
Abstract
Objective:
Evaluation of the effects of exergames in women with fibromyalgia on the impact of the disease—pain threshold and physical variables—compared to performing stretching exercises.
Materials and Methods:
Thirty-five women were enrolled in the study and divided by simple randomization into two treatment groups: the control group (n = 19) and the Wii™ (exergames) group (n = 16). Participants were evaluated using the fibromyalgia impact questionnaire (FIQ), algometry, step tests, cardiopulmonary parameters, and fatigue in the lower limbs. The participants underwent treatments for a period of 7 weeks with three 1-hour sessions weekly and were reevaluated after the 10th and the 20th sessions.
Results:
The exergames group showed significant reduction of their fibromyalgia symptoms, as demonstrated by lower FIQ scores in the key domains on questions regarding missed work, pain, fatigue, problems resting, stiffness, anxiety, and depression. Significant improvements were observed in mean algometric values in the cervical region, the second chondrocostal junction, the lateral epicondyle, left medial knee border, left occipital region, trapezius, supraspinatus, gluteal muscles, and the greater trochanter. Improved cardiovascular adaptation was reflected by decreased systolic blood pressure, reduction in fatigue of the lower limbs assessed by the CR10 Borg scale, and improved exercise capacity assessed by a step test.
Conclusion:
Exergames have the potential to increase exercise capacity, decrease the impact of fibromyalgia, promote cardiovascular adaptation, reduce fatigue of lower limbs, and improve the pain threshold in women with fibromyalgia.
Introduction
Fibromyalgia is one of a subgroup of chronic widespread pain disorders. 1 Its most frequent symptoms include severe fatigue, nonrestorative rest, cognitive difficulties, depressive mood, lower abdominal cramps, and headache.2,3 It is clear from the literature that the practice of physical activities, such as aerobic exercises, muscle strengthening, 4 aquatic exercises,5,6 aquatic bio dance, and stretching, 6 results in positive outcomes for patients with fibromyalgia.7,8
Exergames are digital games that simulate the practice of physical exercises. They replicate movements used in physical rehabilitation. This technique has been utilized for the treatment of various movement disturbances, including cerebral palsy 9 and hemiparesis. 10 It is also useful in postoperative rehabilitation following total knee arthroplasty, 11 for improvement of postural and balance control in the elderly, 12 for vestibular rehabilitation, 13 and to improve quality of life and reduce fatigue in cancer patients.14,15
Recent studies have reported the effects of exergames on women diagnosed with fibromyalgia, achieving additional benefits, such as pain reduction,16,17 decreased overall severity of fibromyalgia symptoms, 18 improvement of perceived health status, 16 improvement of daily living activities, 19 increased cerebral blood flow, 20 and improvements in mobility skills, balance, and fear of falling. 21 However, most previous studies compared exergaming to a control group (CG) not performing any type of activity.16,17 While it has been shown that individualized exercise, including land- or water-based aerobics, strength training, yoga, and stretching activities, is effective in improving physical function for patients with fibromyalgia, 22 the effectiveness of exergames to achieve similar results remains unknown.
Therefore, the aim of this study was to examine systematically the effectiveness of exergames on pain threshold and modifiable physical variables, and the impact of fibromyalgia on the quality of life of women with the disease compared to a control group that performed stretching exercises.
Materials and Methods
Participants
This study was conducted in the Laboratory of Movement Analysis of the Department of Physiotherapy, Federal University of Alfenas, in Alfenas, Minas Gerais, Brazil. It was a randomized, single-blind clinical trial conducted between November 2012 and December 2013. To ensure blinding, the researcher who performed the various result evaluations was not the same as the examiner who applied the interventions. Of 76 women with a diagnosis of fibromyalgia who were screened, 41 did not meet the inclusion criteria and were ineligible. The criteria included a minimum age of 18 years and a diagnosis of fibromyalgia in accordance with the parameters of the American College of Rheumatology (ACR). The diagnosis requires a history of widespread pain (i.e., in ≥7 regions), at least moderate severity (a score ≥5) of pain, fatigue, sleep disruption, and cognitive symptoms, duration of symptoms ≥3 months, and absence of another disorder that could explain the condition. Criteria are also satisfied if only three to six regions are affected by pain, but the symptoms are more severe (a score ≥9).1–23
Volunteers were also withdrawn based on the exclusion criteria: cardiovascular, pulmonary, orthopedic, neurological, or dermatological conditions, which negatively affect muscle strength and physical capabilities 18 and pregnancy. 19 Men were excluded to avoid a heterogeneous sample and due to low prevalence. 24 The remaining 35 volunteers participated in the treatment over a 7-week period and were reassessed after the 10th and 20th treatment sessions (Fig. 1).
