
Abstract
Objective:
Primary dysmenorrhea is a common condition that impacts quality of life significantly. Auricular therapies have shown promise for treating primary dysmenorrhea, but there is a lack of evidence specifically for auricular acupuncture (AA). This study evaluated the safety and efficacy of AA for managing primary dysmenorrhea.
Materials and Methods:
A randomized, double-blinded controlled trial was conducted on 90 females with primary dysmenorrhea: an AA group; n = 45) and a sham-AA (SA) group; n = 45. Specific ear acupoints (i.e., Uterus, Endocrine, Shenmen, Subcortex, Liver, and Kidney) were used for the intervention, which was 1 or 2 days prior to the expected menstruation onset. Outcomes were visual analogue scale (VAS) scores, ibuprofen needs, and adverse events (AEs).
Results:
The AA group had significantly lower VAS scores, compared to the SA group at menstruation onset and for up to 12 hours (mean differences [MDs] and 95% confidence intervals [CIs]: −1.08 [–1.96, −0.21] and −1.17 [–2.16, −0.18], respectively). Both groups had reductions in pain levels, compared to the prior menstrual cycle; the AA group had a significantly greater improvement. The AA group needed fewer ibuprofen tablets (MD: −0.28; 95% CI: −0.58, 0.00]). AEs were mild pain and irritation at insertion sites, all resolved spontaneously with no lasting effects.
Conclusions:
AA is safe. It may be effective for managing primary dysmenorrhea. Further studies are warranted on AA's effectiveness in diverse populations and extended times.
INTRODUCTION
Primary dysmenorrhea is a common condition affecting women of reproductive age, characterized by spasmodic and painful cramps in the lower abdomen before and/or during menstruation. Its prevalence ranges from 45% to 95%,1–3 and the associated pain can last for 8–72 hours after menstruation, varying from moderate to severe intensity. 4 In addition to the physical discomfort, dysmenorrhea has negative implications on various aspects of life, including social and academic performance. 5 The condition can impair concentration in school, lead to increased absenteeism from college and work,6,7 and even have an impact on female brain structure and psychologic well-being. 8 Given the high prevalence and challenges in management, primary dysmenorrhea significantly affects the quality of life and work status of affected individuals.7,9
Management of primary dysmenorrhea involves a range of treatment options, including pharmacologic, nonpharmacologic, and surgical interventions. Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first-line pharmacologic treatment for primary dysmenorrhea. 10 However, long-term use of NSAIDs can lead to adverse effects on the gastrointestinal and nervous systems. 11 Oral contraceptives are commonly used in combination with pain management, but they can cause side-effects, such as nausea, weight gain, and bleeding. 10 Some adolescents have even resorted to self-administration and abuse of NSAIDs for rapid pain relief during menstrual cycles. 6 Furthermore, a significant proportion of women do not respond adequately to NSAIDs. 12 In cases when other therapies are ineffective, surgical interventions, such as laparoscopic uterine-nerve ablation and laparoscopic presacral neurectomy, are considered. However, these interventions are invasive and still leave more than 20% of patients with a condition that is resistant to treatment. 12
According to traditional medicine (TM), menstrual pain is attributed to an obstruction in the flow of Qi and Blood or a Deficiency/Stagnation of these elements, leading to inadequate circulation and pain during menstruation. The underlying cause may involve a Kidney Deficiency in nourishing the Liver or stagnation of Liver Qi, resulting in lower abdominal pain and cramping. 13 TM offers alternative treatment options for primary dysmenorrhea, including herbal remedies, acupuncture, and acupressure. These modalities can alleviate pain by reducing prostaglandin (Pg) levels, modulating nitric oxide, increasing ß-endorphin levels, blocking calcium channels, and enhancing uterine circulatory flow through the uterine pathway. 14
A meta-analysis has demonstrated the effectiveness of acupuncture, including auricular therapies, in reducing primary dysmenorrhea, likely through modulation of Pg levels.15,16 Auricular acupressure, a noninvasive technique, has been commonly used in prior studies, although the specific auricular therapies vary across regions and countries.
