
Abstract
Staphylococcus aureus (Fig. 1) is a gram-positive bacterium that is a common colonizer of human skin and mucosa. It can cause disease, particularly if there is an opportunity for the bacteria to enter the body. A small proportion of S. aureus bacteria is resistant to methicillin and other beta-lactam antibiotics, including the penicillins and cephalosporins. Infections due to these strains are no more dangerous or virulent than other varieties of S. aureus, but they are much more difficult to treat because the range of effective antibiotics is considerably reduced. These antibiotic-resistant bacteria are termed methicillin-resistant S. aureus (MRSA). The first strain of methicillin resistant S. aureus appeared in Cairo in 1961. Since that time, it has spread to become a worldwide problem. This article aims to provide a practical strategy to enable GPs to manage MRSA colonization and potential or actual MRSA infection in the community.
The GP curriculum and MRSA
Management of MRSA in primary care is covered under two sections of the RCGP curriculum:
Curriculum Statement 5: Healthy people — promoting health and preventing disease — deals with prevention of illness through MRSA infection Curriculum statement 15.10: Skin problems — covers diagnosis and treatment of patients with skin infection, the most common presentation of MRSA infection in the community
Both these statements require the GP to be able to demonstrate an understanding of the epidemiology of MRSA presenting in primary care and the risk factors for MRSA infection. In all cases, GPs should take a person- and family-centred approach with an understanding of the psychological impact that being colonized or infected with MRSA has on the patient and family. It is important for GPs to identify the patient's health beliefs and reinforce, modify or challenge these beliefs as appropriate. The GP should encourage questioning by the patient and encourage access to further information and the use of patient support groups.
In addition, Statement 5 requires GPs to understand the principles of prevention and preventative strategies, as applied to MRSA. Statement 15.10 mentions bacterial skin infection as an important topic in its knowledge base and requires GPs to
be able to manage primary contact with patients who have a skin problem demonstrate a reasoned approach to the diagnosis of skin symptoms using history, examination, incremental investigations and referral as appropriate be familiar with treatments commonly used in primary care for the treatment of skin infection, and aware of specialized treatments such as those used in the management of MRSA intervene urgently when patients present with an emergency skin problem describe and implement the key national guidelines that influence health-care provision for skin problems
Epidemiology
Methicillin resistance rates of Staphylococcus aureus vary considerably between countries, with a high prevalence in the United States and southern Europe and a low prevalence in Scandinavia. In England, between 2006 and 2007, there were 17 404 cases of S. aureus bacteraemia reported, of which 6381 were due to MRSA (37%). However, these samples were all taken from people who were ill and in hospital, so the community prevalence is almost certainly much lower. After a peak in infection rates in the late 1990s, incidence of MRSA is now falling in England with a 12% decrease in reported cases of MRSA bacteraemia between 2001 and 2007.
Electron microscope image of Staphylococcus aureus. CDC/Janice Carr/Jeff Hageman, M.H.S.
Types of MRSA
Hospital-acquired MRSA
Patients become colonized with hospital- or health care-acquired MRSA (HA-MRSA) through contact with health-care facilities. Infections may present more than 48 hours after admission in hospital (hospital onset) or in the community in patients who have had contact, directly or indirectly, with hospitals, care homes or other health-care facilities (community onset), for example in patients recently discharged from hospital. This is by far the most common type of MRSA infection that a GP is likely to see. It tends to affect:
Elderly patients (69% of infections occur in those over the age of 65) Those who are debilitated or chronically ill Those who are regular hospital attenders and Patients with open skin lesions or who have had recent surgery
Case history 1
Rose is a 76-year-old diabetic lady. She has a longstanding venous ulcer on her left leg. She has recently come out of hospital after a lengthy admission for treatment of a severe chest infection. Sue, the district nurse has been to visit. Rose is generally well and seems completely recovered from her chest infection. However, Sue is not happy with Rose's leg ulcer. It seems to have become slightly larger, there is some erythema surrounding it and the exudate coming from the ulcer is offensive. She wonders if Rose might have a wound infection and requests a GP review.
