at acupoints in that area were removed for safety. Initially, the needles were left in place for 10 minutes with no manipulation, and the duration was gradually increased over several weeks to 40 minutes. After approximately 1 month of acupuncture, the needles at some acupoints, including LI 4 and ST 36, were manipulated for 1 minute about every 10 minutes, including rotating and/or sparrow pecking. All patients received acupuncture in their own beds in the inpatient ward.
Outcome Measures
For each patient, the frequency of defecation, the number of days per week on which defecation occurred at least once, and the doses of laxative medications administered were extracted from medical records for the period before acupuncture treatment and after 10 weeks of treatment. This period was decided in accordance with that of a previous study of acupuncture for constipation. 7 For each case, the average over a 2 week period was calculated. The frequency of defecation was recorded by ward nurses upon observing stool in each patient's diaper.
Statistical Analysis
The Shapiro–Wilk test was used to assess the normality of distributions. Normally distributed variables are summarized as mean ± standard deviations (SDs) or standard errors (SEs), and those without a normal distribution as medians (first quartile, third quartile). Comparisons before and after the treatment were evaluated using paired t-tests for normally distributed data or a Wilcoxon signed-rank test when the data were not normally distributed. P-values <0.05 were considered to be statistically significant.
Results
The median (first quartile, third quartile) frequency of defecation increased significantly after 10 weeks of acupuncture from 3.0 (2.5, 3.5) to 3.5 (2.5, 4.5) times/week (P = 0.038; Fig. 1A), as did the number of days on which defecation occurred, from 2.0 (2.0, 2.5) to 2.5 (2.0, 3.5) times/day (P < 0.001; Fig. 1B).
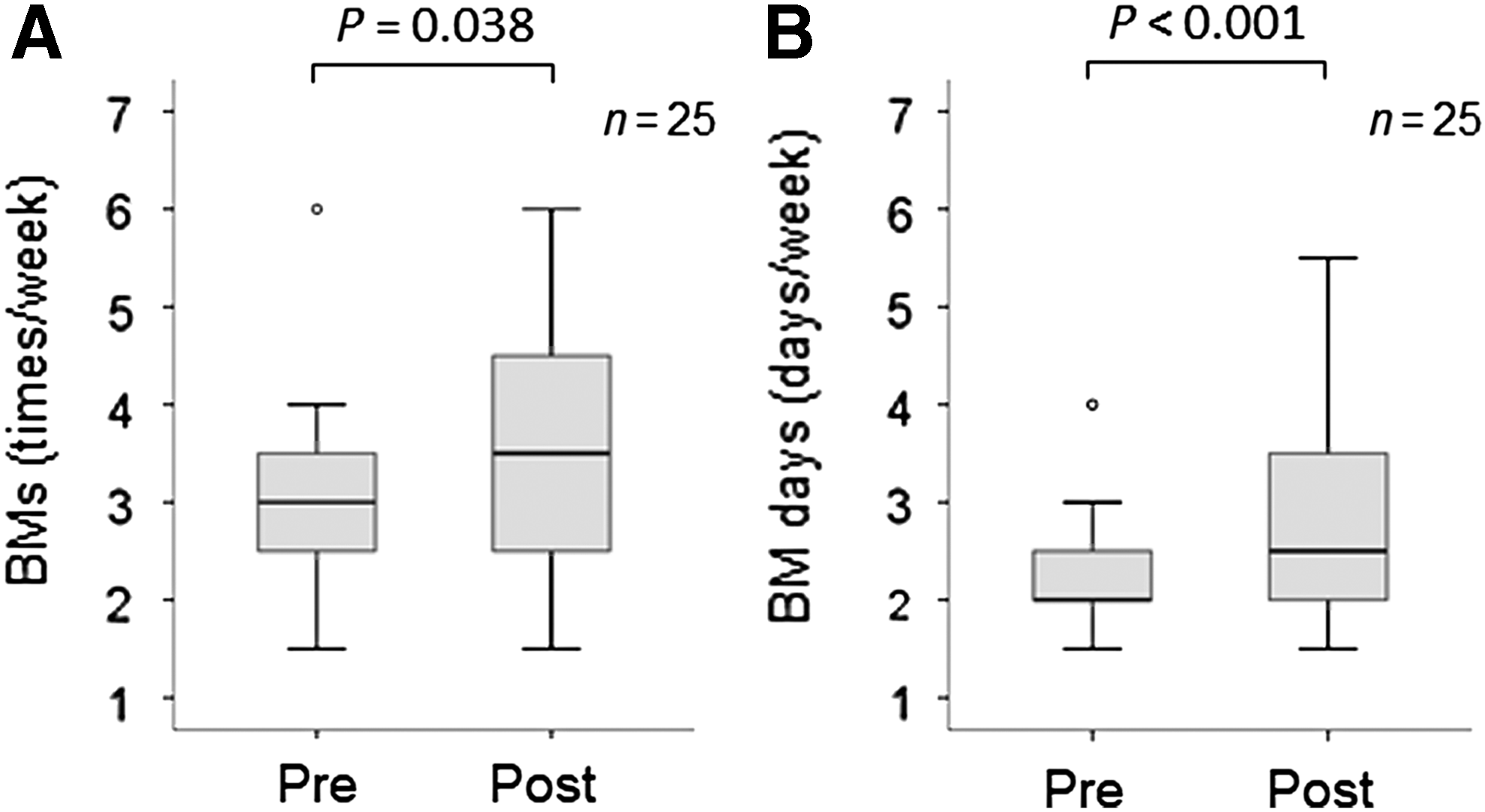
Changes in bowel movement (BM) frequency before and after 10 weeks of acupuncture treatment.