Among these modalities, auricular acupuncture (AA), which can involve application of adhesive patches with small needles inserted and fixed at specific acupoints on the ear, has gained popularity. The inserted needles provide continuous stimulation to the acupoints, yielding effectiveness similar to other acupuncture methods. A notable advantage of AA is that patients only require a single procedure per menstrual cycle, whereas other acupuncture treatments necessitate multiple sessions. However, there is a paucity of evidence regarding the use of AA for treating primary dysmenorrhea. To address this research gap, this study assessed the efficacy and safety of AA for reducing menstrual pain.
MATERIALS AND METHODS
Trial Design
This study was a single-center, double-blinded, randomized controlled trial to compare the efficacy and safety of AA (AA group) and sham AA (SA group) therapies for treating primary dysmenorrhea. The study was conducted at the University Medical Center Ho Chi Minh City, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam, a tertiary medical center, from November 2021 to June 2022.
Ethics Statement
Ethical approval was obtained from the Medical Center's institutional ethics committee. Written informed consent was obtained from all participants prior to their inclusion in the study.
The study adhered to the ethical principles outlined in the Declaration of Helsinki and followed the International Conference on Harmonization-Good Clinical Practice guidelines. The design and reporting of the trial followed the Consolidated Standards of Reporting Trials (CONSORT) and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines. 17
This research was also reviewed and approved by the institutional review board of the University of Medicine and Pharmacy at Ho Chi Minh City (No. 607/ HĐĐĐ-ĐHYD, dated November 16, 2021).
Participants
Patients with primary dysmenorrhea were recruited from the Medical Center's outpatient department to participate in the study. Inclusion criteria were: (1) females between ages 18 and 25, each with an active menstrual cycle; (2) menstrual duration lasting between 3 and 8 days, with a menstrual cycle length of 21–35 days; (3) experiencing dysmenorrhea with a visual analogue scale (VAS) score of 4 points or higher in at least 3 menstrual cycles within the past 6 months, including the most-recent cycle.
Exclusion criteria were: (1) previous diagnosis of endometriosis, adenomas, ovarian cysts, or uterine fibroids; (2) suspected secondary dysmenorrhea detected by ultrasound; (3) use of contraceptives within 1 month or pain relievers within 3 days prior to enrollment; (4) chronic use of pain relievers; (5) history of drug or alcohol abuse; (6) presence of an active disease requiring treatment; (7) any ear infections; (8) previous auricular acupuncture treatment; (9) hypersensitivity reaction to acupuncture; and (10) pregnancy.
Randomization and Blinding
Eligible participants were randomly assigned to either the AA or SA group in a 1:1 ratio. Randomization was conducted with SAS software, version 9.4, using block randomization with a block size of 6. A total of 15 random blocks were created. Sequentially numbered sealed envelopes containing the randomization codes were used for allocations. Eligible patients were assigned to receive treatment based on the order of recruitment.
To maintain blinding, the patients were unaware of the treatment they received. The physician responsible for administering the treatment was aware of the group allocations but did not participate in outcome assessments or data analysis. Outcome assessors and data analysts were blinded to the treatment allocations.
Interventions
Each intervention was performed 1 or 2 days prior to the onset of menstruation, taking into consideration the patient's menstrual history and premenstrual symptoms. An experienced TM expert with more than 5 years of AA experience performed the procedures following the guidelines set by the Vietnamese Ministry of Health.