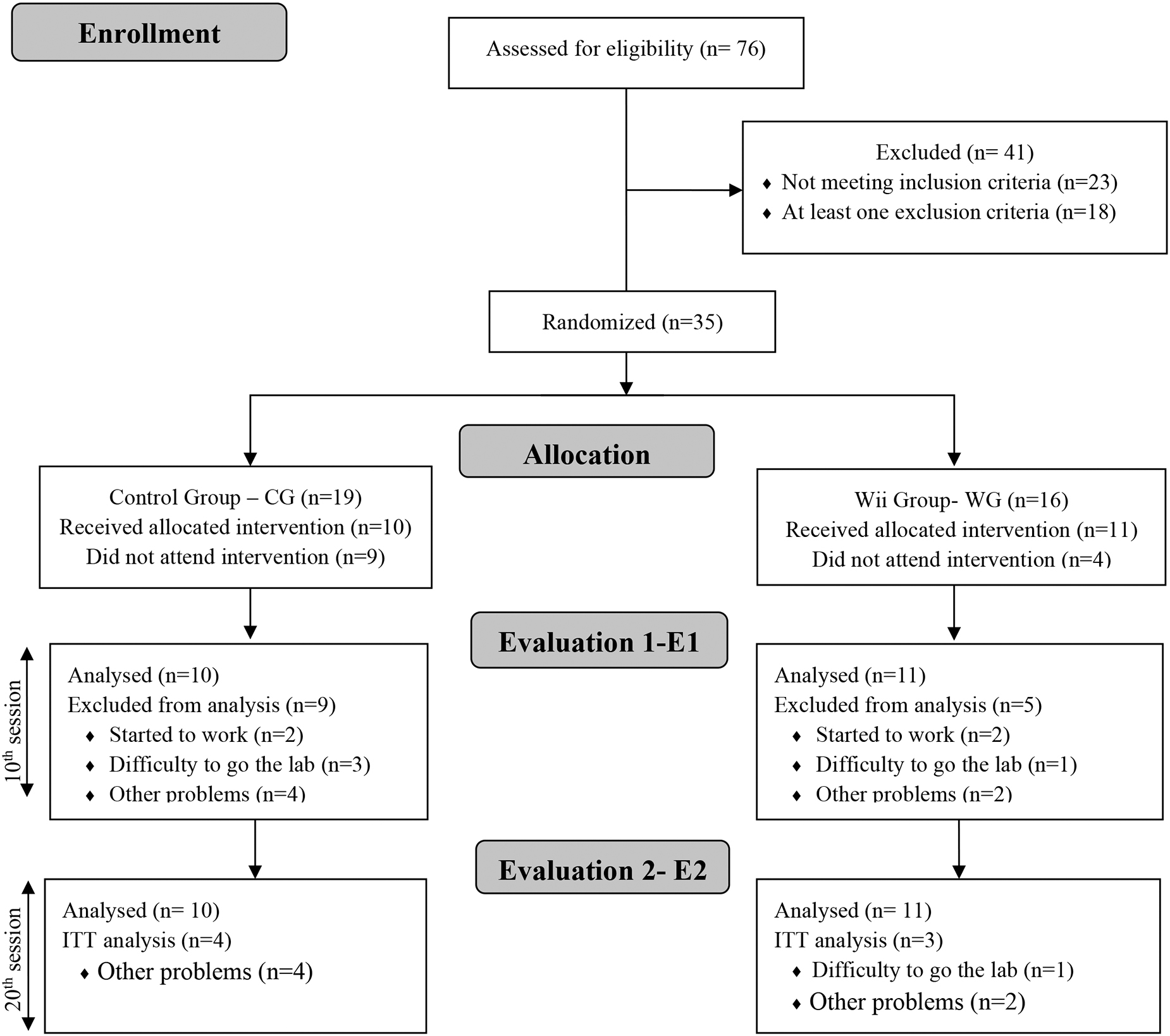
Study design. CONSORT diagram.
