
Abstract
Around 3.8% of the UK population are registered as having diabetes according to the prevalence data from the Quality and Outcomes Framework (QoF). There is a strong evidence base that good control of blood glucose levels, blood pressure levels and the use of statin therapy reduces the risk of developing microvascular complications (retinopathy, nephropathy and foot problems) and macrovasular complications (heart attacks and strokes).
The concept of regular review for control and complications in people with diabetes is explicit in many statements of diabetes care. An example is the UK National service framework for diabetes (2002) which in standards 10 and 11 states:
‘All young people and adults with diabetes will receive regular surveillance for the long term complications of diabetes
The NHS will develop, implement and monitor agreed protocols and systems of care to ensure that all people who develop long-term complications of diabetes receive timely, appropriate and effective investigation and treatment to reduce their risk of disability and premature death’
This idea of regular review has been developed into the concept of an annual review which has become the basis for many of the quality control structures for diabetes care throughout the world (IDF, 2005).
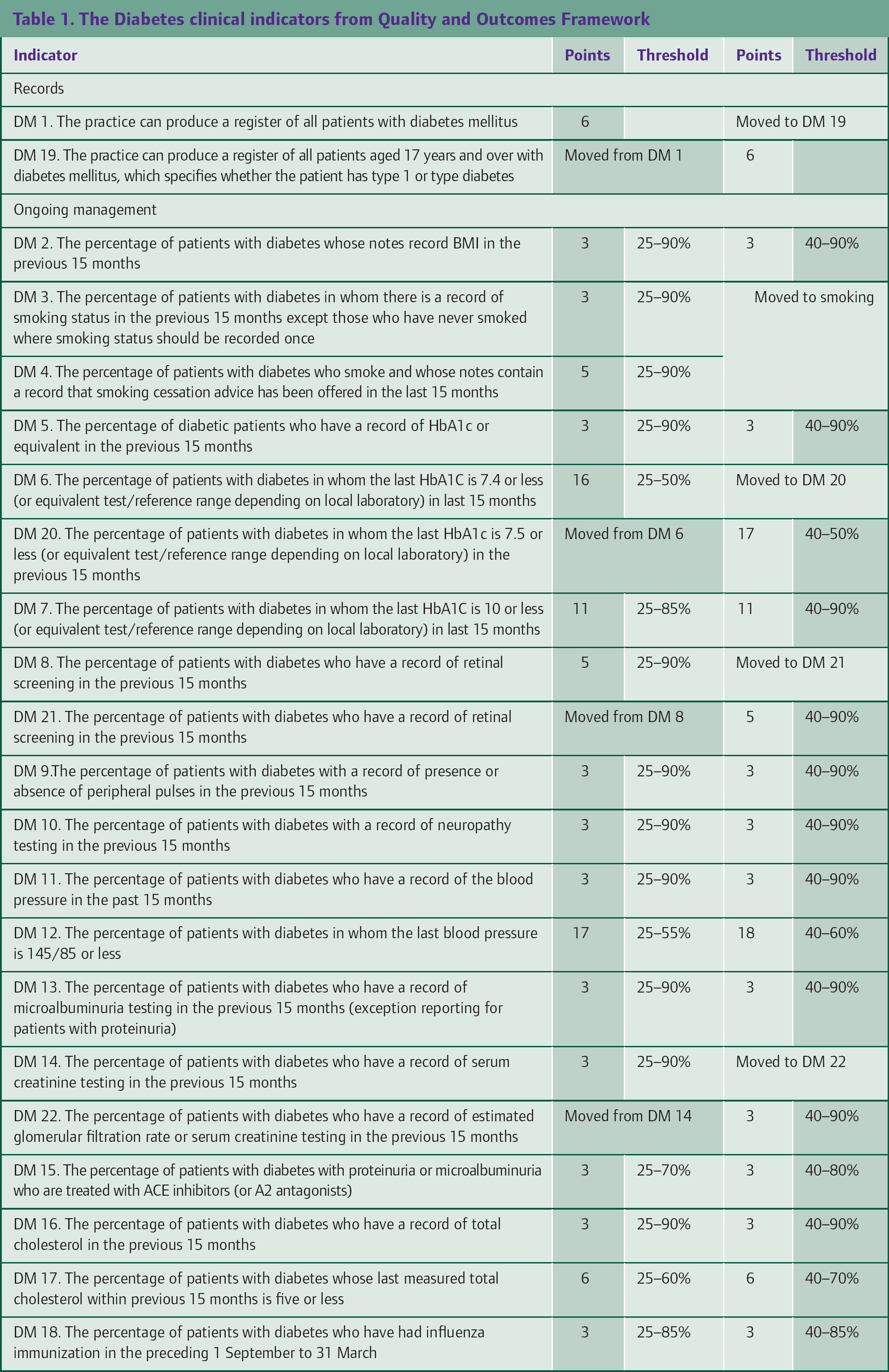
The QoF for diabetes has 18 evidence-based clinical indicators for diabetes. Achievement of these indicator standards is a mark of good diabetes care in the practice. An annual review for everyone with diabetes on the practice diabetes register will facilitate the achievement of full points for the practice from the diabetes QoF. During GP training, you will get opportunity to take part in the diabetes clinic and conduct annual diabetes reviews.
Topic material
The diabetes clinical indicators from QoF