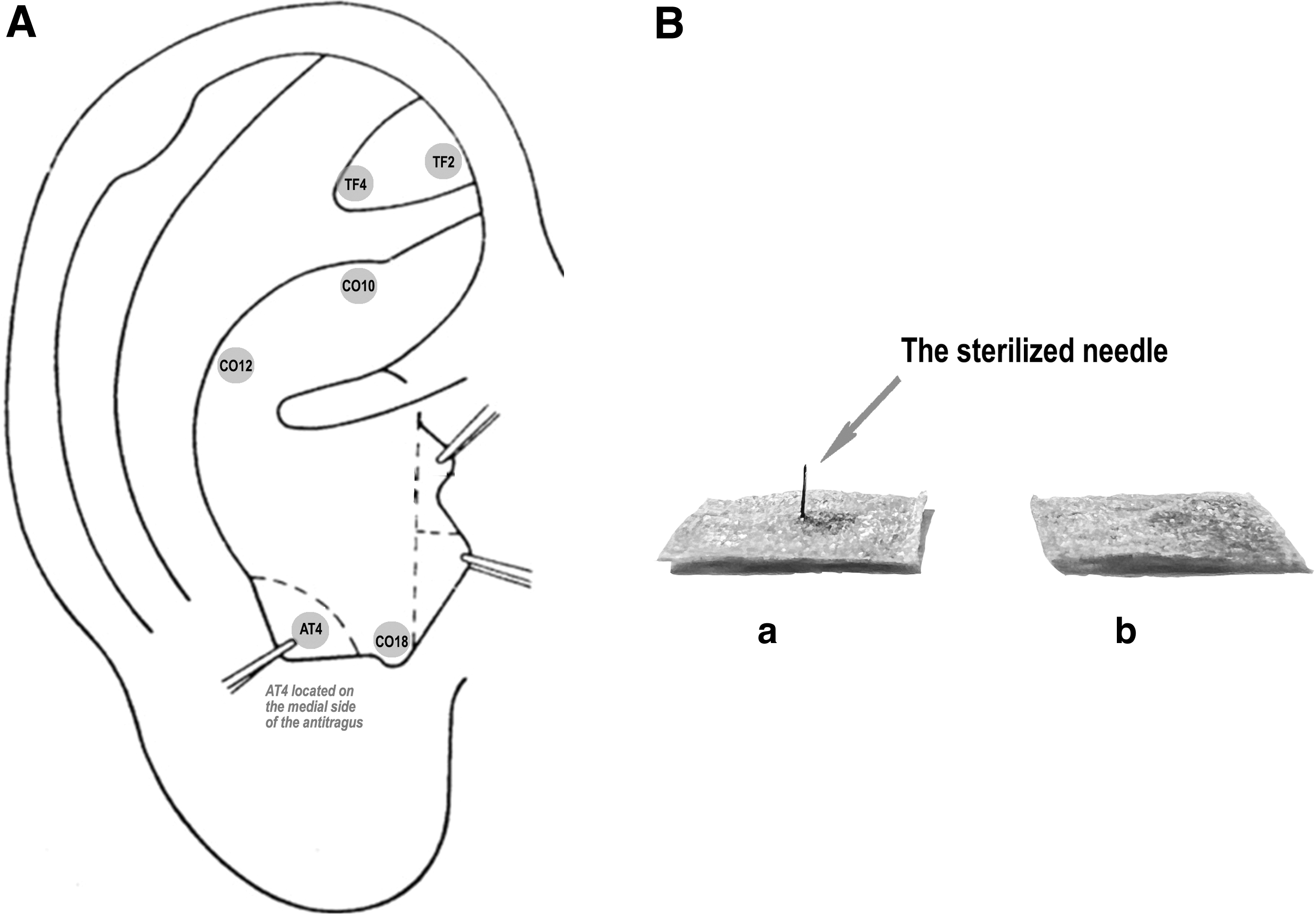
Both the AA and SA groups received the same AA formula. Six acupoints were selected, including Uterus (TF2), Endocrine (CO18), Shenmen (TF4), Subcortex (AT4), Liver (CO12), and Kidney (CO10) points. The acupoint locations were determined based on the standards set by the World Federation of Acupuncture–Moxibustion Societies (Fig 1A). 18 One ear was chosen for the intervention based on the presence of a painful reaction. The physician applied pressure to the Uterus point on both sides of the ear using a blunt object. The ear with a more pronounced painful reaction was selected for treatment. If neither ear exhibited a reaction at the Uterus point, other acupoints were tested using the same procedure, and the ear with a greater number of acupoints showing painful reactions was chosen.