The volunteers received information regarding their participation in this research study and signed free and informed consent agreements. This project was approved by the Ethics and Research Committee for studies involving human subjects of UNIFAL-MG (113.376) in accordance with the Helsinki Declaration, and is recorded in the Brazilian Clinical Trial Registry—RBR-4pmzpq.
Procedure
The 35 participants underwent simple randomization using the Microsoft Office Excel application (version 2010). This program allowed the randomization of volunteers into the CG (n = 19) and the Wii™ group (WG; n = 16). Before beginning interventions with either group, the participants were evaluated using the fibromyalgia impact questionnaire (FIQ), their pain thresholds (algometry), and their exercise capacity. This baseline evaluation was labeled E0. The assessments were repeated after the 10th (E1) and 20th sessions (E2).
The FIQ is designed to measure the status, progress, and results of treatment in patients with fibromyalgia. 25 It has been translated to Portuguese, adapted for cross-cultural use, and validated. 26
Pain threshold was evaluated using a digital algometer (EMG Electromyography System of Brazil). The contact point of this algometer has a diameter of 10 mm. The evaluation was performed by the same examiner whenever possible, who tested the 18 designated tender points. 23 The device was applied to the 18 sites in a gradual and constant manner until the moment the subject reported pain.
In addition to widespread pain, fibromyalgia causes a decline in physical fitness, which affects women's lives dramatically. 27 From this observation, it has been proposed that multiple tests are required for evaluating fitness in this population. One option is the 6-minute walk test. 27 In this study, a step with a height of 25 cm was used; physical performance was determined by climbing and descending the step. The volunteers were encouraged to perform movements using standardized verbal commands that were predetermined. 28
The symptoms of lower-limb fatigue were evaluated using the Borg CR10 Scale, while the PsO2 (peripheral oxygen saturation) and heart rate (HR) were measured using a pulse oximeter (Linde MD 300). Systolic blood pressure (SBP) and diastolic blood pressure were measured in the standard way using a sphygmomanometer. The respiratory rate was recorded at rest, during the exercise (2nd, 4th, and 6th minutes), immediately after the test, and in the 1st, 3rd, and 6th minutes of the recovery period (7, 9, and 20 minutes). 29
Control group
The control group performed the chain muscle stretching technique thrice per week with each session lasting 1 hour. Chain muscle stretching has been used in the treatment of fibromyalgia.6,7 This schedule was followed for the 7 weeks of the study. The positions were held during four deep and prolonged expirations. Exercises were chosen to include standing, sitting, and lying positions (Fig. 2). In addition, they were chosen to engage all muscle groups in a global manner. The following positions were selected: 1, 15, 16, 19, 21, 35, 36, 38, and 40. 30
