
Abstract
It is notoriously difficult to predict when death will occur. Symptoms and signs of death approaching include: day-by-day deterioration, gaunt appearance and profound weakness—the patient needs assistance with all care, and may be bed-bound; difficulty swallowing medicines; reduced intake of food and fluids and drowsiness or reduced cognition. The patient is often no longer able to co-operate with carers. This article aims to give GPs in training a framework with which to manage the last 48 hours of life for patients dying at home.
The GP curriculum and care in the last 48 hours
Statement 12 of the GP curriculum: Care of people with cancer and palliative care requires GPs in training to have a knowledge of the principles of palliative care. This should include a knowledge of the problems that patients and their families may encounter in the last 48 hours of life. In particular, GPs in training should be able to communicate effectively with patients and their families at this difficult time, and know how to use a syringe driver. This should include knowledge about which drugs are suitable for use in a syringe driver, and dose conversions for a syringe driver.
Talking about death
Death is a taboo subject and few people feel comfortable discussing it — even though it is natural, certain and happening all around us all the time. Opening up discussion can be very liberating to patients who then may feel they are being given permission to talk about dying. Families do not like discussions about dying for fear that patients will ‘give up’.
Sometimes the direct question ‘Are you worried about dying?’ is the most appropriate. Often patients' biggest fears are groundless and reassurance can be given (Boxes 1 and 2). Where reassurance cannot be given, it is helpful to break the fear down into constituent parts and try to sort out those aspects that you can deal with.
Avoid the trap of predicting or making a guess when death will occur unless absolutely pushed to do so. Talk in terms of ‘days’ or ‘weeks’. For example: ‘When we see someone deteriorating from week to week we are often talking in terms of weeks; when that deterioration is from day to day then we are usually talking in terms of days, but everyone is different’.
Goals of care
The goals of care in the last 48 hours of life are to ensure that patients are comfortable—physically, emotionally and spiritually, and make the end of life peaceful and dignified. Dying is a unique and special event for each individual. Helping to explore a patient's wishes about death and dying should not be a discussion left to the last 48 hours. What is dignified for one patient may not be for another, ask patients and carers what they would like well in advance. Support patients and carers so that the experience of death for those left behind is as positive as it can be.

Common fears about death and dying
Fears associated with symptoms, for example the pain will escalate to agony; breathing will stop if the patient falls asleep
Emotional fears, for example increasing dependence on family. ‘It would be better if I was out of the way’.
Past experience, for example past contact with patients who died with unpleasant symptoms
Preferences about treatment or withholding treatment, for example ‘What if nobody listens to me or takes my wishes seriously?’
Fears about morphine, for example “can't you get hooked on that?”
Death and dying — fears of being dead and the process of dying need to be differentiated
Patient experiences of death and dying
Not wanting to be a burden
‘I don't want to be a burden to my family, that is something that's definitely out of order as far I'm concerned. I've seen other families that have endeavored to cope with situations of that type when they couldn't and it practically destroyed the family’.
Choosing a place to die
‘I go back to my wife who died from cancer. One of the things she said to me was, ‘I know I'm dying but I want to die in my own home’. And my response was, ‘If we can manage to bring that wish to fulfilment we will do that’. And with the help of my 2 daughters and the local community nurses and the doctor, we managed to achieve that. It was hard work. It was very emotional but we managed to carry out her last wish’.
‘I think if the cancer got bad I would like to go to a hospice. My husband is not terribly practical when it comes to looking after someone who is very ill and I think that I would like, if it came to it, I think I'd like to be in a hospice where they control the pain for you, look after you’.
Worries about death and dying
‘Again I don't know from the doctors what is likely to happen apart from they say I will just get weaker and weaker and as more pain occurs in the bones then I will be given more painkiller’.
‘My biggest problem with thinking about death is not the actual dying because I can envisage that as going to sleep and not knowing anything about it like you go in for surgery. You have the anaesthetic and you're gone and you know nothing about it and you just don't wake up. I think of death like that’.