Two types of patches (10-mm square) were used, 1 with a sterilized needle (0.2 × 2 × 1.5 mm) for the AA group and another without a needle for the SA group (Fig. 1B). The patches were left in place on the acupoints for up to 5 days. Participants were instructed to apply pressure to these acupoints for ∼1 minute every 6 hours. In cases of severe menstrual pain, oral ibuprofen (200 mg) was permitted with a minimum interval of 6 hours between doses.
Acupoint locations and device:
Outcomes
The primary efficacy outcome was the pain score, assessed using the VAS. The VAS is a self-reported pain-rating system wherein a 10-cm line represents a continuum from “no pain” on the left side (scored as 0) to the “worst pain” on the right side (scored as 10). 19 Each participant was instructed to mark a single point on the scale indicating the intensity of her pain. The highest VAS score reported during the previous menstrual cycle was considered the baseline score (preprocedure). In the current menstrual cycle, VAS scores were recorded at specific time points: at menstruation onset (T0); after 30 minutes (T-30 mins); after 60 minutes (T-60 mins); after 12 hours (T-12 hrs); after 24 hours (T-24 hrs); after 48 hours (T-48 hrs); and after 72 hours (T-72 hrs). Participants also reported the highest VAS score experienced throughout the entire menstrual cycle (postprocedure).
The secondary efficacy outcomes included the requirement for ibuprofen and the number of 200 mg tablets taken during the 5-day intervention.
The safety outcome was the occurrence of adverse events (AEs) related to the interventions. Expected AEs included pain at insertion, dizziness, local discomfort, local skin irritation (itching and redness), local inflammation and bleeding, chondritis, and nausea. 20 Serious adverse events (SAEs) were recorded if AEs resulted in severe consequences, such as death, life-threatening conditions, hospitalization (initial or prolonged), disability or permanent damage, or interventions required to prevent permanent impairment or damage.
Sample-Size Calculation
The sample size was determined based on the detection of the treatment-effect difference, with a Type-1 error of 0.01 and a Type-2 error of 0.2, using the primary outcome measure of VAS score after the intervention. Previous studies reported a mean difference in VAS scores between intervention and placebo groups of ∼1.5, with standard deviations (SDs) of 2.16 and 1.69, respectively.21–23 A sample size of 40 participants in each group was required. Considering a potential dropout rate of 10%, a sample size of 45 participants in each group was chosen.
Statistical Analysis
An intention-to-treat dataset was used for analysis of efficacy outcomes, including all randomized participants, regardless of protocol adherence, premature discontinuation, or loss to follow-up. VAS scores at different time points were presented as median (25th, 75th percentiles). A Wilcoxon rank-sum test was used to assess differences between the AA and SA groups in terms of VAS scores and the number of ibuprofen 200-mg tablets used. The requirement for ibuprofen, AEs, and SAEs were presented as frequencies and percentages, and between-group comparisons were performed using Fisher's exact test. Risk ratios (RRs) with 95% confidence intervals (CIs) were calculated for binary outcomes, while mean differences (MDs) with 95% CIs were calculated for continuous outcomes. Statistical analyses were performed using the statistical software R version 4.1.0, with a significance level set at P < 0.05.
RESULTS
Between November 2021 and June 2022, a total of 132 females were screened for eligibility. Among them, 90 participants met the inclusion criteria and were randomly assigned to either the SA group (n = 45) or the AA group (n = 45). There were no dropouts or participants lost to follow-up during the study. See Figure 2 for study flow diagram.
