
Abstract
Campylobacter jejuni is widely recognized as a leading cause of bacterial gastroenteritis worldwide. While its acute effects on human health are well documented, a growing body of research suggests that its impact extends far beyond transient infections. Emerging evidence indicates that C. jejuni may contribute to chronic inflammatory conditions and even tumorigenesis, particularly within the gastrointestinal tract. However, the potential role of this pathogen in cancer development remains underexplored, leaving a critical gap in the current literature. This review aims to bridge this gap by providing a comprehensive analysis of C. jejuni’s dual role as both a foodborne pathogen and a potential catalyst for long-term disease. We examine its transmission pathways, unique virulence factors, and evolving antimicrobial resistance patterns, highlighting their implications for public health. More importantly, we explore recent findings that suggest a mechanistic link between persistent C. jejuni infection, chronic inflammation, and carcinogenesis, focusing on its ability to induce deoxyribonucleic acid damage and immune evasion. By synthesizing insights from microbiology, epidemiology, and clinical research, this review offers a novel perspective on C. jejuni, shifting the focus beyond its acute pathogenicity to its broader health implications. In doing so, it underscores the urgent need for further studies to elucidate its oncogenic potential and inform new strategies for prevention and intervention. This review not only advances our understanding of C. jejuni’s impact on human health but also calls attention to a pressing yet overlooked research frontier in infectious disease and cancer biology.
Keywords
Introduction
Campylobacter jejuni stands as the predominant cause of bacterial foodborne illnesses in the United States and Europe, with the European Food Safety Authority (EFSA) identifying it as the most frequent pathogen in European Union (EU) foodborne outbreaks (EFSA, 2022). In 2019, the EU reported 224,972 confirmed campylobacteriosis cases (59.9 per 100,000 population), with stark regional disparities: Czechia (215.0) and Slovakia (141.1) had the highest rates, while Bulgaria (3.3), Cyprus (2.4), Poland (1.9), and Romania (4.1) reported the lowest (EFSA and ECDC, 2019; European Centre for Disease Prevention and Control, 2019). Trends from 2015 to 2019 revealed rising cases in Italy, Latvia, Portugal, and Romania, contrasting with a decline in Hungary, reflecting differences in surveillance, dietary habits, and public health initiatives (EFSA and ECDC, 2019; Koutsoumanis et al., 2021). In the United States, the Center for Disease Control (CDC) estimates 1.5 million annual infections (∼20 per 100,000), though underreporting and diagnostic variances may explain lower rates compared with the EU (CDC, 2020; Kaakoush et al., 2015). Both regions identify poultry—especially undercooked meat—as the primary infection source, necessitating targeted interventions in food safety and consumer education.
C. jejuni exhibits unique pathogenic adaptations, including N-linked protein glycosylation for host colonization and cytolethal distending toxin (CDT)-mediated cell cycle disruption (Dasti et al., 2010). Unlike classical enteric pathogens, it relies on host factors and environmental adaptability, with flagella serving dual roles in motility and antigen secretion (Burnham and Hendrixson, 2018). Genomic analyses are critical for unraveling its virulence, antimicrobial resistance (AMR), and transmission dynamics.
AMR in C. jejuni poses escalating threats, driven by gyrA mutations (fluoroquinolone resistance) and cmeABC efflux pumps (macrolide resistance) (Barata et al., 2024). Horizontal gene transfer and global food trade exacerbate resistance spread, underscoring the need for stringent surveillance. Emerging evidence also links C. jejuni to chronic inflammation and tumorigenesis, raising questions about its long-term health impacts. This review synthesizes recent insights into transmission pathways, virulence mechanisms, AMR challenges, and potential oncogenic roles, aiming to inform public health strategies and future research directions.
Genetic complexity of C. jejuni
Genomic analyses have revealed the intricate genetic landscape underpinning C. jejuni’s pathogenicity and resistance. For instance, strain YH002, isolated from beef liver, harbors unique features such as an integrated phage, multiple AMR genes, and a Phd-Doc (Prevents host death-Death on curing) toxin–antitoxin system, correlating with resistance to amoxicillin and tetracycline. Amino acid changes affecting motility further illuminate mechanisms of AMR and motility (Ghatak et al., 2020).
