
Abstract
Objective:
Myopia prevalence mostly affects young people, particularly in Asia. Of the several recommendations addressing the myopia epidemic, auricular acupoint stimulation (AAS) has been proposed and investigated. However, reported outcomes have been inconsistent, prompting a meta-analysis to obtain more precise estimates.
Materials and Methods:
Twelve articles were included in a meta-analysis, wherein each article was evaluated for risk of bias. Summary effects were calculated using odds ratios (ORs) and 95% confidence intervals (CIs). Outlier and sensitivity treatments as well as publication bias assessment were applied.
Results:
Risk of bias among the articles was low in random sequence but generally unclear judgments for the other bias criteria. AAS outcomes were significant (Pa [P-value for association] <0.00001–0.003) when random and fixed effects favored the treated groups (ORs: 2.87–3.42; 95% CIs: 1.44–5.75).
Conclusions:
This meta-analysis showed evidence of AAS being effective for controlling myopia. Substantial magnitude (up to 3.4-fold), robustness, and lack of bias strengthened this effect.
Introduction
Myopia is a refractive defect of the human eye, which, on the measurement scale, is identified as −0.50 diopter. This ocular defect especially occurs in the Asian juvenile population.1,2 High myopia is measured at ≥ −6.0 diopter, which is not only a refractive problem3 but one that can lead to serious eye problems, such as macular degeneration, retinal detachment, glaucoma, and cataracts. 4 This eye disorder has become a serious global public health issue wherein myopia prevalence among young adults in Western countries (United States, European countries) is 4 times lower than in East Asia (Taiwan, Hong Kong, and Singapore; 20% versus 80%).5–9 Delaying myopic progression involves several therapeutic approaches that include cycloplegics, ocular hypotensives, contact lenses, bifocals and multifocals, and eye drops (atropine).10–12
In terms of Traditional Chinese Medicine (TCM), auriculotherapy as an alternative medical modality has been used extensively for preventing, reducing, and treating myopia.13,14 As a complementary therapeutic approach, auricular acupoint stimulation (AAS) is defined as “a health care approach wherein the external surface of the ear or auricle, is stimulated to alleviate pathological conditions in other parts of the body.” 15 Previous studies have shown that visual acuity in patients with myopia was significantly improved after AAS treatment,16,17 although the outcomes were reported only for low-grade myopia (<−3.0 diopter).16–18 Since then, more studies have been published in both the Chinese and English languages. Therefore, this study investigated the primary data regarding the effect of AAS intervention on myopia, using a meta-analysis, to clarify the effectiveness of AAS for preventing or retarding the progression of myopia.
Materials and Methods
Selection of Studies
MEDLINE,® was searched, using PubMed, Google Scholar, China National Knowledge Infrastructure (CNKI), and Wanfang databases for association studies as of May 15, 2020 (Table S1). The terms used were
Data Extraction
Two investigators (P.S. and N.P.) independently extracted data; disagreements were adjudicated by a third investigator (P.T.), resulting in a consensus. The following information was obtained from each publication: if the study was included in the previous meta-analysis 19 ; first author's name, language; intervention; control treatment; outcome measures; ages; frequencies/durations of treatment; and sample sizes of cases and controls (Table 1).
Characteristics of the Included Studies
Inclusion of the article in the previous meta-analysis by Zhang 201319 is indicated by ✓; otherwise ○.
Quantitative expressions of age in yrs were mean ± standard deviation, range, or school level.
Grade 5, ages ∼10–11.
K, no of article; C, Chinese; E, English; yr(s), year(s); d, day(s); wks, weeks; mos, months.
Study Quality and Risk of Bias
Risk of bias was assessed based on the Cochrane handbook 20 guideline, which was applied to randomized controlled trials and studies that involved interventions. 21 This assessment tool is used to address biases originating from sequence generation (selection bias), allocation-sequence concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), and selective outcome reporting (reporting bias). Responses to each item was either yes, no, or unclear. More yes responses indicated a low risk of bias; otherwise, risk of bias was considered to be high. Insufficient descriptions merited “unclear” judgments. Judgments were assigned by two of the authors (N.P. and P.T.) working independently, and discrepancies were remedied through discussions with a third investigator (P.S.) to obtain a consensus.