You review Rose and agree that she seems to have an infection of her leg ulcer. As she is well, she does not need hospital admission, but in view of her recent hospital stay and history of pneumonia treated with intravenous antibiotics, the possibility of HA-MRSA with onset in the community goes through your mind. You take a swab from the ulcer and start her empirically on flucloxacillin 500 mg four times a day.
A few days later you get a phone call from the microbiology laboratory to tell you that MRSA has been isolated from the swab. You switch Rose to a combination of doxycycline and rifampicin on the advice of the microbiologist and her leg ulcer starts to improve.
Community-acquired MRSA
Most MRSA infections that appear to have a community onset occur in patients who have had contact, directly or indirectly, with hospitals, care homes or other health-care facilities. These MRSA strains are typical of the local HA-MRSA strains.
Since the late 1990s, new strains of MRSA have emerged. These cause infections in patients who have no history of contact with any type of health-care facility, either directly or indirectly. The strains of MRSA responsible for these infections are genotypically and phenotypically distinct from HA-MRSA and have been termed community-acquired MRSA (CA-MRSA).
Although incidence is rising, particularly in the United States, Canada and Australia, CA-MRSA infection is still rare accounting for just 0.5% of all MRSA infections worldwide. There have been 100 proven cases of CA-MRSA infection in England in the past 3 years. Although CA-MRSA infections are rare at present, they are important as they usually affect young, previously healthy people and may follow a rapid and devastating course.
Case study 2
Greg, a 22-year-old man who is a keen rugby player, comes to the surgery. He has developed a tender, fluctuant, discharging skin lesion on the back of his right calf. He does not feel unwell and does not have a fever. There is a moderate amount of erythema surrounding the lesion. He has self-medicated with some fusidic acid cream that he had left over from a minor skin infection that he saw another GP in the practice about earlier in the year. However, on this occassion with no effect. He mentions that several of his rugby team members have also had similar skin problems.
It is clear from Greg's history and your examination that Greg has a small skin abscess on his calf. The most likely microbial cause of this is S. aureus, although pyogenic streptococci, such as β-haemolytic streptococci or group C or G streptococci, are other possibilities.
You swab some of the pus that has discharged from the skin lesion on Greg's leg and send it to the laboratory. You then start him empirically on flucloxacillin 500 mg four times a day.
Much to your surprise, the swab result comes back showing MRSA infection. Greg has not had any recent contact with health-care facilities. You take advice from the local microbiologist who suspects a CA-MRSA infection and advises you to change Greg's antibiotics. He recommends a combination of rifampicin and trimethoprim. Greg makes an uneventful recovery over the next week.
Spread
Spread of MRSA from person to person is by direct contact with the skin, particularly if the skin is heavily colonized or if the affected patient has a skin condition, such as eczema, which causes increased shedding of skin and thus organisms. Skin scales carrying bacteria may also spread infection and can be dispersed into the environment by activities such as shaking clothing or bedmaking. Staphylococci shed into the environment can survive long periods in dust. Box 1 lists the do's and don'ts of MRSA prevention.
The do's and don'ts of MRSA prevention
Keep the environment as clean and dry as possible Clean surfaces with commercial disinfectants or a 1:100 solution of diluted bleach Wear gloves when managing wounds and safely dispose of dressings and any other materials then come into contact with any bodily substances Always wash hands after every patient contact, even if you were wearing gloves, either with soap and warm water or with an alcohol-based hand sanitizer Patients colonized or infected with MRSA should, whenever possible, be placed in a separate room or kept with other patients who have MRSA. Application of topical treatments for known carriers may reduce skin carriage and reduce the likelihood of infection during admission
Practice standard infection control precautions in the community, for example wear disposable gloves if you are in contact with bodily fluids and use aseptic technique for wound care Decontaminate your hands before and after giving care, either by using soap and water or an alcohol-based hand sanitizer, even if you have been wearing gloves People with MRSA living at home can work and socialize as usual. They do not need to restrict contact with friends, children or the elderly. In nursing homes and other residential care homes, people with MRSA should socialize as normal. They should not share a room if they have a chronic open wound or invasive device, such as a urinary catheter. If a patient known to be carrying MRSA or who has a known MRSA infection requires hospital or care home admission, it is important to inform the hospital or care provider so that the patient is screened for ongoing carriage of MRSA either prior to admission or on admission and can be treated and nursed appropriately.