‘What worries me is what's going to happen before [death], particularly with cancer because you hear so much about the pain. I've experienced pain, I've had the pain in this breast so I have experienced pain and that side of it does worry me in wondering how I would cope with it’.
Acceptance of dying
‘Everybody is so different. Some people can shout, some people can scream, some people are quiet, it's very different, difficult. But acceptance is a great thing. It heals the mind. You know, you didn't bring it on yourself. You didn't make yourself sick. It comes on. You don't know why. So, that's all I can say because that's all I can get from it. I accept it’.
‘Life is a mixture of all sorts of things. There are sad moments and there are moments when things have gone wrong and there are things when you can be upset and angry about things, but find the positives. And rejoice in those positives and rejoice in the life that you've had. Celebrate the life that you've had and come to terms with the fact that it will ultimately end. The only difference is that you now know and some people … well it comes to an end and they don't know about it’.
Different religious and cultural groups have different approaches to the dying process. It is important to be sensitive to cultural and religious beliefs. If in doubt ask a family member. You are more likely to cause offence by not asking than by asking.
Assessment of the patients' needs
Try to discover which problems are causing the patient and/or carers most concern and address those concerns where possible. Patients often under-report their symptoms and families or carers may misinterpret symptoms.
Physical examination
Keep examination to a minimum to avoid unnecessary interferenmce. Check:
Sites of discomfort/pain suggested by history or non-verbal cues Mouth Bladder and bowel
Psychological assessment
Find out what the patient wants to know. Gently assessing how the patient feels about his/her disease and situation can shed light on individual needs and distress.
Investigations
Any investigation at the end of life should have a clear and justifiable purpose (e.g. excluding a reversible condition where treatment would make the patient more comfortable). The need for investigations in the terminal stage of illness is minimal.
Review of medication
In the final 48 hours, comfort is the priority. Stop unnecessary medication such as oral hypoglycaemics or warfarin. Continue analgesia, anti-emetics, anxiolytics or antipsychotics and anticonvulsants. Diabetes can be managed with short acting insulin as needed. Consider alternative routes of drug administration such as rectal administration of drugs such as paracetamol and morphine, patches or a syringe driver. Explain any changes in medication that you make to relatives and/or carers.
Symptom control
Dying patients tolerate symptoms very poorly because of their weakness. Nursing care is the mainstay of treatment. As a GP, your role is to:
Seek to prevent new problems arising. For example, ensure use of appropriate mattresses and measures to prevent bed sores Treat specific symptoms, such as dry mouth Think ahead—discuss treatment options which might be available later such as use of a syringe driver, buccal, rectal or transcutaneoous preparations to deliver medication when/if the oral route is no longer possible. Discuss the use of strong analgesia which may also have a sedative effect. Ensure there is a clear management plan agreed between the medical and nursing team and the patient, family members and/or carers. Anticipate probable needs of the patient so that immediate response can be made when the time comes—define clearly what should be done in the event of a symptom arising/worsening; ensure drugs or equipment that may be needed are in the home; alert all those who might become involved, including local ambulance services and out-of-hours providers, about the patient and the care plan that has been agreed.
Referral to specialist palliative care services
Involve specialist palliative care services ideally before the terminal phase is reached. Referral in the terminal phase is appropriate when:
One or more distressing symptoms prove difficult to control There is severe emotional distress There are dependant children and/or elderly vulnerable relatives involved
Terminal anguish and spiritual distress
Terminal anguish is characterized by overwhelming distress, often related to unresolved conflict, guilt, fears or loss of control. Anxiety can be increased if patients are unaware of the diagnosis, but feel that people are lying to them, or they have certain symptoms such as breathlessness, haemorrhage or constant nausea or diarrhoea. Patients with weak religious conviction are more likely to be anxious. Convinced believers and non-believers have less anxiety. Those with young dependant children or other dependant relatives or other unfinished business to attend to, such as legal affairs, are also likely to suffer more anguish.