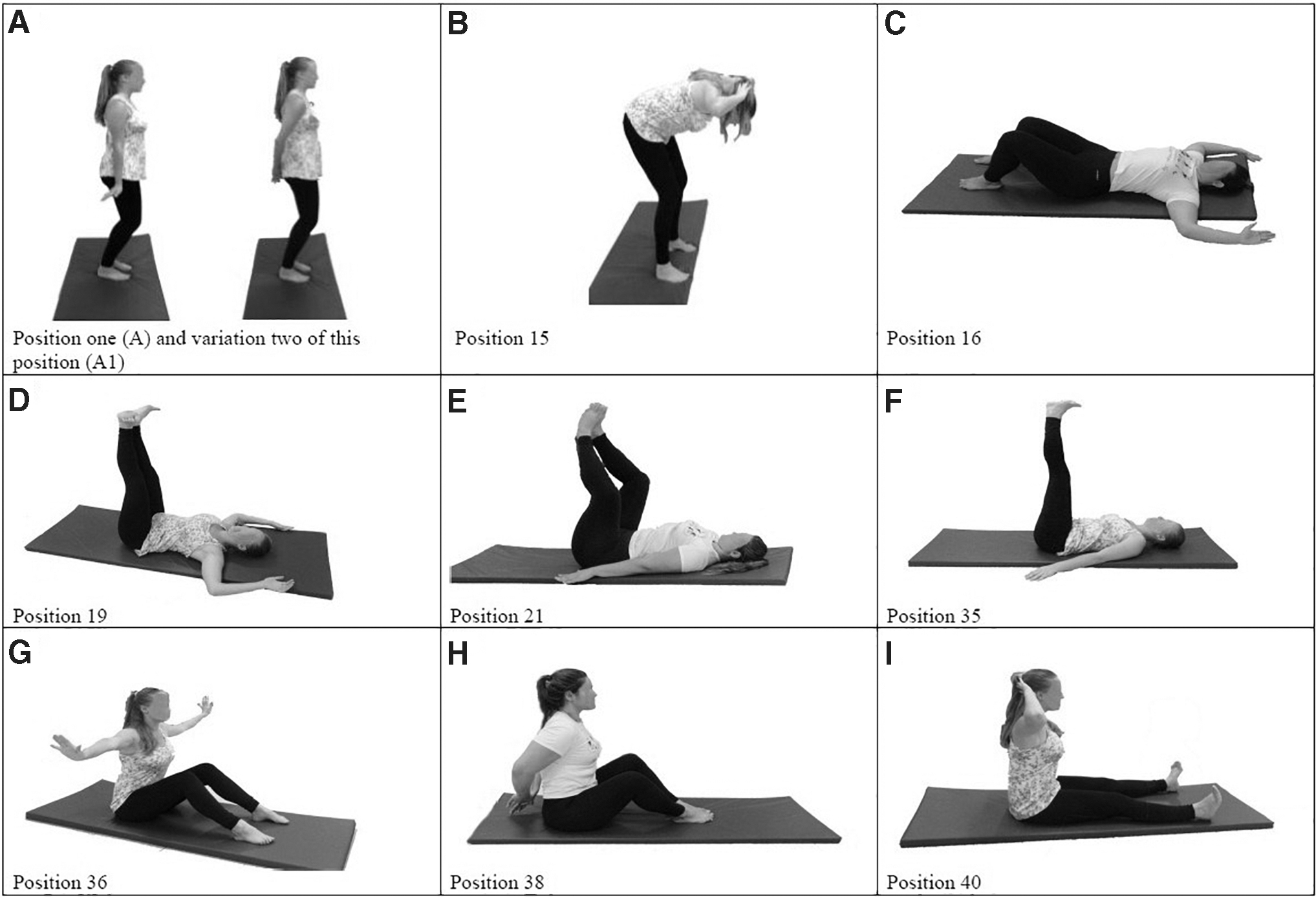
Stretching technique positions. A1 is the variation of Position one.
Position 1: orthostatic position, feet parallel, semiflexion of the knees, pelvic retroversion, arms outstretched and slightly backward, wrists and fingers flexed in extension, gluteal muscles contracted, scapular adduction, and erect spine (Fig. 2A). Variation 2 of this position, which is performed with the hands in contact, was also used (Fig. 2A1).
Position 15: standing position, anterior trunk inclination, knees flexed, and arms flexed with the hands supported on the back of the head (Fig. 2B).
Position 16: dorsal decubitus position, legs flexed, feet on the floor, and arms crossed (Fig. 2C). 30
Position 19: dorsal decubitus position, lower limbs in hip flexion at 90° and knees in extension, shoulders and elbows in 90° flexion, foot dorsiflexion, and scapular adduction (Fig. 2D).
Position 21: dorsal decubitus position, knees and hips semiflexed vertically and in external rotation, the soles of the feet in contact, and the arms positioned along the sides of the body (Fig. 2E). 30
Position 35: dorsal decubitus position, arms in extension and slight abduction, and legs extended at 90° (Fig. 2F).
Position 36: seated position, erect spine, lower limbs semiflexed, feet supported on the floor, horizontal abduction and extension of the arms, and wrist extension at 90° (Fig. 2G).
Position 38: seated position, erect spine, lower limbs semiflexed, feet supported on the floor, upper limbs in extension behind the body, and hands in contact with one another (Fig. 2H).
Position 40: seated position, shoulder abduction, and hands positioned behind the head (Fig. 2I). 30
Exergames
The exergames group performed the program thrice per week with each session lasting 1 hour. Before beginning the intervention, participants were instructed and trained to play the games and handle the game console.
The Nintendo® Wii system (Nintendo, Kyoto, Japan), linked with a 42-inch LED TV, a Wii remote plus, and a Wii balance board were used for this treatment. Six subgames of Wii Fit Plus were chosen for this group. These included Jogging Plus, an activity in which the subjects perform stationary running. It results in active and constant movement of the lower limb muscles for 15 minutes. The “Bird's-eye Bull's-eye game” was performed for 9 minutes. It is a game that requires active movement of the upper limbs in isolation from weight and balance training. The “Yoga game” was used for 3 minutes. It stimulates not just control of expiratory and inspiratory movements but also active control of the body's center of gravity. The “Super Hula Hoop game” was performed for 9 minutes. It requires the action of the trunk muscles associated with circular rhythmic movements as well as balance control. A “Step game” was used for 15 minutes and consists of active and alternating movements of the lower limb muscles, as well as balance and unipodal discharge. Finally, “Rhythm Parade” was performed for 9 minutes. It consists of stationary walking associated with active and rhythmic movements of the lower limb muscles.