Colonization
About 30% of the general population is colonized by S. aureus. In about one in 10 of these cases (3% of the population overall), the S. aureus is MRSA. The percentage of people who carry S. aureus and proportion having MRSA is increased among hospital patients due to increased exposure.
Under these circumstances, S. aureus is a commensal organism. Patients who are colonized by S. aureus have no symptoms or signs and are not ill, but can infect themselves. In some individuals, colonization is transient lasting just hours or days; in others, colonization is more long-term lasting years. Carriage sites are most commonly the nose and the skin, especially skin-folds such as the axilla or groin. Screening of patients by culture of samples from the anterior nares identifies 80% of carriers. Screening from additional sites increases the sensitivity to over 92%.
Treatment of S. aureus colonization
Carriage of MRSA may only be transient, sometimes lasting just hours, and is unlikely to harm a healthy carrier. Therefore, screening and treatment of healthy MRSA carriers is not usually necessary in the community. In high-risk situations (for example, prior to major surgery such as hip or knee replacement), screening and then skin and nose treatment of those screening positive may be warranted.
Similarly, routine screening of staff for MRSA carriage, and treatment of those testing positive, is not recommended. Pre-employment screening of staff for MRSA carriage is also unnecessary but local guidelines may vary.
Where it has been deemed necessary to treat a patient or health-care worker colonized with MRSA, topical mupirocin ointment (Bactroban nasal) is recommended for eradication of nasal carriage of MRSA. The ointment should be applied three times daily for 5 days and a sample taken 2 days after treatment to confirm eradication. The course may be repeated if the sample is positive. To avoid the development of resistance, the treatment course should not exceed 7 days and the course should not be repeated on more than one occasion. If the MRSA strain is mupirocin resistant or does not respond after two courses, then elimination can often be achieved with nasal chlorhexidine and neomycin cream (Naseptin). Triclosan 2% (Aquasept) skin cleanser is the preferred treatment for eradication of skin carriage of MRSA.
MRSA infection
MRSA is no more dangerous or virulent than other varieties of S. aureus, but it is much more difficult to treat because the limited range of antibiotics which can be used to treat it. Typical infections that may result from S. aureus infection include
Skin infections and soft tissue infections Urinary tract infections Pneumonia Bone and/or joint infections and Bacteremia (blood stream infection)
Infections are commonly endogenous, caused by the patient's own colonizing strain.
Take a history and examine the patient. Box 2 lists questions to ask yourself when assessing a patient who you think may have a S. aureus infection.
Checklist of questions to ask yourself when a patient presents with a possible S. aureus infection
How severe is the illness? Is it possible to distinguish between Methicillinsensitive S. aureus infection and MRSA infection? If you suspect MRSA, is it likely to be HA-MRSA or CA-MRSA? Do you need to send a sample for microbiological assessment? If so, how? Appropriate clinical samples (swabs, urine samples, sputum specimens) should be sent to the laboratory to confirm infection and provide information on sensitivities to antibiotic treatment Do you need to start empirical antibiotic treatment (or definitive treatment if microbiology results are available)? Is surgical treatment, such as incision and drainage, required? Is hospital admission warranted? What advice do you need to give to the patient, family and other contacts of the patient?
Severe infection
If a patient presents with severe pneumonia (especially if it follows a flu-like illness), a suspected bone or joint infection, or is severely systemically unwell, then admit as an acute emergency for specialist care.