The Meta-Analysis
Given the hypothesis that AAS lowers the risk and delays the progression of myopia, the ORs were estimated for each study and calculated pooled ORs with 95% CIs. ORs > 1.0 favored AAS treatment; otherwise, controls were favored (ORs < 1.0). Operating data was dichotomous for AAS, wherein treatment and control numbers were used. Heterogeneity between studies was estimated with a χ 2 -based Q-test, 22 with a threshold of significance set at Pb [P-value for heterogeneity] <0.10. Strength of evidence was more versus less, based on the following features: (1) Pa [P-value for association] values with more decimals had greater associative significance than those with fewer decimals; (2) OR values further from the null effect (OR = 1.00) had greater magnitude than those that were not 23 ; (3) lower CI difference (CID) values were more precise than high CID values; and (4) low-level heterogeneity (Pb > 0.10) or homogeneity (I 2 = 0%) were more favored than heterogeneous (Pb < 0.10) outcomes. Heterogeneity was quantified with the I2 statistic, which measures variability between studies. 24 I2 values of >50% indicate more variability, compared to ≤50%, with 0% indicating 0 heterogeneity (homogeneity).
Evidence of functional similarities in population features of the studies warranted using a fixed-effects model 25 ; otherwise a random-effects model 26 was used. Sources of heterogeneity (outliers) were detected with a Galbraith plot 27 followed by reanalysis (without the outliers) that dichotomized the comparisons into pre-outlier and post-outlier categories. Sensitivity analysis—which involves omitting one study at a time and recalculating the pooled OR—was used to test for robustness of the summary effects. Publication bias for comparisons was assessed using an Egger's regression test. 28 Except for heterogeneity estimation, 22 2-sided P-values of <0.05 were considered significant. Data for the meta-analysis were analyzed using Review Manager 5.3 (Cochrane Collaboration, Oxford, England), SIGMASTAT 2.03, and SIGMAPLOT 11.0 (Systat Software, San Jose, CA).
RESULTS
Search Results and Study Features
Figure 1 outlines the study selection process in a PRISMA [Preferred Reporting Items for Systematic Reviews and Meta-Analyses]–sanctioned flowchart. A detailed description of this meta-analysis is summarized in the checklists