Pangenome studies emphasize this genetic diversity. Cao et al. identified 900 core and 4621 accessory genes among 173 strains (Cao et al., 2021). Similarly, Rodrigues et al. (2023) found that lineage-specific genomic variations influence both virulence and resistance, underlining the need to consider these differences when assessing adaptation and pathogenicity.
A meta-analysis of C. jejuni genomes revealed low plasticity, with most genes conserved and only 599 variable genes nearly half localized to previously defined variable loci. This genetic stability is essential for maintaining core functions and provides robust markers for genotyping (Taboada et al., 2004).
Clinical studies, such as one involving perimyocarditis in a family, identified single nucleotide polymorphisms (SNPs) in phase-variable genes, suggesting that phase variation during human colonization modulates virulence and can lead to severe complications (Ortega-Sanz et al., 2023). Such cases link genomic changes directly to disease outcomes.
On a global scale, multilocus genotype analyses demonstrate clonal dispersal of sequence types across continents, yet reveal marked genetic differentiation among populations. These findings have significant implications for food security and public health (Poorrashidi et al., 2024).
Comparative genomics also highlights the role of C. jejuni-integrated elements (CJIEs) and hypervariable regions in driving diversity, informing the development of improved genotyping tools (Parker et al., 2006).
Genomic investigations during outbreaks, such as the Hangzhou incident, confirmed the clonal nature of the event and underscored the value of genomic tools for precise outbreak tracking (Yu et al., 2020).
Research on Campylobacter coli from turkeys revealed interspecies DNA acquisition from C. jejuni, especially between cydA and aspA, illustrating the dynamic nature of genetic exchange and its impact on adaptation (Chan et al., 2008).
Microarray-based comparisons of human isolates showed a core genome comprising about two-thirds of genes, with conserved virulence determinants, highlighting the species’ complexity and the need for advanced epidemiological tools (Dorrell et al., 2001).
Direct transmission studies, such as those on strain M1 from chicken to human, identified a pangenome of 2427 gene families, providing insights into core and auxiliary genes that influence virulence and diversity (Friis et al., 2010).
Despite low genome plasticity, C. jejuni adapts via horizontal gene transfer and phase variation. While stability may slow resistance emergence, mechanisms like point mutations and plasmid acquisition still enable adaptation (Sheppard et al., 2011; Yahara et al., 2016). Further research should clarify how this stability shapes long-term evolution under selective pressures.
High-resolution transcriptome mapping revealed strain-specific regulatory features and RNA repertoires, with SNPs in promoter regions leading to distinct transcriptional outputs and the discovery of a minimal CRISPR (clustered regularly interspaced short palindromic repeats) system. These regulatory differences contribute to phenotypic variation and may inform targeted therapies (Dugar et al., 2013).
Whole-genome sequencing (WGS) has been instrumental in elucidating C. jejuni diversity and pathogenicity across sources and regions, identifying key determinants of virulence and resistance (Table 1). This breadth of research underscores the value of WGS in tracking the evolution and spread of C. jejuni.