Empathic listening can itself be therapeutic. Talk to the patient, if possible, about dying and try to break down fears into component parts. Address those fears that can be dealt with. As a last resort, and after discussion with the patient (where possible) and/or relatives, consider sedation.
Terminal restlessness
Common causes of terminal restlessness include:
Pain or discomfort—urinary retention, constipation, pain which the patient cannot tell you about or excess secretions in throat are all common culprits Opioid toxicity—causes myoclonic jerking. The dose of morphine may need to be reduced if a patient becomes uraemic Biochemical causes—such as hypercalcaemia, uraemia. If it has been decided that biochemical abnormalities will not be treated, do not check for them Psychological or spiritual distress
Treat reversible causes. For example, catheterize a patient in retention or consider giving hyoscine to dry up secretions. If the patient is still restless, treat with a sedative. This does not shorten life but makes the patient and any relatives in attendance more comfortable. Suitable drugs include haloperidol 1–3 mg three times daily orally, chlorpromazine 25–50 mg three times daily orally, diazepam 2–10 mg three times daily orally, midazolam 10–100 mg/24 hours via syringe driver or 5 mg subcutaneously stat or levomepromazine 25–100 mg/24 hours via syringe driver or 6.25 mg subcutaneously stat.
Excessive respiratory secretion (death rattle)
Death rattle describes the noisy, moist breathing heard in many patients approaching death. It rarely distresses patients but can be very distressing for relatives in attendance.
Reassure relatives that the patient is not suffering or choking. Try repositioning and/or tipping the bed head down (if possible) to reduce the noise. Treat prophylactically. It is easier to prevent secretions forming than remove accumulated secretions. Suitable drugs include:
Glycopyrronium—non-sedative drug. Give 200 mcg subcutaneously stat and review after an hour. If that is effective, repeat every 4 hours or set up a syringe driver delivering glycopyrronium 0.6–1.2 mg/24 hours subcutaneously. Hyoscine hydrobromide—sedative in high doses. Give 400 mcg subcutaneously stat and review the patient's response after 30 minutes. If this is effective, give 400–600 mcg 4–8 hourly or 0.6–2.4 mg/24 hours via syringe driver. If the patient is conscious and respiratory secretions are not too distressing, it may be more appropriate to use a transdermal patch (Scopaderm 1.5 mg over 3 days) or sublingual tablets (Kwells). Dry mouth is a side effect.
Terminal breathlessness
Terminal breathlessness is a particularly distressing symptom for both patients and carers. Support those in attendance and explain your management to them. If the patient has sticky secretions, then nebulized saline, suction and/or physiotherapy (if available) may be helpful.
In all cases, consider diamorphine or morphine that helps to reduce the sensation of breathlessness and can help patients relax, which can sometimes make breathing more efficient as well as more comfortable. The dose depends on whether the patient is being converted from oral morphine or an alternative opioid. If the patient has not been on an opioid until that point, start diamorphine 5 mg/24 hours subcutaneously via a syringe driver. If the patient has previously been taking oral morphine, divide the patient's total 24-hour dose by 3 to obtain the 24 hour, subcutaneous dose of diamorphine. Increase the dose slowly as needed. Patients already on subcutaneous diamorphine should have their dosage increased by 25–50% to allay symptoms. Combine subcutaneous diamorphine with midazolam 5–10 mg/24 hours via syringe driver to allay anxiety associated with the breathlessness.
Use of syringe drivers
Although drugs can usually be administered by mouth to control symptoms of terminal illness, occasionally that is not possible. Portable syringe drivers give a continuous subcutaneous infusion and can provide good control of symptoms with little discomfort or inconvenience to the patient. Indications include:
The patient is unable to take medicines by mouth owing to nausea and vomiting, dysphagia, severe weakness or decreased conscious level There is bowel obstruction and further surgery is inappropriate The patient does not want to take regular medication by mouth
Types of syringe driver
There are two types of syringe driver (Fig. 1) in common use in the UK. Each health care trust or primary care organization should use only one type of syringe driver to decrease risks of dose errors.