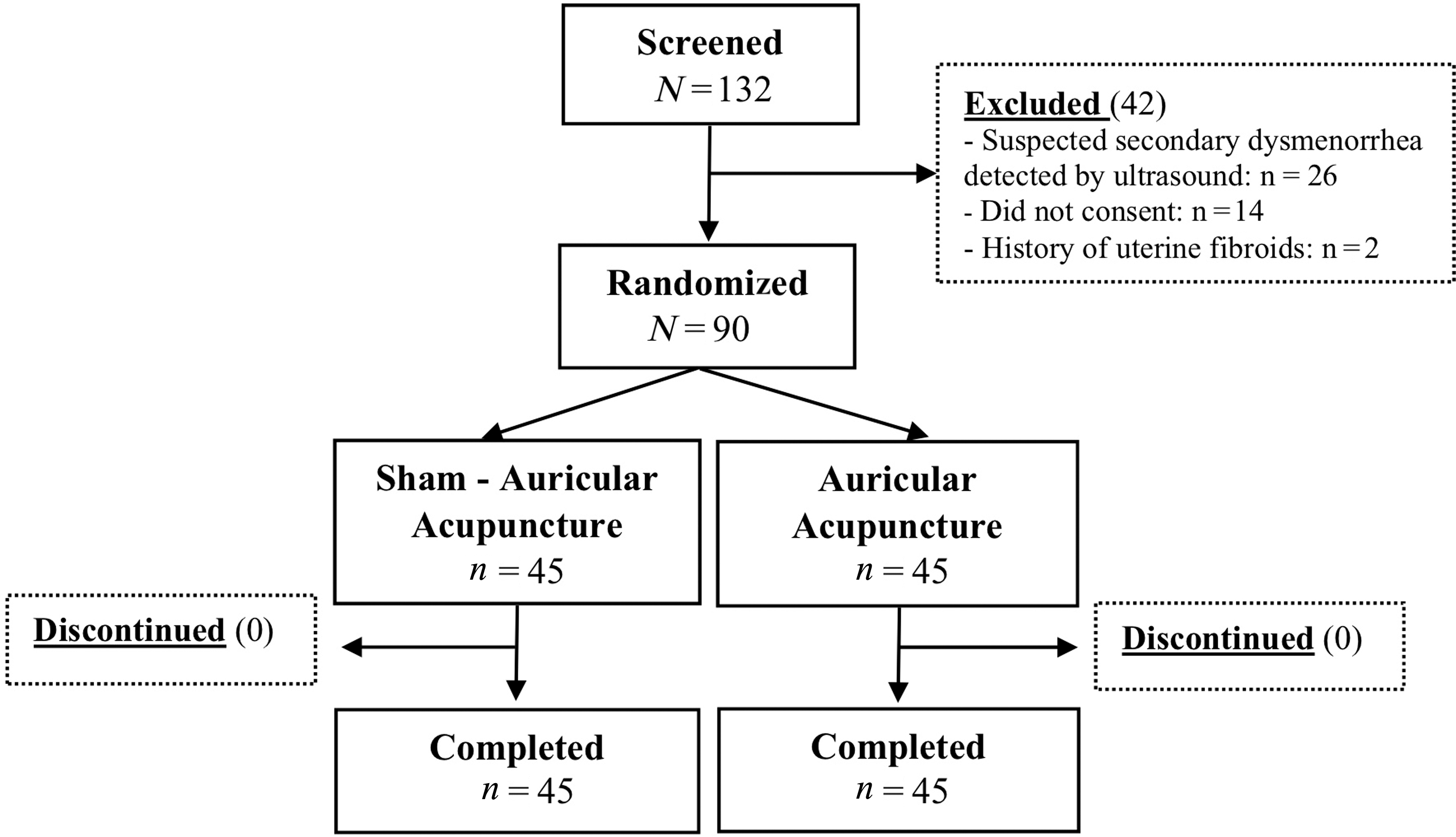
Flow diagram of patient selection.
Baseline Characteristics
Table 1 shows the baseline demographic and clinical characteristics of the randomized participants. The median age in both groups was 21 years, with a median age at menarche of 13 years. Most participants experienced the onset of dysmenorrhea within 2 years of menarche. In the last menstrual cycle, the median of the highest VAS score recorded was 7 in the SA group and 8 in the AA group. The majority of participants had normal weight, and family history of dysmenorrhea was common in both groups. More than 50% of the participants had used NSAIDs in the last cycle. Overall, the baseline characteristics were well-balanced between the SA and AA groups.
Demographic Characteristics
Statistics are median (25th, 75th percentiles) and n (%).