The 18 clinical indicators for diabetes from the QoF are listed in Table 1. These form the content outline for the annual diabetes review process in every general practice in the UK.
The Diabetes clinical indicators from Quality and Outcomes Framework
Running a diabetes clinic in the practice
Staff and dedicated diabetes time
Many practices in the UK run diabetes clinics in which practices nurses with special training and expertise in diabetes care recall and review people with diabetes. Such clinics are supervised by the GP partner in the practice with an interest in diabetes care.
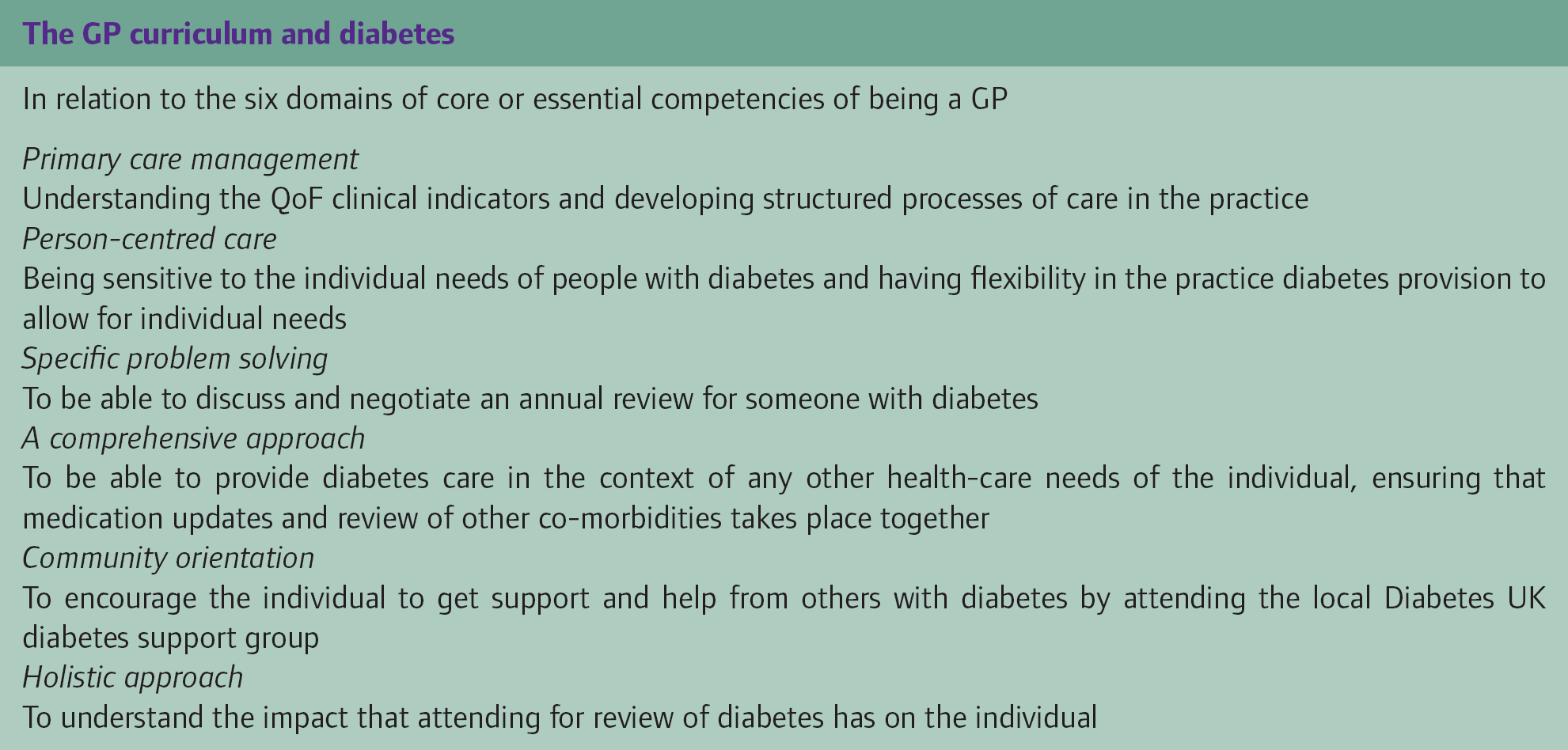
The GP curriculum and diabetes
In relation to the six domains of core or essential competencies of being a GP
Primary care management
Understanding the QoF clinical indicators and developing structured processes of care in the practice
Person-centred care
Being sensitive to the individual needs of people with diabetes and having flexibility in the practice diabetes provision to allow for individual needs
Specific problem solving
To be able to discuss and negotiate an annual review for someone with diabetes
A comprehensive approach
To be able to provide diabetes care in the context of any other health-care needs of the individual, ensuring that medication updates and review of other co-morbidities takes place together
Community orientation
To encourage the individual to get support and help from others with diabetes by attending the local Diabetes UK diabetes support group
Holistic approach
To understand the impact that attending for review of diabetes has on the individual