Whole-Genome Sequencing Studies on Campylobacter jejuni
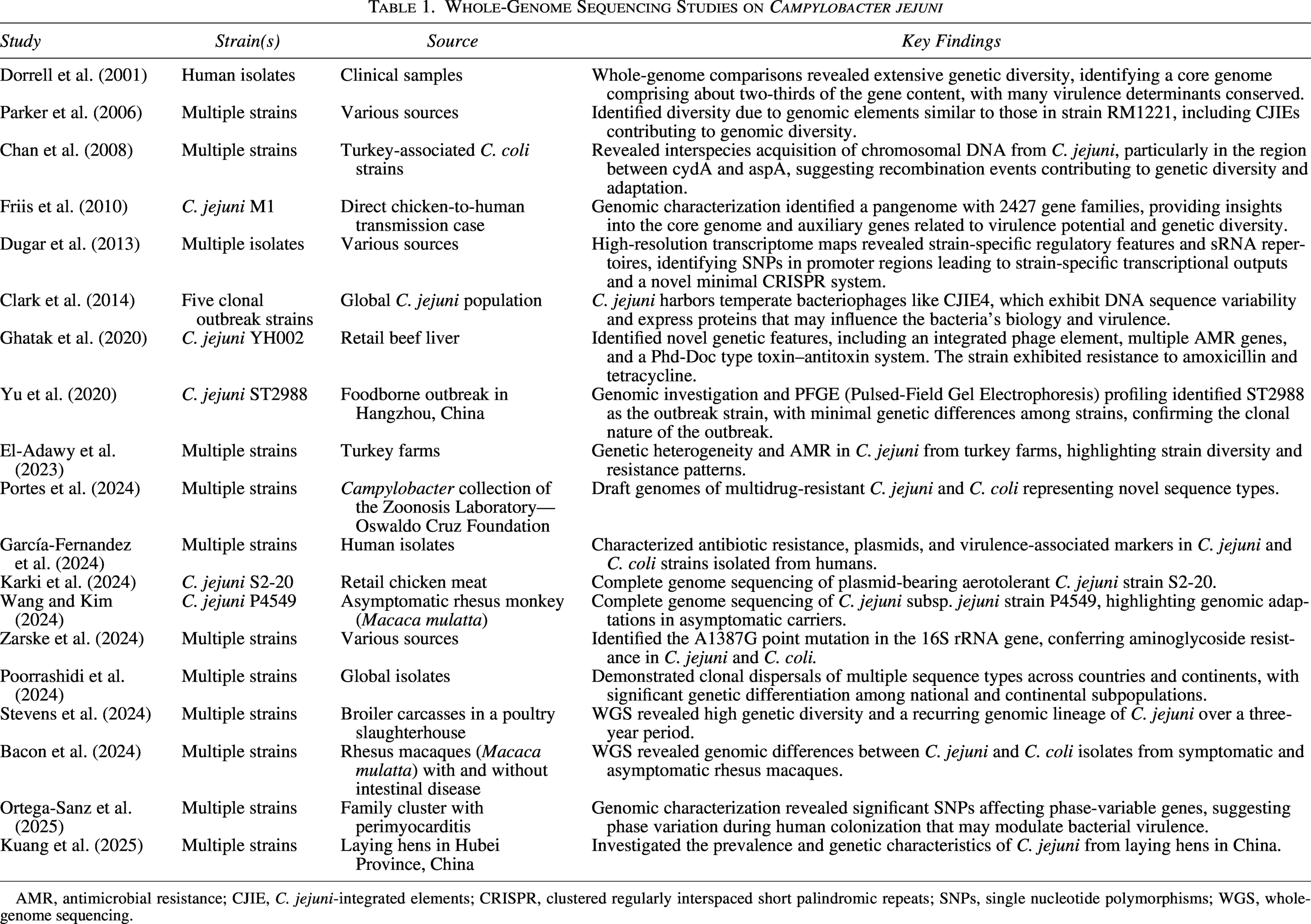
AMR, antimicrobial resistance; CJIE, C. jejuni-integrated elements; CRISPR, clustered regularly interspaced short palindromic repeats; SNPs, single nucleotide polymorphisms; WGS, whole-genome sequencing.
AMR in C. jejuni
AMR in C. jejuni is a growing public health concern worldwide, as emphasized by the CDC and the World Health Organization (Zhang et al., 2020; Hull et al., 2021) The rise of resistance, particularly to fluoroquinolones and macrolides, threatens the effectiveness of treatments for severe infections (Zhang et al., 2020; Ghielmetti et al., 2023). This situation calls for ongoing surveillance and urgent measures to preserve therapeutic options.
Recent advances in monitoring AMR rely on WGS and phenotypic assays, which have proven highly effective for tracking resistance trends. In North Carolina, 90.4% of Campylobacter isolates carried AMR genes, with high resistance to tetracyclines, beta-lactams, and aminoglycosides (Hull et al., 2021). In England and Wales, strong concordance between phenotypic resistance and genotypic determinants confirmed the reliability of WGS for AMR surveillance (Painset et al., 2020). These findings highlight the value of genomic tools for both surveillance and deeper understanding of AMR dynamics.