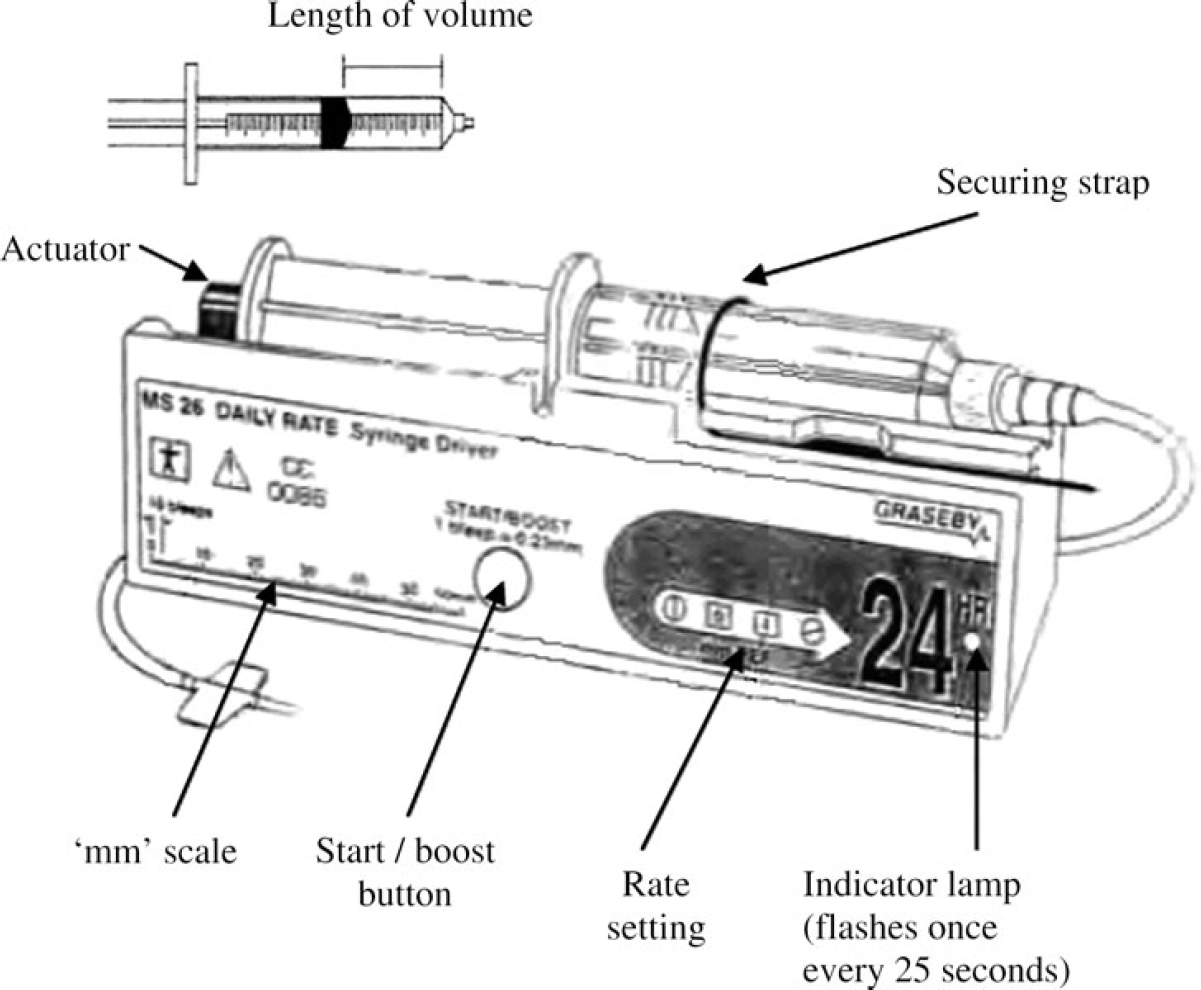
The syringe driver.