Health-care assistants are now being employed by a number of practices. They can help in diabetes clinics by collecting and recording some of the clinical information, for example weight, blood pressure and foot screening, leaving the practice diabetes nurse more time to spend on education and support. In practices with small numbers of people with diabetes, dedicated diabetes clinics may be impractical and dedicated diabetes time may be best provided in dedicated slots in ordinary surgery times.
It is vital that staff providing diabetes care are appropriately skilled. There are a number of excellent diabetes education and training programmes that are available in the UK which enable a health-care professional to gain certification of training through certificates, diplomas and master's degrees in diabetes. One example is the Certificate of Diabetes Care from the University of Warwick which is a 6-day taught programme delivered over 6 months. Over 6000 GPs and practice nurses have successfully completed the programme (www.Warwick.ac.uk/go/studydiabetes, accessed on 11.08.2008). A number of Universities have master's programmes in diabetes for those who wish to study diabetes at this level.
The Primary Care Diabetes Society has been set-up as a national group to offer support and encouragement to community diabetes teams. It has an annual conference and other educational events (www.pcdsociety.org). The journal Diabetes and Primary Care contains specific pages dedicated to the Society.
Diabetes register
One of the basic building blocks for running such a clinic is a diabetes register. In the vast majority of practices in the UK, this is an electronic register. The register prevalence of diabetes from the 2006–07 QoF database is 3.7%. Figures below that, in practices with ‘average’ ethnicity and an ‘average’ age distribution, imply under-recording or under-diagnosis. In practices with many people from ethnic minority backgrounds, the practice prevalence may rise to 8–12%.