Global studies reveal significant regional variations in AMR patterns. In Iran, C. jejuni isolates exhibited high resistance to tetracycline, ciprofloxacin, and nalidixic acid, with clear links between resistance and genomic clusters (Divsalar et al., 2019). In South Africa, beef cattle were identified as a reservoir for multidrug-resistant (MDR) Campylobacter (Karama et al., 2020). In China, resistance rates have increased over time, with specific mutations in the 23S rRNA gene associated with erythromycin resistance (Zhou et al., 2016; Zhang et al., 2020). Recent data from Peru showed high prevalence of the cmeRABC operon conferring resistance to fluoroquinolones and macrolides in poultry and children (Rodrigues et al., 2023). In China, C. coli isolates displayed higher MDR rates than C. jejuni, with notable genomic diversity and multiple resistance genes (Li et al., 2025). In Indonesia, nearly all C. jejuni isolates from chickens were resistant to enrofloxacin, with detection of the gyrA gene in all cases (Yanestria et al., 2024). In Korea, high resistance to ciprofloxacin and tetracycline was reported among C. jejuni isolates (Lee et al., 2017). In Northwest Ethiopia, AMR patterns in isolates from children under five revealed resistance to ciprofloxacin and tetracycline, and some to erythromycin, with C. coli showing higher resistance than C. jejuni but erythromycin remaining largely effective (Worku et al., 2024).
The molecular mechanisms behind AMR in C. jejuni are diverse. Mutations in the gyrA gene drive quinolone resistance, the tet(O) gene mediates tetracycline resistance, and both the ermB gene and alterations in the CmeABC efflux pump contribute to macrolide resistance (Ghielmetti et al., 2023; Moser et al., 2020; Zhou et al., 2016; Liao et al., 2022). These mechanisms enable C. jejuni to persist in environments with antibiotic exposure, complicating infection management.
The prevalence of AMR in C. jejuni highlights the need for robust surveillance and effective control strategies. Interspecies gene transfer between C. coli and C. jejuni further complicates the AMR landscape, underlining the necessity of continuous research to monitor evolutionary trends and emerging resistance (Hull et al., 2021; García-Fernandez et al., 2024). Advanced gene network analyses have identified the importance of ribosomal proteins in resistance mechanisms (Kim et al., 2024). As the AMR situation evolves, future studies should focus on molecular characterization of resistance and the development of strategies to limit AMR spread in Campylobacter spp. (Liao et al., 2022; Ghielmetti et al., 2023).
Addressing the escalation of AMR in C. jejuni requires a comprehensive approach, combining advanced genomic techniques, enhanced surveillance, and innovative therapeutic strategies to protect public health and maintain antibiotic efficacy.
C. jejuni and chronic inflammation
C. jejuni is a leading cause of gastroenteritis, but its effects often extend to chronic inflammatory conditions such as reactive arthritis, Guillain–Barré syndrome, and inflammatory bowel diseases (IBD) (Nachamkin, 2002). The bacteria’s ability to evade immune defenses and sustain inflammation underpins its role in these prolonged disorders. Persistent inflammation following C. jejuni infection complicates clinical outcomes, resulting in significant long-term health consequences.
C. jejuni initiates a robust pro-inflammatory response by colonizing the intestinal mucus layer, leading to cytokine and chemokine production and, ultimately, diarrhea. Central to this process is the ALPK1 pathway, which mediates NF-κB-dependent inflammation independently of classical Toll-like and Nod-like receptors. Key virulence factors, such as adenosine diphosphate-heptose and related heptose phosphates, drive this pathway, highlighting unique interactions with host immunity (Cui et al., 2021).
The immune response involves a dynamic interplay of cytokines. Pro-inflammatory mediators like TNF-α, IL (Interleukin)-6, and IL-8 initiate inflammation, while IL-1β, IL-12, and IL-23 further activate immunity. In contrast, anti-inflammatory cytokines such as IL-4 and IL-10 help resolve inflammation. Understanding these cytokine dynamics is crucial for developing targeted therapies (Al-Banna et al., 2018).
Another pathogenic mechanism involves bacterial sirtuins. C. jejuni secretes a sirtuin that deacetylates host histones, promoting neutrophil activation and extracellular trap formation. Mice infected with sirtuin-deficient mutants exhibit reduced inflammation, underscoring the protein’s role in disease (Callahan et al., 2023).
Beyond gastrointestinal symptoms, C. jejuni infection can cause chronic sequelae like reactive arthritis and Guillain–Barré syndrome, the latter resulting from immune-mediated nerve damage (Nachamkin, 2002). The persistent inflammatory response thus links acute infection to long-term neurological and autoimmune complications.