Preintervention VAS score is the highest VAS score in the last menstrual cycle.
SA, sham auricular acupuncture; AA, auricular acupuncture; yrs, years; d, days; VAS, visual analogue scale; BMI, body mass index; NSAID, nonsteroidal anti-inflammatory drug.
VAS Score
The participants in both the SA and AA groups experienced an increase in pain intensity within the first 60 minutes after the onset of menstruation, followed by a gradual decrease over time. By the first 72 hours, pain had mostly resolved in almost all participants in both groups (Fig. 3). During the first 12 hours since the onset of menstruation, the AA group had a significantly lower VAS score compared to the SA group (Table 2). The postintervention VAS score was significantly lower in the AA group, with a MD of −1.06 (95% CI: −1.94, −0.18). This indicates that the AA group experienced a greater reduction in pain intensity, compared to the SA group. The MD for the decrease in VAS score from pre- to postintervention was 1.60 (95% CI: 0.83, 2.36), indicating a significant difference between the two groups (Fig. 3 and Table 2).
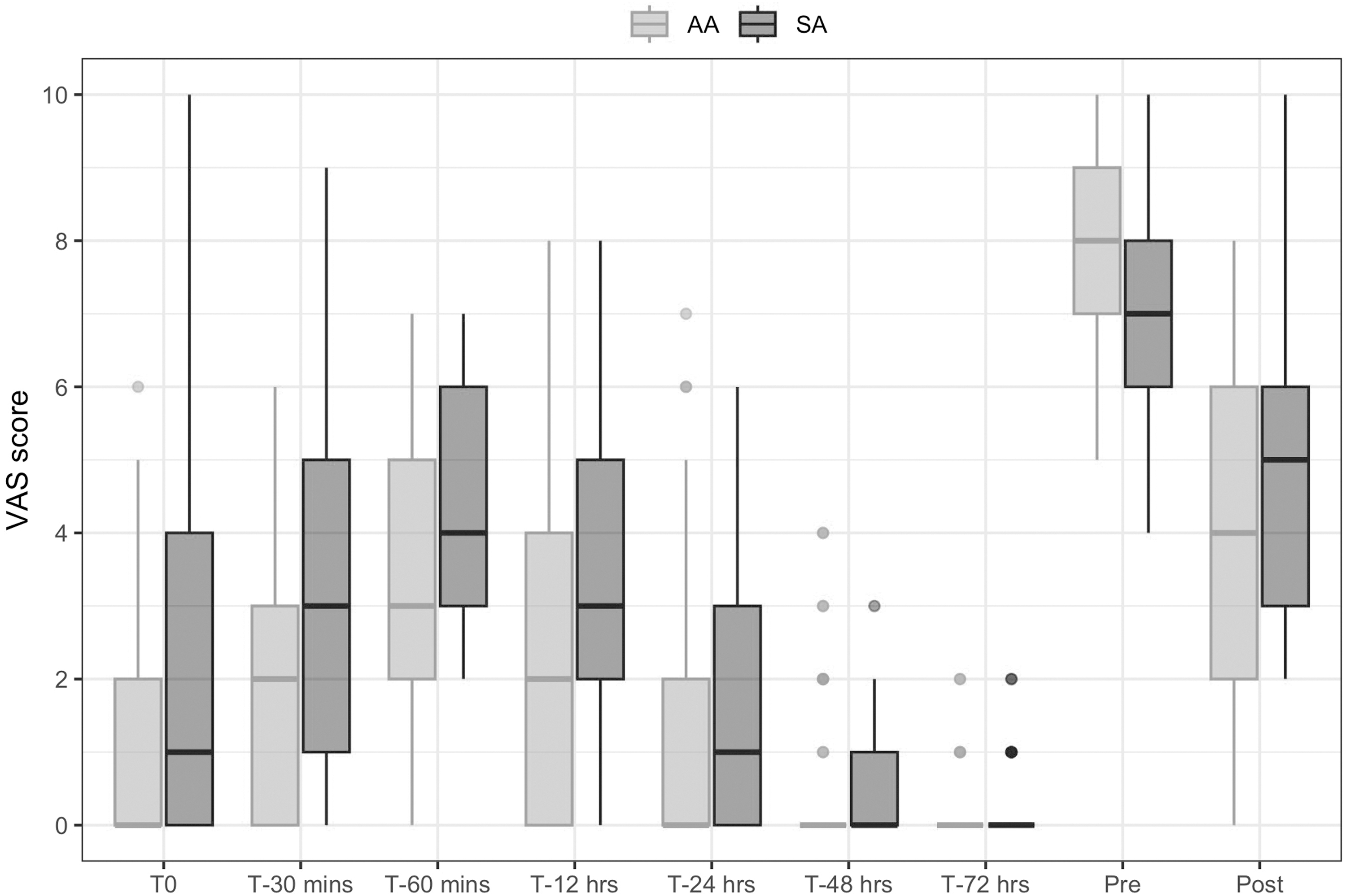
Visual analogue scale (VAS) scores by groups before and after treatments. T0 is the time of menstruation onset. Preintervention VAS score is the highest VAS score in the last menstrual cycle. Postintervention VAS score is the highest VAS score in the current menstrual cycle. AA, auricular acupuncture; SA, sham auricular acupuncture; mins, minutes; hrs, hours.
Clinical Outcomes Between the Groups
Statistics are median (25th, 75th percentiles), mean ± standard deviation and n (%).
Bolded P-value indicates significant result.
Postintervention VAS score is the highest VAS score in the current menstrual cycle.
SA, sham auricular acupuncture; AA, auricular acupuncture; MD, mean difference; RR, risk ratio; CI, confidence interval; VAS, visual analogue scale; T, time; min, minutes; hrs, hours.
Ibuprofen Requirement
The AA group had a significant reduction in requirement for ibuprofen, compared to the SA group. The RR for ibuprofen requirement was 0.54 (95% CI: 0.30, 0.96), indicating a lower likelihood of needing ibuprofen in the AA group. The MD for the number of ibuprofen tablets used was −0.28 (95% CI: −0.58, 0.00), suggesting a lower consumption of ibuprofen in the AA group compared to the SA group (Table 2).