Clinic template
Practice clinical computer systems contain a diabetes clinic template which automatically uses the appropriate Read codes for recording care. These are updated each year to ensure that they record care information by designated Read codes in a form that will fit the quality indicators from the new contract. A diabetes dataset has been developed and is being modified to allow accurate recording of the various items of clinical care that need to be recorded to document care for the contract quality payments. In most GP diabetes clinics, blood tests are requested 2 weeks before clinic attendance, so that this information is available on the clinic day. Many systems receive test results from the local laboratory by electronic download. These test results are then posted into the diabetes clinical template.
Blood tests before annual review
People with diabetes need to have blood tests done 1–2 weeks before the annual review so that results can be assessed and discussed at clinic visit.
It is usual for the following tests to be done:
Urea and electrolytes (U&Es) and liver function tests (LFTs) Creatinine and estimated glomerular filtration rate (eGFR) which is calculated by the laboratory from the creatinine Glycosylated haemoglobin (HbA1c). Total cholesterol with HDL cholesterol, LDL cholesterol and triglycerides as indicated.
People are also asked to bring a first-pass urine specimen with them to the annual review clinic.
Annual review targets
Managing glycaemia—to achieve the quality targets
Optimize blood glucose lowering therapy by following the NICE Guideline on management of type 2 diabetes (NICE, 2008; www.nice.org.uk).
The target HbA1c where safely achievable is 6.5% for those on diet therapy alone, those on metformin alone and those on metformin plus sulphonylurea. It is 7.5% for those on maximal tolerated doses of metformin plus sulphonylurea who will require third-line therapy. The QoF target is an HbA1c of 7.5% or below.
Managing blood pressure—to achieve the quality targets
Optimize blood pressure by following the NICE Guideline on management of type 2 diabetes (NICE, www.nice.org.uk).
Blood test glucose
AJ Photo/Science Photo Library.
What is done at the Annual Review?
Welcome
General questions, for example how are you? Are there any problems with your diabetes? Is there anything bothering you? Ask about smoking status and record on the computer
Education
Ensure that they have been referred to a structured group education programme and have attended. Update education about diabetes on a one-to-one basis
Measure
Weight and blood pressure Check urine for proteinuria using dipstick Send off the first-pass urine sample to the laboratory for an albumin: creatinine ratio as the test for microalbuminuria
Check feet and give foot education
Ask about any history of ulceration With the shoes and socks off look for any signs of bony abnormality or callus Palpate the foot pulses Use a 10-g nylon monofilament on their feet to detect loss of protective pain sensation If there is a history of ulceration, bony abnormalities, absent foot pulses or loss of protective pain sensation that person has an ‘at risk’ foot and needs to be referred to the local podiatry foot at risk clinic for further assessment, education and follow-up
Ask about attendance for eye screening
Screening for retinopathy is by digital retinal photography through dilated pupils. Each area should have a retinal screening service and it is important to check that each person with diabetes has attended for their screening and that the results are on the practice's clinical computer system
Record
All the above pieces of information onto the computer template and ensure that all blood test results are discussed with patient
Discuss
Glycaemic control, blood pressure control and lipid control results Any changes or additions to therapy that are needed Targets that the person with diabetes wants to achieve in an agreed time frame Ensure that the appropriate follow-up appointment is made
The target is a blood pressure at or below 140/80. An angiotensin-converting enzyme (ACE) inhibitor or if not tolerated an angiotensin receptor blocker is the first choice of agent especially if microalbuminuria is present.
Managing lipids
Assess cardiovascular disease risk if indicated and initially prescribe generic statin (e.g. Simvastatin 40 mgs once daily) following the lipid protocol in the NICE type 2 diabetes guideline.
Key points
Ensuring that everyone with diabetes has an annual review enables the practice to demonstrate that it is delivering good diabetes care and facilitates the achievement of full QoF scores for diabetes care The diabetes clinic template on the practice clinical computer system gives a full outline of all that needs to be done at an annual review The completion of this template allows the health-care professional and the person with diabetes to monitor the progress being made in their diabetes care and facilitates the setting of goals for the next year