IL-23 is particularly significant in C. jejuni-induced intestinal inflammation, promoting IL-17 and IFN-γ production by innate lymphoid cells. Mice lacking IL-23 show reduced pathology, suggesting that IL-23 is a promising therapeutic target (Jing et al., 2021).
Nutritional interventions, such as human milk oligosaccharides like 2′-fucosyllactose (2′-FL), can modulate inflammation. Studies show that 2′-FL inhibits bacterial invasion and suppresses pro-inflammatory cytokine release, indicating its potential as a preventive or therapeutic agent (Yu et al., 2016).
Infants are particularly vulnerable, especially in low-income countries, where C. jejuni is a major cause of diarrhea and is linked to growth faltering and cognitive delays. Chronic inflammation can lead to malabsorption and developmental issues, highlighting the need for effective interventions (Schnee and Petri, 2017).
At the cellular level, C. jejuni activates both pro- and anti-inflammatory pathways in intestinal epithelial cells via PI3K/Akt signaling, suggesting complex immune modulation that may facilitate bacterial persistence (Li et al., 2023).
Toll-like receptors (TLRs) are central to the host response. TLR4 is critical for inflammation, while TLR2 maintains mucosal integrity, emphasizing the importance of TLR signaling in controlling infection (Stahl et al., 2014).
Finally, C. jejuni infections may contribute to IBD development or exacerbation by disrupting intestinal barrier function and promoting chronic inflammation, particularly in susceptible individuals (Kalischuk and Buret, 2010).
Mechanisms of C. jejuni in tumorigenesis: A complex interplay of bacterial virulence and host immune responses
C. jejuni contributes to tumorigenesis through several interconnected mechanisms, prominently involving the production of CDT, its delivery via extracellular vesicles (EVs), and the modulation of host immune responses. These processes reflect a sophisticated interplay between bacterial virulence factors and host cellular pathways, highlighting the bacterium’s significant role in promoting colorectal cancer (CRC).
CDT is central to the tumorigenic potential of C. jejuni. This genotoxin exhibits DNase activity, causing DNA double-strand breaks—an event critical for colorectal tumorigenesis (He et al., 2019). Experimental studies using germ-free ApcMin/+ mice have demonstrated that colonization with CDT-producing C. jejuni results in significantly increased tumor number and size compared with uninfected controls. The cdtB subunit is essential for this effect; its mutation diminishes both tumorigenesis and DNA damage responses in cells and enteroids (He et al., 2019), underscoring the pivotal role of CDT and its subunits in cancer development.
Beyond its free form, CDT is also delivered to host cells via EVs, which are vital for efficient toxin transfer. These vesicles bind to host cell glycans, inducing cell cycle arrest and contributing to tumorigenesis (Le et al., 2024). The EV-associated CDT is shielded within membrane blebs, facilitating cellular uptake independent of surface proteins. Glycan array studies reveal that EVs share receptor-binding specificities with C. jejuni for fucosyl GM1 ganglioside, P1 blood group antigen, sialyl, and sulfated Lewisx, illustrating complex host–pathogen interactions (Le et al., 2024).
Upon internalization, C. jejuni triggers a multifaceted host response, characterized by the upregulation of genes involved in transcription, signal transduction, apoptosis, and immune modulation. This response reflects a delicate balance between cell survival and death, with implications for postinfectious pathology. Notably, genes linked to tumorigenesis, such as TLR3 and CD36, are upregulated following infection, suggesting a direct connection between C. jejuni and cancer initiation (Steinbach et al., 2024).
C. jejuni infection also alters neutrophil function, inducing a subtype with cancer-promoting properties. These neutrophils display delayed apoptosis and heightened reactive oxygen species production, both of which can foster colorectal tumorigenesis. Their interactions with T cells and colonocytes can upregulate pro-tumorigenic genes, further linking infection to cancer progression (Dolislager et al., 2022).
In addition, C. jejuni manipulates regulatory networks of microRNAs (miRNAs) and their target genes. These miRNAs are crucial in mediating bacterial invasion and modulating host immune responses, thereby influencing the expression of tumorigenesis-related genes. Interactions between miRNAs and targets such as BCL9 and IL4R exemplify the intricate molecular mechanisms by which C. jejuni may promote cancer (Wang et al., 2018).