The MS26 Green driver dispenses a set number of millimetres of fluid in a syringe every 24 hours. In other words, it dispenses drugs at a daily rate. The rate is equal to the measured ‘length of volume’ in millimetres divided by the delivery time in days. For example, a rate of 48 means that 48 mm of fluid will be dispensed in 24 hours.
The MS16A Blue driver dispenses a set number of millimetres of fluid in a syringe driver every hour. In other words, it dispenses drugs at an hourly rate. The rate is equal to the measured ‘length of volume’ in millimetres divided by the delivery time in hours. Therefore, if you wish to dispense 48 mm of fluid, the rate must be set at 48/24 = 2 mm/hour.
General principles
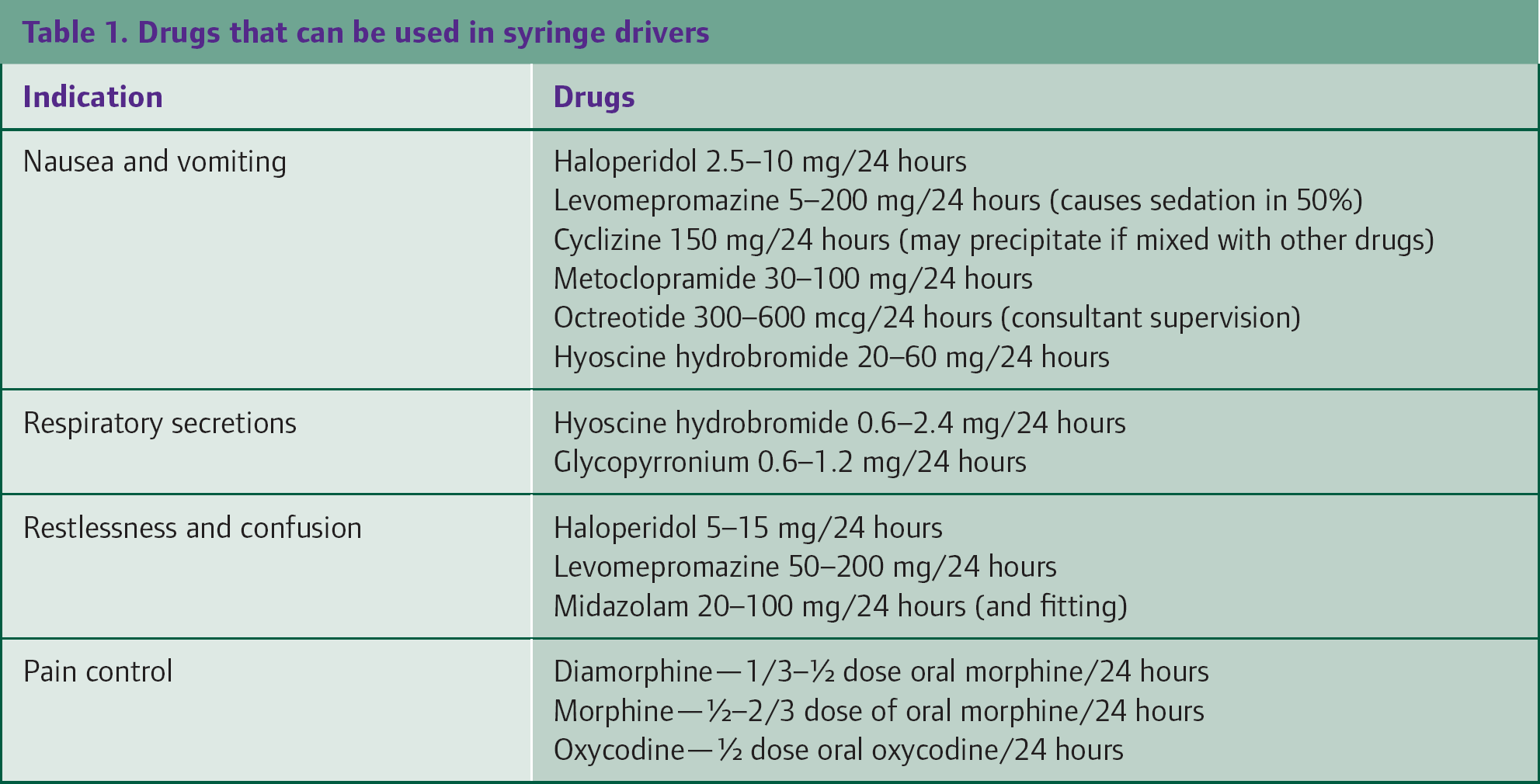
Local policies may differ, and hands-on training is essential. Incorrect use of syringe drivers is a common cause of drug errors. Drugs that can be used in syringe drivers are listed in Table 1. Diazepam, chlorpromazine and prochlorperazine are all drugs commonly used in palliative care that are not suitable for use in a syringe driver.