The median use of bisacodyl suppositories decreased significantly, from 1.5 (1.5, 2.0) to 1.5 (0.5, 2.0) times/week (P = 0.041; Fig. 2A), as did the mean (± SE) use of picosulfate in 10 patients, from 20.4 ± 3.5 to 14.3 ± 3.3 drops/week (P = 0.004; 1 drop is approximately 0.067 mL; Fig. 2B). There were also nonsignificant decreases in the use of magnesium oxide (from 953.3 ± 128.3 mg/day to 806.7 ± 156.4 mg/day; P = 0.104; Fig. 2C) and pantethine (from 328.6 ± 36.0 mg/day to 285.7 ± 50.8 mg/day; P = 0.200; Fig. 2D). Other medications—including CNS medications, rehabilitation, and nutrition and water intakes—were maintained at the same levels throughout the study period.
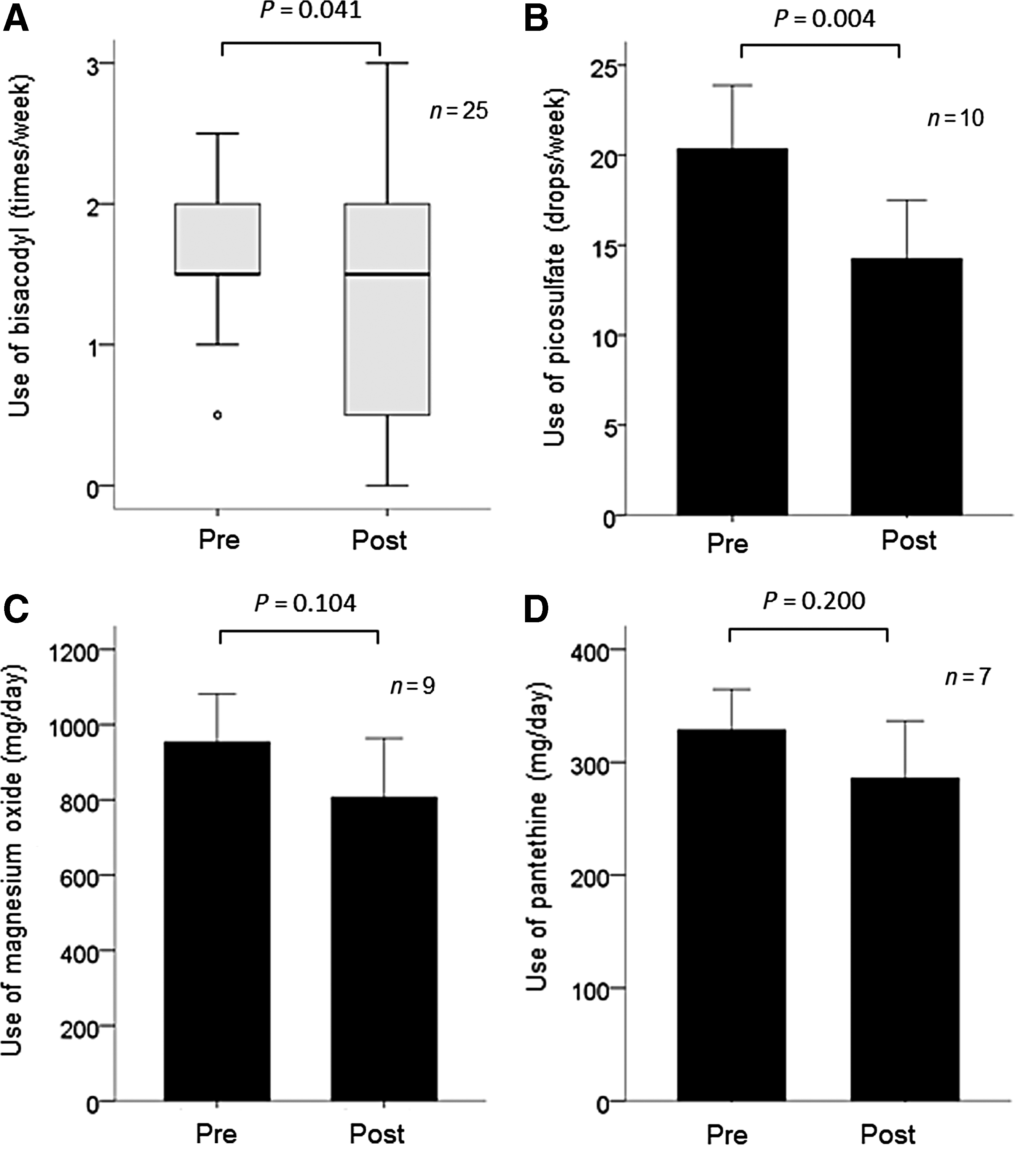
Changes in the use of laxatives before and after 10 weeks of acupuncture treatment.