Dendritic cell activation is another key aspect, involving TLR4 and adaptor proteins MyD88 and TRIF. This leads to the secretion of pro-inflammatory cytokines and the priming of Th1 immune responses, which, while essential for pathogen defense, can also contribute to inflammation-associated tumorigenesis (Rathinam et al., 2009). The dual role of dendritic cells in both immune protection and tumor progression underscores the importance of immune balance in preventing cancer.
The prevalence of C. jejuni in poultry and food sources represents a major public health concern, as contaminated poultry is the primary reservoir for human infection (Humphrey et al., 2007; Painter et al., 2013). The emergence of antibiotic-resistant strains, particularly in poultry slaughterhouses (Szczepanska et al., 2017), complicates infection management. MDR infections are increasingly reported, especially in immunocompromised individuals, necessitating effective treatment strategies, such as carbapenem therapy in severe cases (Montgomery et al., 2018; Du et al., 2018; Youh et al., 2021; Rasschaert et al., 2020; Jorgensen et al., 2002).
In summary, the mechanisms by which C. jejuni promotes tumorigenesis are multifaceted, involving CDT production, EV-mediated toxin delivery, immune modulation, and complex molecular interactions. Understanding these pathways is crucial for developing effective preventive and therapeutic strategies against C. jejuni-associated cancers. Recent advances in microbiome research and antibiotic resistance highlight the urgent need for comprehensive approaches to mitigate the health impact of this pathogen.
Clinical and epidemiological evidence of C. jejuni
C. jejuni is increasingly implicated in chronic gastrointestinal inflammation and malignancies, supported by clinical and epidemiological data. Persistent infections are linked to chronic inflammation, a known risk factor for colorectal and gastric cancers. Individuals with chronic gastrointestinal disorders like IBD frequently exhibit persistent C. jejuni infections, accompanied by elevated pro-inflammatory cytokines such as IL-1β and TNF-α, which may drive tumorigenesis when combined with genetic or microbial cofactors (Young et al., 2002). Cohort analyses highlight enriched Campylobacter in CRC samples, suggesting a potential carcinogenic role, though prospective studies remain limited (Nhung et al., 2024).
Epidemiological studies correlate higher C. jejuni exposure with increased colorectal and gastric cancer rates, particularly in regions with endemic infections, implying a dose–response relationship (Poosari et al., 2021). The bacterium’s genotoxin, CDT, induces DNA double-strand breaks, activating carcinogenic pathways—a mechanism validated in germ-free ApcMin/+ mice, where CDT-producing strains drive tumorigenesis, while cdtB mutants attenuate DNA damage and tumor growth (He et al., 2019). Developing nations with high C. jejuni exposure report rising gastric and CRC incidences, exacerbated by virulent, antibiotic-resistant strains in food sources like poultry (Coker et al., 2002).
Experimental models reinforce these findings. Chronic C. jejuni exposure in IL-10-deficient mice promotes tumorigenic environments via mTOR (Mechanistic Target of Rapamycin) and NF-κB (Nuclear Factor-kappa B) activation (Sun et al., 2012). In vitro studies using intestinal epithelial cells (e.g., HT-29, Caco-2) demonstrate disrupted tight junctions, increased permeability, and oxidative stress—key contributors to inflammation and carcinogenesis (Ong et al., 2023). Infection also triggers TLR4dependent chemokines like IL-8 and MCP-1 (Monocyte Chemoattractant Protein-1), sustaining pro-inflammatory microenvironments (Otto et al., 2012).
Collectively, this evidence underscores the need for public health strategies to mitigate persistent C. jejuni infections, emphasizing improved diagnostics, food safety, and targeted therapies to disrupt inflammation-driven carcinogenesis.
Challenges and research gaps in understanding the role of C. jejuni in tumorigenesis
The role of C. jejuni in tumorigenesis remains incompletely understood due to several persistent challenges, including difficulties in establishing causality, considerable strain-specific variability, and the intricate interplay of host and environmental factors. Although chronic inflammation induced by C. jejuni is a recognized risk factor for cancer, the exact mechanisms connecting infection to carcinogenesis are still not fully elucidated. Establishing direct causal links between bacterial infection and tumorigenesis is particularly challenging, as most evidence demonstrates associations rather than mechanistic pathways; for example, while CDT production is implicated in DNA damage, it is still unclear if this alone initiates carcinogenesis within the context of complex host–microbiota interactions (He et al., 2019). Recent findings that C. jejuni EVs carrying CDT can bind host cell glycans and induce cell cycle arrest suggest a possible mechanism for tumorigenesis (Le et al., 2024).