Drugs that can be used in syringe drivers
Draw up the prescribed 24-hour medication mixed with water for injection as a diluent, except if levomepromazine, diclofenac, octreotide or ondansetron are being used when 0.9% sodium chloride should be used as a diluent instead of water. Set the rate on the syringe driver based on a length of fluid in millimetres per unit time. The subcutaneous infusion solution should be monitored regularly both to check for precipitation and discolouration, and to ensure that the infusion is running at the correct rate. Common problems that you might encounter are listed in Table 2.
Troubleshooting common syringe driver problems

Mixing drugs in syringe drivers
Provided there is evidence of compatibility, drugs can be mixed in syringe drivers. Diamorphine can be mixed with:
Cyclizine Dexamethasone (at doses of less than 4 mg in 24 hours) Glycopyrronium Haloperidol Hyoscine hydrobromide Hyoscine butylbromide Levomepromazine Metoclopramide Midazolam Octreotide Ondansetron
If mixing drugs in a syringe driver, ensure that drugs are compatible. If combining two or three drugs in a syringe driver, a larger volume of diluent and larger syringe may be needed (e.g. a 20- or 30-ml syringe). Do not combine more than three drugs in one syringe driver. If more than three drugs are needed, re-assess the treatment aims. Further information on mixing drugs in syringe drivers can be obtained from website: www.book.pallcare.info.
Use a separate syringe driver for:
Dexamethasone (if using doses of 4 mg or more per 24 hours) Phenobarbital Diclofenac Ketamine Ketorolac
Notes on using cyclizine in a syringe driver: Cyclizine is incompatible with 0.9% normal saline. If the dose of cyclizine required is greater than 75 mg/24 hours in conjunction with a dose of diamorphine of greater than 160 mg/24 hours, dilute the solution to a volume greater than 14 ml in a 20-ml syringe to prevent precipitation in the syringe.
Notes on using levomepromazine in a syringe driver: Levomepromazine can be an irritant. If skin site soreness becomes a problem, dilute the levomepromazine with 0.9% saline rather than water for injections. If diamorphine is combined with levomepromazine, normal saline can only be used when the diamorphine concentration is less than 40 mg/ml. If the diamorphine concentration is greater than 40 mg/ml, use water for injections and either increase the size of syringe used or consider adding dexamethasone 1 mg to reduce the skin reaction.
Key points
When a patient will die is difficult to predict Signs of approaching death include day-by-day deterioration, gaunt appearance, profound weakness, difficulty swallowing medicines, reduced intake of food and fluids, drowsiness or reduced cognition and inability to co-operate with carers Talking about death can be difficult. Try to be sensitive and address the patients ‘and carers’ fears The goals of care in the last 48 hours are to ensure that patients are comfortable—physically, emotionally and spiritually, and make the end of life peaceful and dignified When patients are no longer able to take medication by mouth, stop any medication not relieving symptoms and consider the use of a syringe driver