Skin and soft tissue infections
Skin and soft tissue infections caused by S. aureus include
Wound infections — these may be surgical wounds, wounds from insertion of intravenous cannulae, wounds formed as a result of other injury, burns, leg ulcers or pressure sores Impetigo—superficial skin infection. A thin-walled blister ruptures easily to leave a yellow-crusted lesion. Folliculitis—inflammation of the hair follicles that presents as pustules in hair bearing areas such as the axilla or beard area Abscess or boil — acute infection of a hair follicle. A hard, tender, red nodule surrounding a hair follicle becomes larger and fluctuant over several days. Abscesses are occasionally associated with localized cellulitis surrounding the lesion and/or systemic upset in the form of fever and malaise. If a group of hair follicles become deeply infected, a swollen, reddened painful area may develop discharging pus from several points. This is termed a carbuncle. Acute paronychia — infection of the skin and soft tissue of the proximal and lateral nail fold that often originates from a break in the skin or cuticle as a result of minor trauma, such as nail biting. Skin and soft tissue of the proximal and lateral nail fold are red, hot and tender; the nail may appear discoloured or distorted. Acute paronychia is treated in the same way as an abscess or boil.
In all cases of skin or soft tissue infection presenting in the community, follow local guidelines for treatment. Swab the lesion if a purulent exudate is present and send the swab for microscopy, culture and sensitivity. If MRSA is suspected because the patient has recently been in hospital or is a frequent hospital attender, was previously known to be colonized with MRSA or has a past history of MRSA infection, then it is especially important to collect a microbiology sample.
Do not give systemic antibiotics to patients with minor infections, such as folliculitis or mild impetigo. Consider topical antibiotics such as fusidic acid cream or treatment with skin antiseptics such as chlorhexidine. For small abscesses less than 5 cm in diameter without cellulitis, incise and drain the abscess but do not prescribe antibiotics unless other family members or close contacts have similar skin lesions. These abscesses are likely to heal spontaneously within a week when drained.
Start empiric antibiotic treatment if other close contacts of the patient have similar skin lesions or if the patient has
systemic symptoms as a result of the skin or soft tissue infection any surrounding cellulitis an abscess of 5-cm diameter or larger that has been incised and drained or extensive impetigo
In the UK, the recommended community antibiotic treatment for suspected S. aureus infection is oral flucloxacillin 500–1000 mg 6 hourly (or oral clindamycin 300–450 mg 6 hourly in penicillin allergic patients); 5–7 days of treatment is usually sufficient. If MRSA is isolated or strongly suspected because of known carriage or past history of infection, then take advice from a microbiologist before starting treatment. If the patient is febrile, appears unwell or is toxic with a skin or soft tissue infection, consider admission for assessment in hospital.