There is a critical need to clarify how bacterial factors interact with host determinants to drive tumorigenesis. The unfolded protein response in host cells has emerged as a key mediator in C. jejuni pathogenesis, potentially influencing bacterial survival and immune evasion. Small RNAs like CjNC110, which regulate the activated methyl cycle, are essential for optimal colonization, illustrating the complexity of pathogenic mechanisms. The lack of robust longitudinal studies further limits understanding, as most available data are cross-sectional and do not capture the progression from infection to chronic disease or cancer. Without large, representative cohorts followed over time, the contributions of immune response, microbiota composition, and genetic predisposition to cancer risk after C. jejuni infection remain uncertain (National Academies of Sciences, Engineering, and Medicine, 2006).
Unresolved questions persist regarding the host and environmental factors that modulate the risk of tumorigenesis after infection. The influence of diet, immune status, and coinfections on the inflammatory response to C. jejuni is poorly understood. Comparisons with Helicobacter pylori, which shares structural and pathogenic features with C. jejuni, highlight both similarities and key differences. H. pylori is a well-established cause of gastric cancer, largely due to the CagA toxin, whereas C. jejuni is primarily linked to gastroenteritis and neurological complications, with emerging evidence for a role in chronic intestinal inflammation and CRC (Kelly, 2001; Butt and Epplein, 2019; Hatakeyama, 2017; Kaakoush et al., 2015). Immune dysregulation, particularly in IBD, may amplify the carcinogenic potential of chronic inflammation induced by these bacteria, and recent studies show that C. jejuni can drive neutrophil differentiation into cancer-promoting subtypes (Dolislager et al., 2022). However, the precise mechanisms by which both bacteria contribute to intestinal oncogenesis are not fully defined, emphasizing the need for further research on their impact and potential targeted therapies (Backert and Hofreuter, 2013).
Strain variability represents another major research gap. Some C. jejuni strains produce high CDT levels, while others do not, and clinical outcomes differ accordingly. Comparative genomic and proteomic studies are needed to determine why certain strains are more associated with severe inflammation and carcinogenesis (Hu and Hickey, 2005). The genetic diversity and antibiotic resistance profiles of C. jejuni isolates, especially from poultry, further complicate this picture and highlight the importance of understanding strain-specific variations (Jeong et al., 2025). Differences in host–pathogen interactions between humans and animal models add to the challenge of generalizing findings.
Addressing these gaps requires integrative research strategies. Longitudinal studies should be prioritized to establish causal relationships and long-term outcomes of infection. Experimental animal and in vitro studies should dissect host–microbiota–pathogen interactions and the specific pathways leading to tumorigenesis. Advances in molecular biology and genomics provide opportunities to explore strain-specific differences and their implications for infection outcomes. Investigating genetic factors, such as immune signaling polymorphisms, may reveal individual susceptibilities to cancer following infection. Standardized infection models and high-throughput sequencing could clarify the roles of specific virulence factors in promoting chronic inflammation and cancer.
A comprehensive approach is essential for advancing understanding of C. jejuni in tumorigenesis and improving public health strategies. The rise of AMR in C. jejuni complicates treatment and underscores the need for ongoing surveillance and research (Jeong et al., 2025). Further studies are needed to elucidate the mechanisms by which C. jejuni contributes to cancer, building on insights into bacterial pathogenesis and host immune interactions (National Academies of Sciences, Engineering, and Medicine, 2006). Innovative approaches, such as multiepitope vaccine development, could offer new preventive strategies (Saravanan and Mohan, 2024).