Each patient received 21.4 ± 1.5 sessions of acupuncture treatment during 12 weeks of the study period. ST 36, LI 4, GV 26, Ex-HN 3, and KI 3 were used for all patients. In addition, GV 20 were used for 12 patients; PC 6 was used for 13 patients; GB 20 was used for 15 patients; LR 3 was used for 17 patients; and GV 23 was used for 4 patients. The number of acupuncture needles used in a session was 13 ± 2 (mean ± SD). No adverse events requiring medical treatment resulted from the acupuncture treatment.
Discussion
To the best of the current authors' knowledge, this is the first report to demonstrate the effects of acupuncture treatment on BMs in patients with chronic DOC resulting from severe TBI and chronic constipation. After 10 weeks of acupuncture treatment, the patients showed increases in frequency of defecation and number of days during which defecation occurred at least once. In addition, use of some medications for constipation was reduced. These findings suggest that acupuncture alleviated the chronic constipation although it was not always administered for that purpose. Acupuncture treatment may therefore be beneficial for chronic constipation in patients with DOC, and a prospective cohort study to elucidate the efficacy of acupuncture treatment for constipation as a primary endpoint in patients with DOC is warranted.
Delayed colon transit time has been reported in brain-injured patients with constipation, 2 and acupuncture increased colon motility and transit in an animal study. 18 The ST 36 acupoint—used in previous studies to increase colonic motility and relieve constipation14,18,9—was used for all patients in the present study. The current authors, therefore, speculate that colon transit might have been improved by acupuncture in these patients, leading to increased BMs; however, colon motility was not evaluated in this study. Further research is needed to elucidate the effects and underlying mechanisms of acupuncture on colon motility in patients with DOC and constipation.
There was a significant decrease in use of some laxatives after acupuncture treatment in this study. Thus, the use of acupuncture might reduce the risk of adverse events reported to result from the long-term use of stimulant laxatives.5,6
This preliminary study had some limitations. It was a retrospective case series. There was no comparative control group without acupuncture, no follow-up observation, and no blinded assessor. There were also several risks related to bias. The acupuncture points used were not always specific for constipation. Using additional acupoints reported to have beneficial effects for constipation8,9 could lead to more effective results. The types of laxatives used were not standardized, except for bisacodyl suppositories, because most of these laxatives were continuously prescribed by the hospitals where the patients were originally admitted before admission to the current authors' hospital. The criterion for medication tapering was also not standardized, as would occur in a prospective RCT. Different effects of acupuncture might have been observed because different medication regimens were used.
Stool forms and volumes were not investigated, because uniform records were not available. Subjective outcomes (straining, incomplete evacuation, and anorectal obstruction)—which are important when evaluating constipation—were not used as outcomes in the present study because it was not possible to evaluate these phenomena, given that patients' had DOC. The relatively small sample size and long observation period also could reduce the soundness of the study's findings because of the increased variability of multiple factors. Further prospective, large cohort studies with control groups and designed to relieve constipation as the main outcomes are needed.
Conclusions
Increased frequency BMs were noted after 10 weeks of acupuncture treatment in patients with chronic constipation and chronic DOC as a result of severe TBI. Acupuncture treatment could be beneficial for chronic constipation in this patient population. Further large prospective cohort studies with control groups are warranted.
Footnotes
Acknowledgments
The authors thank all the staff members of the Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, of Kizawa Memorial Hospital, and the participants in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.