Safety Outcome
Two AEs were observed in the study, including pain at the insertion site and local irritation. Pain at the insertion site occurred shortly after the procedure and resolved within 1 day. Itching, however, typically appeared 3 days after the intervention and resolved upon removal of the patch at the end of the study. The AA group had a significantly higher level of pain at the insertion site compared to the SA group (RR: 4.00; 95% CI 0.89, 17.80]), while the incidence of local irritation was similar between the 2 groups (Table 2). All reported AEs were mild and resolved spontaneously without the need for treatment. There were no lasting sequelae associated with the reported AEs.
Data Availability
The data that support the findings of this study are available from the corresponding authors, upon reasonable request.
DISCUSSION
This study demonstrated that AA was more effective than SA for reducing pain intensity during menstruation. AA significantly reduced VAS scores in the first 12 hours after menstruation onset and also decreased the highest VAS score in the current menstrual cycle. Additionally, the AA group had a decreased requirement for ibuprofen, further indicating its pain-reducing effect. Importantly, this study confirmed the safety of AA as a procedure.
Auricular therapy encompasses various forms, with acupuncture and acupressure being 2 common long-term methods. Both methods utilize a patch to provide stimulation to acupoints. AA involves the use of needles, while auricular acupressure utilizes Vaccaria seeds or magnetic pellets. Previous studies using auricular acupressure in women with primary dysmenorrhea have shown significant pain reduction, compared to sham treatment. 24 The current study using AA yielded similar results, indicating the effectiveness of both forms of auricular therapy for reducing menstrual pain in women with primary dysmenorrhea. In this study, AA was chosen over auricular acupressure based on the belief that needle insertion provides continuous stimulation, potentially leading to better outcomes. Previous research has suggested that auricular acupressure may have a limited effect beyond 2–3 days from the onset of menstrual pain.16,23,25 However, further studies are needed to compare the effects of acupuncture and acupressure directly for relieving menstrual pain.