Statistical analysis
The collected data were analyzed with the SPSS software 20.00 (Chicago, IL) considering the significance level at 0.05.
For the calculation of the sample n, the variable physical function by FIQ was used, with a sample size of 16 volunteers as estimated for a power of 80%. The initial data were evaluated with ANOVA test and sample size was calculated using G* Power software, v. 3.1.7 (Franz Faul, Universität Kiel, Germany), with parameters: F tests→ANOVA: Repeated measures, with factors→Effect size f estimated from variances. The normality of the data was verified using the Kolmogorov–Smirnov test and its homoscedasticity (equality of variance) by the Levene test. The variable anthropometric data and time of pain symptom were submitted to the Mann–Whitney U test.
Data from all 21 initial participants who underwent treatment since the beginning of the study were used to conduct the intention-to-treat by multiple imputation analysis.
The analysis of variance (repeated two-way ANOVA measures), followed by the Bonferroni post-test for multiple comparisons, was used when the data presented normal distribution. In addition, we used Mauchly's test of Sphericity and, in case of violation of this assumption, a Greenhouse Geisser correction was performed.
To calculate the effect size in ANOVA, f2 Cohen was used, and values from 0.02 to 0.15 (small effect), 0.15 to 0.35 (moderate effect), and above 0.35 (large effect) were adopted. 31
Results
A total of 76 volunteers were assessed for eligibility. Forty-one were excluded for the following reasons: not meeting inclusion criteria (n = 23) and having at least one of the exclusion criteria (n = 18). The remaining patients (n = 35) were allocated into the Wii group (n = 16) or the control group (n = 19) using the simple random sampling method. Of the nine control group participants who quit the program, two did so because their work schedule was not compatible with the exercise schedule, three due to transportation difficulty, and four from other problems (E1). Five participants were lost from the Wii group because they started a job (n = 2), had transportation difficulty (n = 1), and other problems (n = 2) preventing them from completing the 10 sessions. To account for the dropouts from both groups, we conducted an intention-to-treat analysis by replacing missing values in the 20th session with each patient's previous score (Fig. 1).
The groups were found to be similar in demographic data and duration of symptoms (Table 1).
Sample Characterization [Mean (Standard Deviation)] and Comparison of Anthropometric Data and Time of Pain Symptom
Mann–Whitney U test.
CG, control group; BMI, body mass index; WG, Wii™ group.
The analysis of the FIQs demonstrated that both groups were similar at the beginning of the study (E0) in relationship to symptoms and the impact of fibromyalgia on their lives.
Significant intragroup improvements were found in the Wii group for several factors, including “not feeling good,” “missed work,” “severity of pain,” “fatigue,” “unable to feel rested,” “stiffness,” “anxiety,” “depression,” and FIQ total score after 10 and 20 sessions. Intergroup variation analyses also revealed significant drops in FIQ total scores, increases in “feeling good,” and decreases in “fatigue,” “anxiety,” and “depression” in the Wii group after 10 and 20 sessions. There was an improvement in the parameters of “missed work,” “pain,” and “rested” after 10 sessions, whereas improvement in “stiffness” was noted only after 20 sessions. The “physical function” and “doing my job” factors showed no change following the intervention in the exergaming group. The magnitude of the effects was high for all evaluated variables, except “doing my job,” which was moderate (Table 2).
Evaluation of the Domains and Total Scores of the Fibromyalgia Impact Questionnaire
Three evaluation times: Baseline (E0), after 10 sessions (E1), and after 20 sessions (E2).
Bonferroni test: aWG versus CG and A versus B P < 0.05; effect size (f 2 ).
L, left; R, right; SD, standard deviation.
Before treatment (E0), the pain threshold analysis was similar in both groups. After 10 sessions (E1) and 20 sessions (E2), the pain threshold had increased, which indicates an improvement in pain levels. In the intragroup analysis, the WG showed bilateral improvement in several areas, including in the cervical C7 region, the second chondrocostal junction, the lateral epicondyle, the trapezius and gluteal muscles, the supraspinatus, and the greater trochanter. For the occipital and medial knee border regions, only the left side's pain threshold increased.