Future perspectives in understanding and managing C. jejuni-associated pathologies
Addressing C. jejuni-linked pathologies requires integrating advanced research models, microbiome insights, and clinical innovations. Current experimental models, such as germ-free and IL-10-deficient mice, provide foundational insights but lack human physiological complexity. Developing “humanized” mouse models with human microbiota and immune components could better replicate host–pathogen dynamics, particularly when incorporating environmental cofactors like diet and coinfections. Recent advancements using OligoMM12 gnotobiotic mice demonstrate robust colonization and pathogen-specific metabolite signatures, offering new avenues to study host responses (Sun et al., 2012; Kang et al., 2025).
The gut microbiota’s role in modulating C. jejuni pathogenicity is critical. Dysbiosis exacerbates bacterial persistence and inflammation, necessitating studies on microbial taxa interactions and environmental influences like antibiotics or diet (Bereswill et al., 2011; Schnee and Petri, 2017). Probiotic and enzyme-based interventions reducing C. jejuni shedding in poultry suggest translatable strategies for humans (Gibbs et al., 2021).
Clinically, preventing chronic infections through vaccines targeting virulence factors (e.g., flagella, CDT) and enhancing food safety protocols could reduce long-term risks (Altekruse et al., 1999). Identifying high-risk patients via biomarkers, such as immune pathway polymorphisms (e.g., IL-10, TLR4), may enable personalized interventions (Otto et al., 2012). Emerging therapies, including CDT-neutralizing agents and microbiota-modulating treatments, show promise in mitigating genotoxicity and inflammation (He et al., 2019). Small-molecule inhibitors targeting adhesion mechanisms or two-component regulatory systems could disrupt infection cycles (García-Sánchez et al., 2024).
Recent discoveries highlight bacterial components like the ChuABCD heme transport system as vital for colonization, offering novel intervention targets (Randaisi et al., 2025). Similarly, C. jejuni bacterial ghosts inducing IL-6/IFN-γ responses in mice underscore potential immunotherapeutic strategies (Al-Mansoori & Al-Yassari, 2024).
A multidisciplinary approach-combining refined models, microbiome modulation, targeted therapies, and precision diagnostics will be essential to reduce the global burden of C. jejuni-associated diseases. Prioritizing longitudinal studies and translational research will bridge gaps between mechanistic insights and clinical applications, ultimately improving outcomes for at-risk populations.
Conclusion
The dual identity of C. jejuni—as both a pathogen and a potential instigator of tumorigenesis—unveils a captivating narrative at the crossroads of microbiology and oncology. Traditionally recognized for its role in acute gastroenteritis, C. jejuni is now emerging as a significant contributor to chronic inflammation, immune dysregulation, and genetic instability, all of which may culminate in gastrointestinal cancers. This paradigm shift challenges established perceptions and underscores the profound impact of persistent bacterial infections on long-term health.
As research delves deeper into the molecular intricacies of C. jejuni’s interaction with its host, the bacterium reveals itself not merely as an infectious agent but as a potential architect of cancer. By orchestrating inflammatory cascades and inducing genetic damage, C. jejuni epitomizes how microbial pathogens can reshape the delicate balance between health and disease. Its multifaceted role—shaped by genetic diversity, host immune dynamics, and environmental factors—positions it as a compelling model for understanding bacterial contributions to carcinogenesis.
These findings herald an urgent call to action for future research aimed at unraveling the complex interplay between C. jejuni infection and cancer development. Advancing our understanding could revolutionize strategies for early detection, prevention, and treatment. From identifying biomarkers to developing vaccines and targeted therapies, these efforts hold transformative potential for public health. Moreover, integrating preventive measures such as enhanced food safety protocols and public awareness campaigns could significantly mitigate the global burden of C. jejuni-related diseases.
The time to act is now. By exploring the full scope of this pathogen’s influence, we not only gain insights into combating infection but also unlock opportunities to prevent cancer—reshaping the future of gastrointestinal health on a global scale.
Authors’ Contributions
Z.A. and M.M. jointly led the conceptualization and design of the study, conducted the in-depth literature review, and were primarily responsible for drafting and revising the article. L.C. contributed to the organization of the article structure and assisted in synthesizing thematic content. M.Y. and C.H.F. supported data organization, reference formatting, and contributed to language editing and final proofreading. D.I. participated in reviewing selected sources and provided input on the article’s structure.
Footnotes
Funding Information
No funding was received for this article.
Disclosure Statement
The authors declare that there are no financial, personal, or professional conflicts of interest related to the content of this article.