In most previous studies on auricular therapies, the interventions were performed after the onset of menstrual pain. However, in the current study, similar to another study, 21 the procedure was conducted before the onset of menstruation. The current authors believe that early intervention with AA prior to menstruation may be more effective and beneficial for patients as this approach helps prevent the experience of severe menstrual pain. Previous research has shown that even after 3 days of treatment from the onset of extreme menstrual pain, patients still experienced pain. 21 In contrast, in the current study, the pain had nearly disappeared after 24 hours in the AA group and 48 hours in the SA group. While this hypothesis faces challenges due to differences in sample characteristics and interventions, it is worth exploring in future studies.
An intriguing finding in this study, consistent with previous research,21,26 was that even the sham procedure significantly reduced menstrual pain and reduced the requirement for NSAIDs, compared to the previous menstrual cycle. The sham procedure in this study did not involve insertion of seeds or needles, but it included regular stimulation of the acupoints every six hours. Additionally, both the SA and AA groups received stimulation at the Uterus auricular point and/or other acupoints prior to the intervention, which can be considered a short-term acupressure stimulation. A single-group experimental study also raised the suspicion that auricular therapy may produce prolonged pain reduction, lasting until the next menstrual cycle. 25 This suggests that initial stimulation or regular pressing on the acupoints can have an effect, even without the use of seeds or needles.
In a systematic review, the most commonly reported AEs associated with AA were tenderness and pain at the needling site, while adverse skin reactions such as irritation and redness were frequently attributed to the adhesive tape used. 20 The current study findings align with these reports. Pain was predominantly observed in the AA group, attributable to needle insertion, while skin irritation was observed in both groups, likely caused by the adhesive tape. Importantly, all AEs were mild and resolved spontaneously without requiring treatment, consistent with previous findings that highlight the safety of AA as a therapy. 20
The current study did have several limitations that should be acknowledged. First, the study focused exclusively on reproductive-age women and had a relatively small sample size, which may restrict the generalizability of the results. Secondly, the sham-AA method, while implemented to blind participants to the needle-insertion experience, may not have fully achieved complete blinding. An attempt was made to minimize this by excluding participants with prior AA experience. Finally, the study only assessed the effects of AA within a single menstrual cycle, thus lacking evidence on long-term effects.
CONCLUSIONS
This study demonstrated that AA administered just prior to menstruation is a safe and effective intervention for reducing pain intensity in women with primary dysmenorrhea. AA should be considered as a routine option for patients with primary dysmenorrhea before the onset of menstruation. Future research should encompass diverse populations and include longer follow-up times to elucidate the efficacy and durability of AA further as a therapeutic approach to menstrual-pain management.
Footnotes
ACKNOWLEDGMENTS
The authors thank the staff at the University Medical Center Ho Chi Minh City (the third branch) who assisted in the recruitment, treatment, and follow-up of the patients in this study. The authors also gratefully acknowledge the patients for participating in the study.
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
No funding was provided for this project.
CME Quiz Questions
Publication date: February 12, 2024
Expiration date: February 28, 2027
None of the authors, editors, or reviewers of this educational activity, have relevant financial relationship(s) with ineligible companies to disclose.
Articles in Medical Acupuncture will focus on acupuncture research through controlled studies (comparative effectiveness or randomized trials); provide systematic reviews and meta-analysis of existing systematic reviews of acupuncture research and provide basic education on how to perform various types and styles of acupuncture. Participants in this journal-based CME activity should be able to demonstrate increased understanding of the material specific to the article featured and be able to apply relevant information to clinical practice.
You may earn CME credit by reading the CME-designated article in this issue of Medical Acupuncture and taking the quiz online. A score of 75% is required to receive CME credit. To complete the CME quiz online, go to ![]() – AAMA members will need to login to their member account. Non-members have opportunity to participate for small fee.
– AAMA members will need to login to their member account. Non-members have opportunity to participate for small fee.