for PRISMA (Table S2). The initial search of the 4 databases using 5 search strings yielded 16,459 citations (Table S1), followed by a series of omissions (Fig. 1) that resulted in 12 articles for inclusion.29–40 Table 1 shows that the majority of the included articles were in Chinese, and 3 articles were in English.29,35,37 Subjects in all the included articles were Chinese (Asian) with a centennial demographic profile (born around the turn of the twentieth century and after) (Table 1). All interventions involved auricular acupuncture, with some studies using modifications, such as laser irradiation, 30 plasters (bandages),35,40 and interactive multimedia. 37 Control treatments in most of the studies involved eye drops, with 2 studies using abdominal acupuncture 31 and correct posture. 38 A homogeneous aspect of this meta-analysis was the outcome measure, which was visual acuity in all component studies. Treatment frequencies and durations in cases ranged from once to 6 times per day and 1–6 months, respectively.
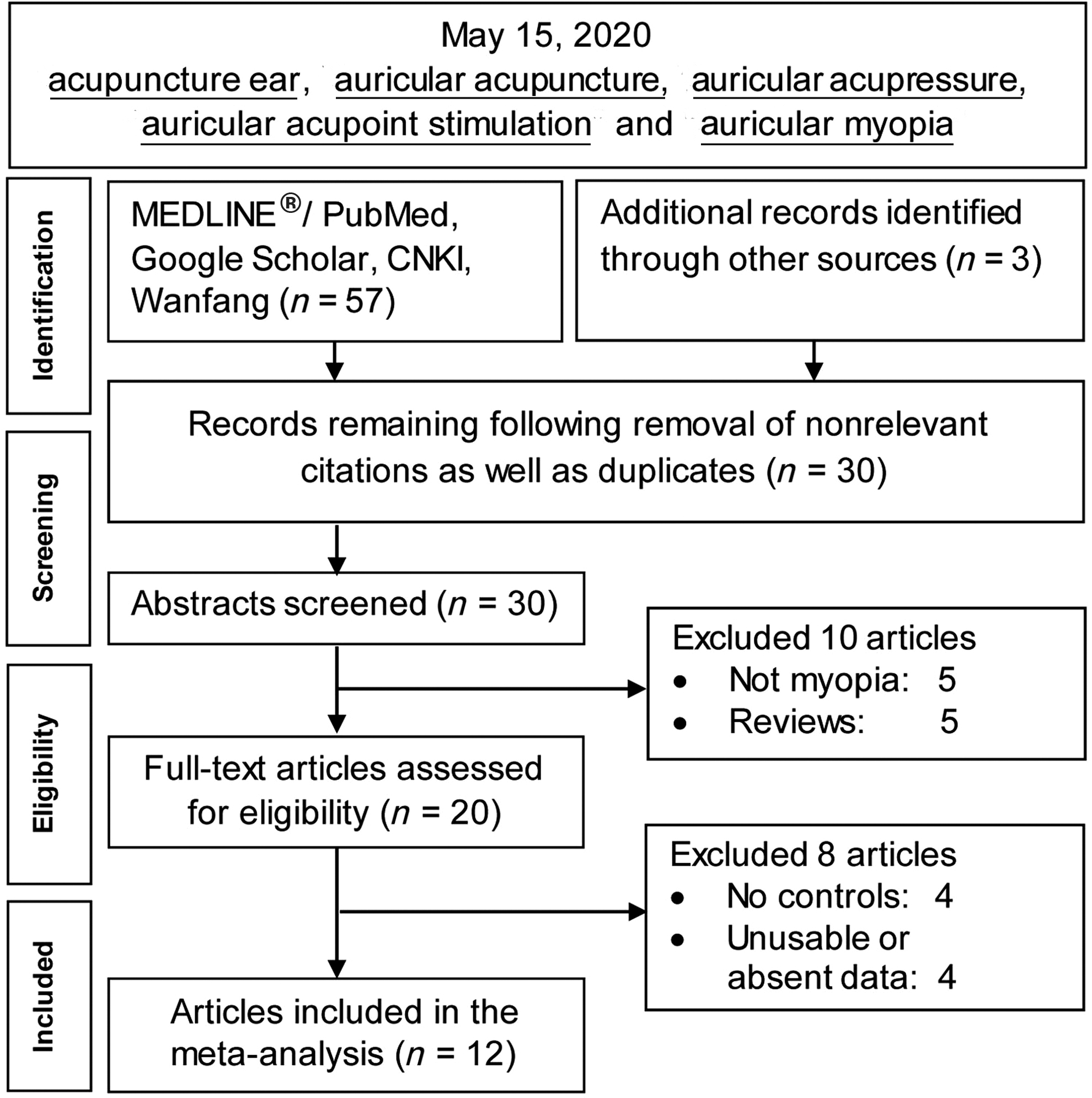
Summary flowchart of literature search. CNKI, China National Knowledge Infrastructure.
Study Quality and Risk of Bias