Urinary tract infections
A significant MRSA urinary tract infection with systemic symptoms and the presence of white cells in the urine is likely to require systemic antibiotic treatment. For adults with normal renal function, doxycycline (100 mg two times a day) or tetracycline (250–500 mg four times a day) for 5–7 days is the drug of choice. Trimethoprim (200 mg two times a day) or nitrofurantoin (50–100 mg four times a day) is an alternative.
Antibiotics are unlikely to clear MRSA in the presence of a urinary catheter. There is no evidence that catheter changes should be covered with appropriate antibiotic prophylaxis to prevent catheter-related urinary tract infections.
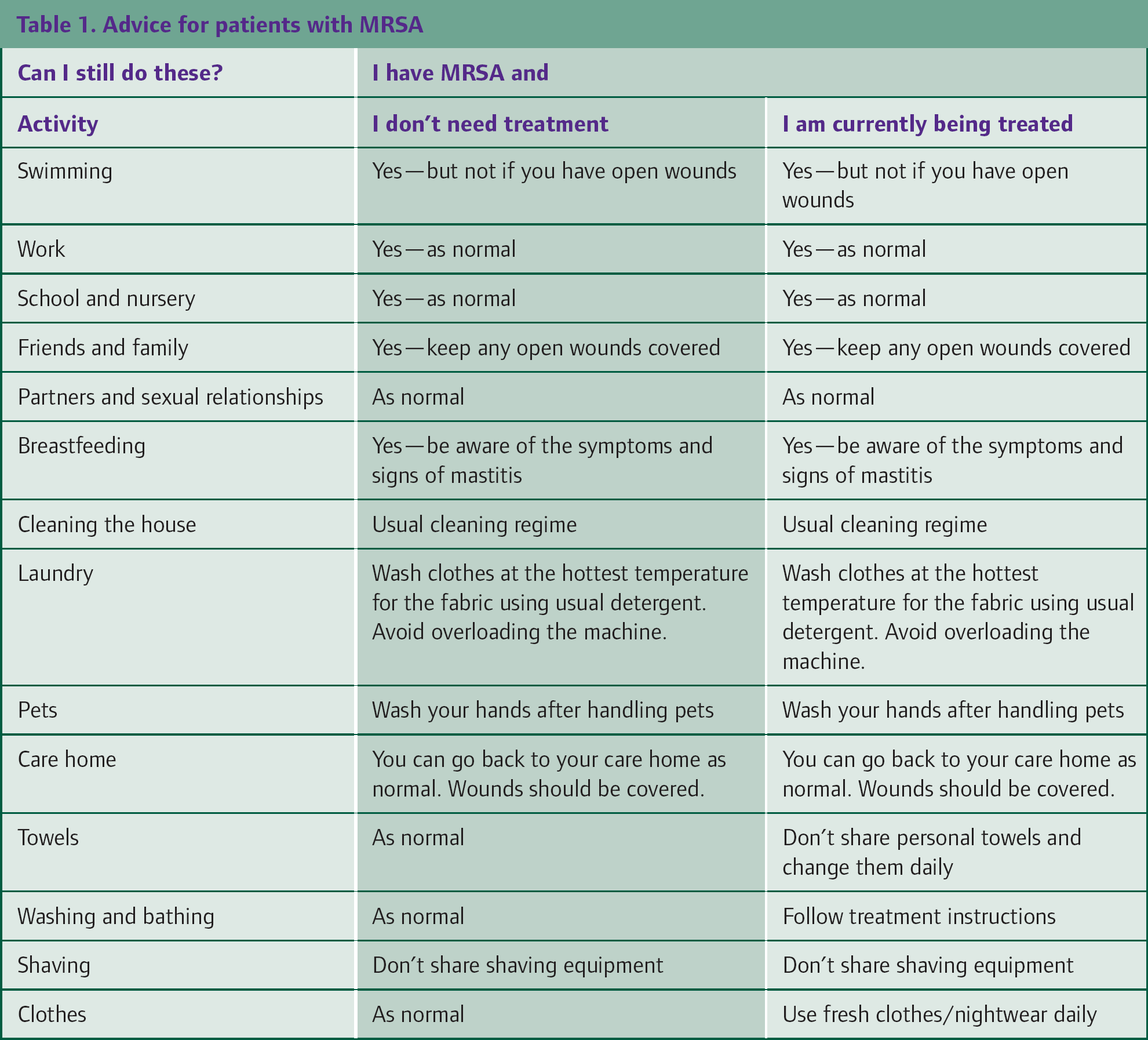
Advice for patients about MRSA
MRSA is commonly known as the ‘superbug’. Mention of colonization or infection with MRSA fills most patients with fear and dread. In all cases, it is important to explore the patient's view and expectations and explain what MRSA is and how it will be managed for that individual. Good information leaflets are available from the Department of Health (the references to these leaflets are listed in the references and further information section) and more information is available via MRSA Action UK (website: mrsaactionuk.net). Table 1 summarizes advice on everyday activities for patients with MRSA.
Advice for patients with MRSA
Key points
Staphylococcus aureus is a gram-positive bacterium that is a common colonizer of human skin and mucosa and can cause disease if there is an opportunity for the bacteria to enter the body A small proportion of S. aureus bacteria are resistant to methicillin and other beta-lactam antibiotics, including the penicillins and cephalosporins, and termed MRSA HA-MRSA is commonly seen in primary care and affects elderly, ill and/or debilitated patients who have been exposed to MRSA as a result of hospital admission or frequent contact with health-care facilities CA-MRSA is rare and affects young, healthy people who no history of contact with health-care facilities Colonization of healthy people with MRSA may be transient and is rarely harmful, so eradication treatment is only necessary in high-risk situations Treatment of MRSA infection depends on the site and severity of infection. Patients with severe infections, such as pneumonia or septicaemia, should be admitted as emergencies. Patients with urinary tract infections or skin/soft tissue infections should have appropriate microbiology specimens taken and be treated as needed with antibiotics in the community. Always take advice from a microbiologist before starting treatment for MRSA or suspected MRSA infection in the community.