In contrast, in the CG, the pain threshold improved only in the medial knee border and gluteus on both sides, in cervical C7, second chondrocostal junction, and supraspinatus only on the right side, and the occipital only on the left side (Table 3).
Pain Threshold (kgf) in the Four Quadrants of the Body
Three evaluation times: Baseline (E0), after 10 sessions (E1), and after 20 sessions (E2).
Bonferroni test: aWG versus CG and A versus B P < 0.05; effect size (f 2 ).
In the intergroup analysis, an increase in the pain threshold for the left lateral epicondyle and right trapezius was observed after 10 and 20 sessions of exergames. It was observed that the pain threshold level improved in the Wii group only on the left side at cervical C7, but the CG obtained a better result, compared to those performing exergaming, in pain threshold for the left medial knee border after 10 sessions. There was no significant improvement in the pain threshold of the right occipital region after 10 sessions and 20 sessions (Table 3).
The level of effect was high for almost all regions evaluated, except cervical C7 and second chondrocostal on both sides, and the left lateral epicondyle, which reported a moderate effect (Table 3).
Initially, the groups were similar in all items evaluated according to the physical fitness test. The results of the evaluations indicated that the WG showed improvement in physical performance by increasing the total number of steps climbed (E1–E2), less fatigue in the lower limbs during 6 minutes of activity (E1–E2), and increased HR (9 minutes). The CG showed a significant decrease in fatigue in the lower limbs at the beginning of the evaluation (2 minutes) and at the end (6 minutes), but the reduction was more significant in the WG after 10 sessions than in the CG.
The WG showed a significant decrease in SBP in recovery time (12 minutes), suggesting cardiovascular adaptations after 10 sessions. Likewise, an insignificant trend toward reduced systolic pressure can be observed in the initial (0 minutes) and recovery (12 minutes) moments after 10 and 20 exergaming sessions (Table 4).
Evaluation of the Physical Capacity and Cardiopulmonary
Three evaluation times: Baseline (E0), after 10 sessions (E1), and after 20 sessions (E2).
Bonferroni test: aWG versus CG and A versus B P < 0.05; effect size (f 2 ).
CR10, Borg CR10 Scale; DPA, diastolic blood pressure; HR, heart rate; PsO2, peripheral oxygen saturation; RR, respiratory rate; SPA, systolic blood pressure.
The effect size was large in almost all the parameters evaluated, except CR10 at 2 minutes, which was moderate (Table 4).
Discussion
The data in this study suggest that the exergames are useful for the treatment of fibromyalgia symptoms. The main finding of this trial was that intervention based on exergames significantly reduced the impact of fibromyalgia by improving the participants' perceptions of feeling good, missed work, pain, fatigue, feeling rested, stiffness, anxiety, depression, and improved pain threshold algometry measured at multiple tender points. The between-group analysis also revealed benefits in FIQ scores, in total score, and in the individual scores for the above factors, as well as improved pain threshold in the left lateral epicondyle and right-side trapezius. This therapeutic approach may improve exercise capacity and promote cardiovascular adaptations.
Physical exercise has been shown to improve symptoms of fibromyalgia, such as pain,8,16,17,32 nonrestorative rest, 33 depression, 34 anxiety,33,35 stiffness, 36 health-related quality of life, 16 and physical fitness. 21 The literature indicates that the improvement of symptoms, based on the FIQ, results in a reduction of the impact of fibromyalgia on the patients' lives.36,37 This study has similarly 17 shown benefits in the same FIQ domains, indicating a reduction in the impact of fibromyalgia on patients' lives. 20 In contrast, according to other studies, 17 the protocol of exergaming did not show significant changes in the physical function domain of the FIQ. The protocol adopted in this study was able to improve factors in the other domains, such as “missed work,” “doing my job,” and “feeling rested.” It is possible that being applied more frequently achieved better results when compared to another study. 17 It is likely that the exercise may have promoted changes in brain dynamics that could be related to increased cerebral blood flow, 21 which justifies the findings.