Indication of methodological quality was expressed in the risk-of-bias assessments of the included studies, the outcomes of which are presented in Figure 2. Figures 2 and 3 show low risk of bias in the random-sequence generation with conspicuity of unclear judgments for the allocation concealments and blinding criteria.
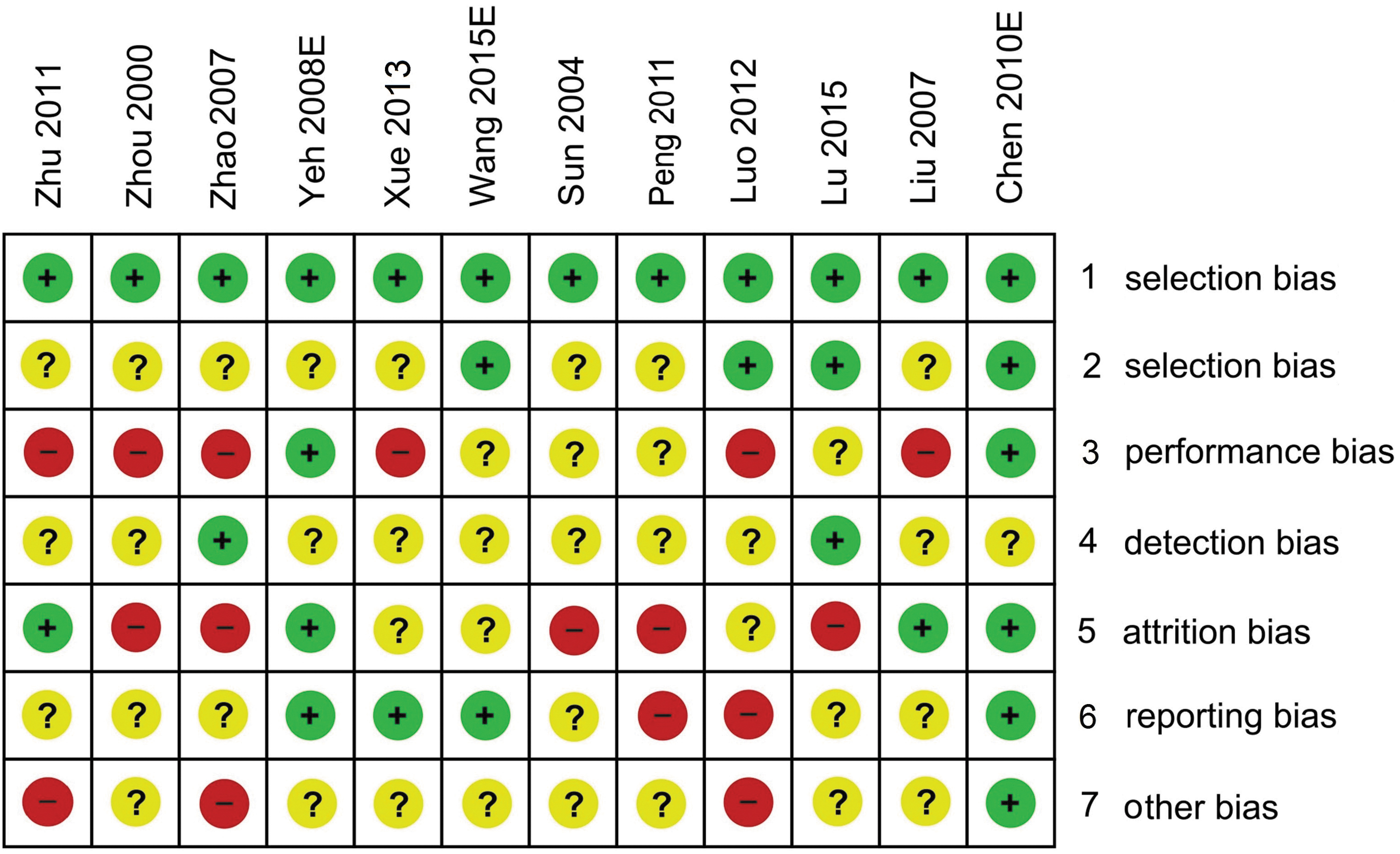
Risk of bias analysis in studies that examined the auricular acupoint stimulation–myopia association. E, English circle colors (green, red, and yellow) and signs in the circles (+, −, and ?) indicate low, high, and unclear risk of bias, respectively.
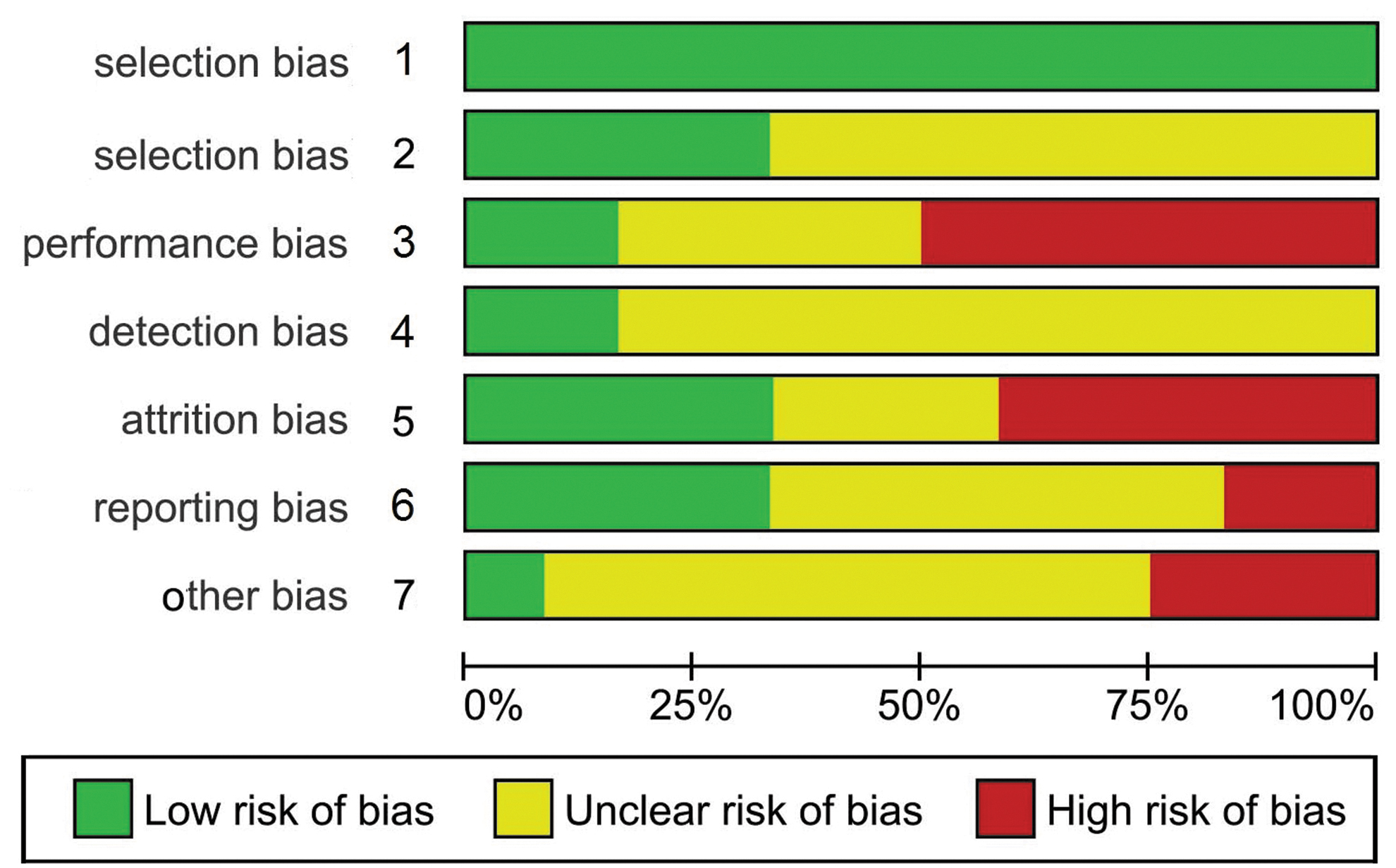
Risk-of-bias summary in studies that examined the auricular acupoint stimulation–myopia association.
Meta-Analysis Outcomes
Figure 4 shows the AAS pooled effect significantly (Pa = 0.003) favoring treatment over the controls (OR: 2.87; 95% CI: 1.44–5.75). This pre-outlier outcome was heterogeneous (Pb < 10–5; I2 = 87%). The Galbraith plot identified 2 studies31,39 as the sources of heterogeneity (outliers), located above the +2 and below the −2 confidence limits (Fig. 5). In Figure 6, the post-outlier outcome (OR: 3.42; 95% CI: 2.58–4.53) showed reduced heterogeneity (Pb = 0.37; I2 = 8%). AAS pooled effects between pre-outlier and post-outlier generated the following outcomes: (1) intensified significance (Pa < 10−5) and (2) increase in magnitude (from 2.8-fold to 3.4-fold). The 2 significant (Pa < 0.05) AAS outcomes (Figs. 4 and 6) were robust, with none of the component studies influencing the pooled ORs. The Egger's regression test showed no evidence of publication bias (Intercept: −0.45; P = 0.84).
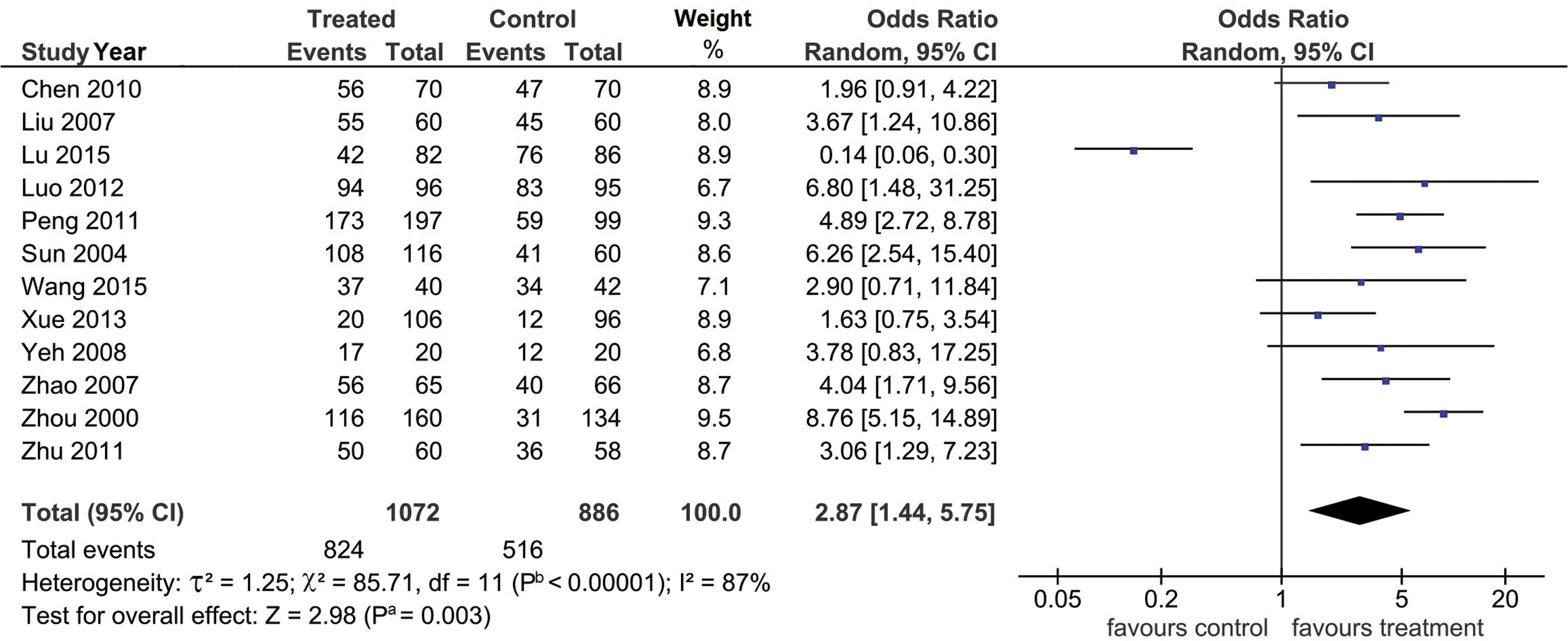
Forest-plot pre-outlier outcome. The diamond denotes the pooled odds ratio (OR), favoring treatment (2.87). Squares indicate the OR in each study. The horizontal lines on either side of each square represent the 95% confidence intervals (CIs). The Z-test for overall effect is highly significant (Pa = 0.003). The χ 2 test shows the presence of heterogeneity (Pb < 0.00001; I2 = 87%). Pa, P-value for association; Pb, P-value for heterogeneity; I2, a measure of variability expressed in %.
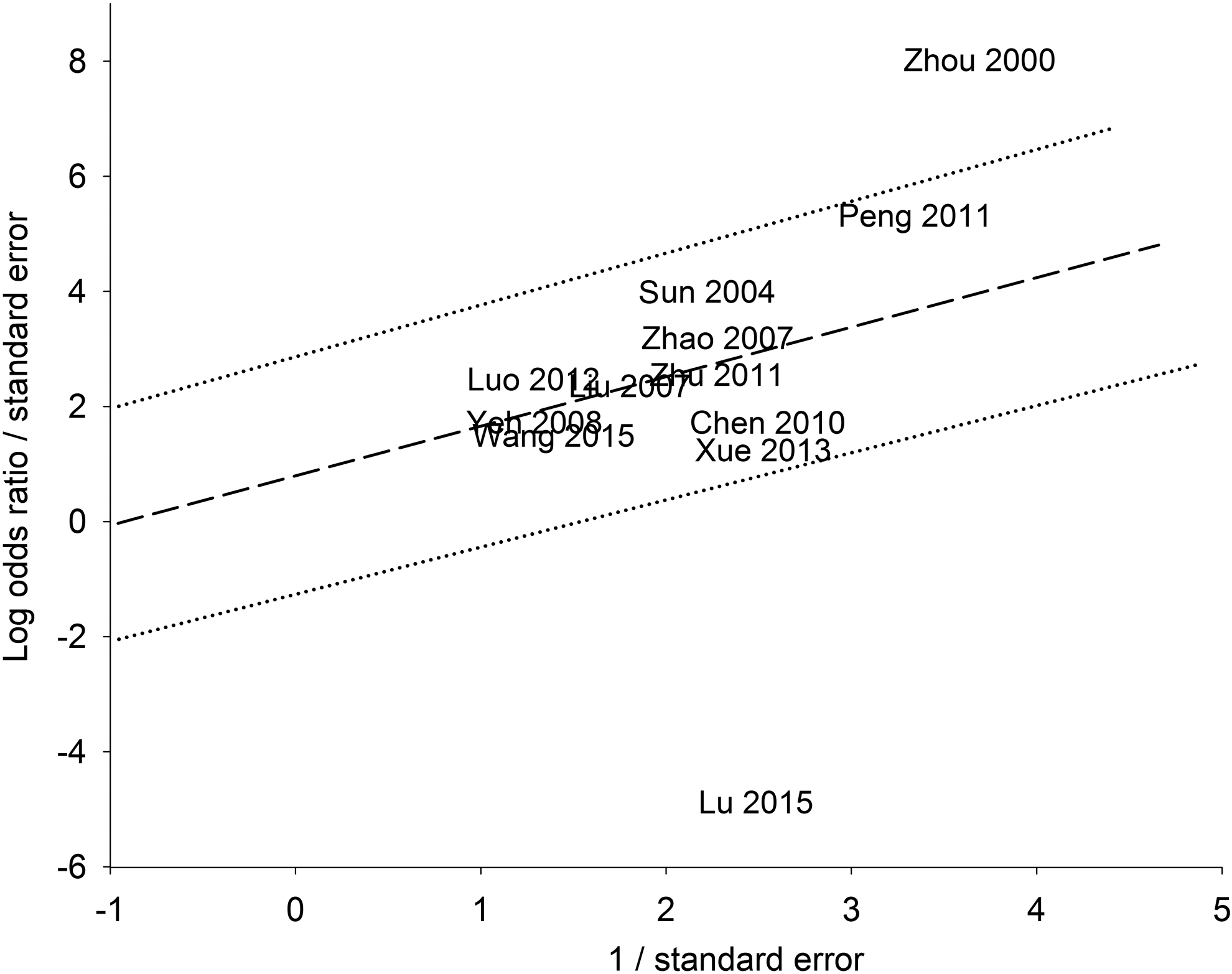
Galbraith-plot analysis. Log, logarithm; the 2 studies above and below the +2/–2 confidence limits are the outliers.