The practice of physical exercise is associated with a decrease in pain among the general population 38 and in people with fibromyalgia.16,17 However, with regard to pain responses, the practice of exergames is more evident in patients with higher pain thresholds. 16 In this study, volunteers with higher or lower pain thresholds were not separated, and this variable was measured by a Visual Analog Scale (VAS)—the FIQ—and algometry. Similar to the findings by Villafaina et al., 16 we observed greater pain reduction, according to the VAS (FIQ), after 20 sessions in both groups, but more pronounced in the WG for the right trapezius and left lateral epicondyle regions when evaluating the algometry, with moderate to large effect magnitude. It is likely that the nonstratification of volunteers by pain level may have favored the larger effect size findings, as volunteers with both higher and lower pain thresholds comprised the sample.
In another study of patients with fibromyalgia, it was noted that a 16-week program of continuous movement (dancing) resulted in improved sleep quality. 39 Likewise, a 10-week study of aerobic exercises and progressive relaxation techniques also resulted in improved sleep quality. 33 In our study, the practice of exergames promoted substantial improvement in the “rest” factor on the FIQ. This result was obtained in a shorter treatment period (7 weeks), suggesting that it provides benefit more quickly than dance, aerobic exercises, and relaxation techniques.
A further study reports improvements in the symptoms of depression in women with fibromyalgia, who performed exercises and participated in a 17-week educational program. 34 In another study, in which the intervention was a 16-week program of hydrokinetic therapy, the results demonstrated improvement in symptoms of depression, as measured by Beck's inventory. 40 These findings suggest that the aerobic exergames using the Nintendo Wii may improve depression in a shorter time (4 weeks). Thus, the interactive exergames and the engagement of patients with the games can directly contribute to successful treatment of the depression component of fibromyalgia, compared to other forms of exercise.
There are studies reporting improvement in certain FIQ domains. For instance, physical function has been used as a variable to evaluate the use of multidisciplinary therapy 41 and Tai Chi treatment. 42 Both obtained positive outcomes in 12 weeks of treatment. Furthermore, an improvement in anxiety symptoms, as revealed by the FIQ, was achieved with a 28-week program of Tai Chi. 37 These clinical trials required a longer period of intervention compared with this study.
In another clinical trial, it was determined that aerobic exercises resulted in more significant improvements than stretching exercises. The evaluation of the 18 tender points through palpation for pain threshold was among the variables evaluated. A pain scale was used to measure these variables after the 10th and 20th weeks of treatment. 43 In this study, it was noted that exergames produced more substantial responses compared to the control (chain muscle stretching technique).
Another study used rehabilitation exercises based on a group of therapeutic exercises that combine mobility work and body awareness. Positive outcomes were achieved, as evidenced by a reduction in the number of tender points, 44 a finding that matches this study.
In the analysis of the results from the 6-minute step test, together with the Borg scale, there was significant improvement in physical function. Once again, a short period of training was sufficient to change the variables, which has not been demonstrated in other studies. 42 These promising results from exergames may be justified by the ability of this tool to improve mobility skills 18 and physical fitness in women with fibromyalgia. 20
Although the effect of regular exercise on improvement of blood pressure readings is not yet clear, this study's data agree with previous investigations that posit that the power of a regular exercise program can decrease SBP, 45 which was observed mainly in the recovery period after exergaming in this study.
The use of exergames in rehabilitation has been steadily gaining acceptance in therapeutic plans, mainly because it can be performed at home and at a distance. At home, the variable score obtained in the game informs the progress of the treatment. In addition, the position variables of the lower and upper limbs are obtained by means of infrared sensors that detect and record the performance achieved by patients. In relationship to distance use, games can be used to maintain the gains obtained in a rehabilitation session, as well as being applied at a distance through Internet connection favors the real-time analysis of the patient at home.
Limitations of this study were that the number of sessions proved to be insufficient to promote improvement in doing my job and other physical functions. In addition, the number of volunteers is a factor that limits the statistical significance of this study.
Conclusion
In conclusion, exergames techniques have demonstrated robust results in improving the symptoms, pain threshold, exercise capacity, and cardiovascular adaptation in women with fibromyalgia. The exergames required a shorter treatment period than other types of exercise to achieve positive outcomes.
Footnotes
Acknowledgments
The authors wish to thank the patients who participated in the study and the Research Support Foundation of Minas Gerais.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by a grant from the Research Support Foundation of Minas Gerais (APQ 02794-11) and Tutorial Education Program (PET-MEC-SESU). The study was financed, in part, by the Coordination for the Improvement of Higher Education Personnel (CAPES)—Finance Code 001.