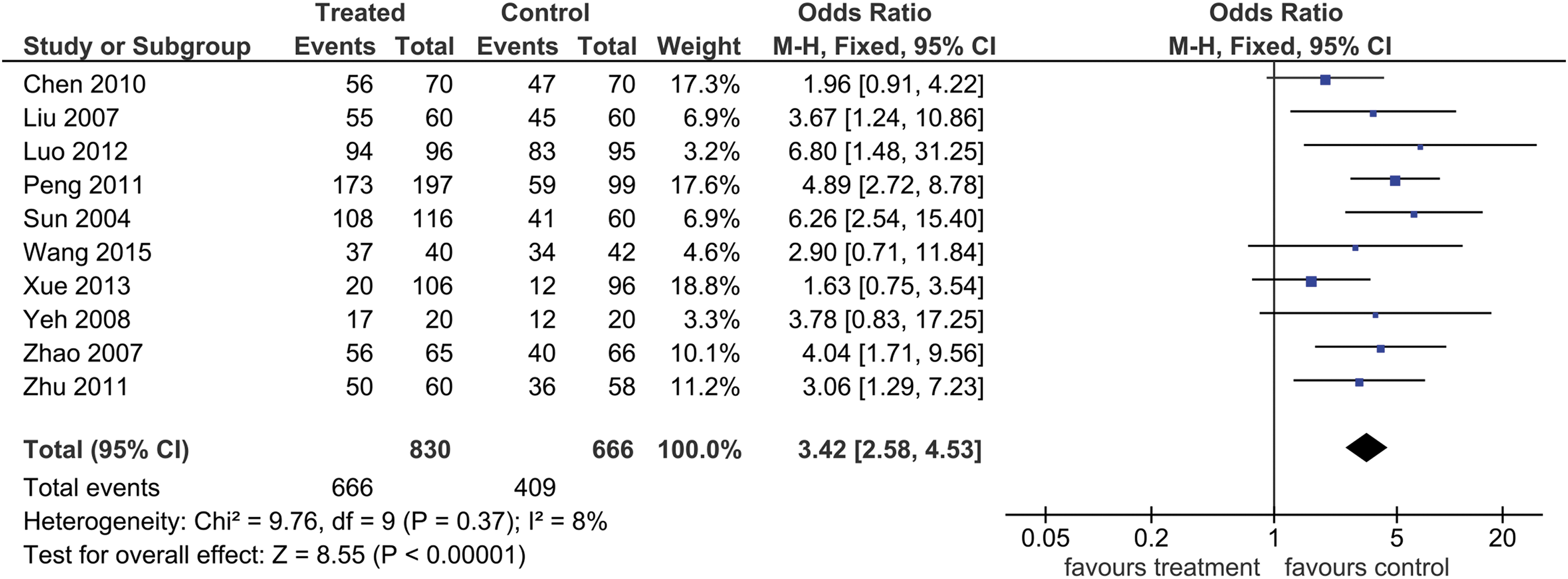
Forest-plot post-outlier outcome. The diamond denotes the pooled odds ratio (OR) favoring treatment (3.42). Squares indicate the OR in each study. Horizontal lines on both sides of each square represent the 95% confidence intervals (CIs). The Z-test for overall effect shows significance (Pa < 0.00001). The χ 2 test indicates nonheterogeneity (Pb = 0.37; I2 = 8%); I2, a measure of variability expressed in %. Pa, P-value for association; Pb, P-value for heterogeneity.
DISCUSSION
Summary of Associations
To the current authors' knowledge, this is the first English-language meta-analysis that examined the role of AAS in controlling myopia. The principal findings of this analysis favored treatment over controls. The level of evidence that supported these findings was clarified when the pre-outlier and post-outlier outcomes (Figs. 4 and 6) were compared. Meta-analysis and statistical features that were altered are as follows (pre-outlier versus post-outlier): (1) significance (Pa): moderate (0.003) versus high (0.00001); (2) magnitude of effect (OR): 2.9-fold versus 3.4-fold; (3) precision of effect: CID 4.31 versus 1.95. With the added features of robustness and lack of bias, these layers of evidence underpinned the finding of AAS being effective for treating myopia. Outlier treatment (Galbraith-plot tool) in this meta-analysis unraveled low-level heterogeneous associations that the component single-studies were not designed to examine. Conflicting outcomes between primary studies may be attributed to their lack of power and small sample sizes; these 2 statistical features that rendered those studies to the risk of Type 1 errors.
Comparison with a Previous Meta-Analysis
The current findings were compared with a previous Chinese-language meta-analysis. 19 That study by Zhang (n = 7) found a 4.1-fold effect, while the current meta-analysis resulted in a modulated 2.8 to 3.4–fold (n = 12) effect. Four differences between the current meta-analysis and that of Zhang 19 were: (1) inclusion of English-language articles versus having all Chinese-language studies; (2) n = 12 in the current meta-analysis versus n = 7 in the other studies; (3) risk of bias was assessed; and (4) the current meta-analysis involved outlier treatment. Zhang 19 did not perform items 3 and 4.
AAS and Myopia
With regard to the Inner Canon of Huangdi, ancient (179–141
The World Health Organization recognized AAS as a microacupuncture system that can produce a positive impact on human physiology. 44 For example, stimulating the ear acupoints (AAS) can elevate endorphin levels and regulate the sympathetic nervous system. 45 In TCM, AAS has been used as a noninvasive intervention for healing and alleviating ill-health conditions, 46 with minimal side-effects, no toxicity, and easy manipulation. 29 Hence, treatment of myopia with AAS is readily acceptable to children. 29 Moreover, AAS intervention reinforces visual-health behaviors in children.47,48 However, AAS intervention is not entirely risk-free; adverse events, such as chest tightness, dizziness, and nausea, have been reported in the literature. 49 Moreover, the ear has several capillaries that make it highly vulnerable to skin inflammations and other infections. 49
Limitations and Strengths of the Meta-Analysis
The limitations and strengths of the current meta-analysis help contextualize the interpretation of the findings.
Limitations included: (1) Confinement of the subjects to young people precluded generalization to other demographic strata. (2) Risk-of-bias judgments were unclear for allocation and blinding. Without an overall score, risk-of-bias judgments can be made from the visual details of the graph, which underscores the weaknesses and strengths of each study based on the criteria set by the Cochrane Collaboration. 20 (3) Heterogeneity of the control subjects whose treatments ranged from none to eye drops to eye exercises.
Strengths included: (1) The outcome measure in common for all of the included studies was visual acuity, which indicated homogeneity of clinical outcomes. This was considered a strong point in this meta-analysis. (2) There was a low risk of bias. (3) Outlier treatment was key to generating significance and reducing heterogeneity. This demonstrated the utility of this meta-analysis tool in elevating the level of evidence for associations. (4) Sensitivity treatment conferred robustness on the significant outcomes. (5) Publication bias was not evident.
CONCLUSIONS
This meta-analysis showed that AAS is an effective therapy for addressing myopia. The evidence presented here may render AAS as an alternative modality in treating this ocular disorder. In spite of the evidence for associations, the complexity of myopia involves interactions between other factors not covered in this meta-analysis. Additional well-designed studies exploring other parameters would confirm or modify these results and add to the extant knowledge about the efficacy of AAS for treating myopia.
Footnotes
AUTHORS' CONTRIBUTIONS
Dr. Sangvatanakul and J. Tangthianchaichana contributed to study conception and design, and translation of articles from Chinese to English. Drs. Sangvatanakul, Tasanarong, Pabalan, and Tharabenjasin performed data and data analysis, and wrote the article. All authors reviewed, revised, and approved its final version.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.