
Abstract
Otitis media, the inflammation of the middle ear, is a common primary care problem, and encompasses several subclasses of clinical conditions. The most frequently seen is acute otitis media, which most often affects children. However, otitis media exists in both acute and chronic forms, and also in the presence and absence of infection. Knowledge of how to identify the different types is essential for the formulation of an appropriate management plan.
The GP curriculum and otitis media
Curriculum statement 15.4 requires the GP in training to be competent in:
Knowledge of causes of the symptoms of otalgia and discharging ear Knowledge of otitis media (suppurative/secretory) Indications for appropriate referral to an ear, nose and throat (ENT) specialist Otoscopy Understand the likely outcome of tests (e.g. ear swabs after multiple courses of antibiotics always grow pseudomonas) Effective strategies for dealing with parental concerns, e.g. glue ear Demonstrate an evidence-based approach to antibiotic prescribing to prevent the development of resistance in otitis media
Figure 1 shows the different subtypes of otitis media. The presence of an infective process is suggested by the presence of any of pain, purulent discharge, fever or a hyperaemic tympanic membrane.

Types of otitis media.
Assessing the ear
The tympanic membrane is an oval membrane, measuring approximately 8 mm wide by 10 mm high in the adult. It is tented by the handle of the malleus and infero-anteriorly to this is the light reflex. Around the outside is the fibrous annulus and the tympanic membrane attached to this is the pars tensa. The annulus is incomplete superiorly and the tympanic membrane here is known as the pars flaccida, which is particularly important to identify in chronic suppurative otitis media. It is important to be familiar with the anatomy of the tympanic membrane (Fig. 2) and to be able to identify these structures through otoscopy (Fig. 3) in order to differentiate between the different types of otitis media.

Anatomy of the tympanic membrane.

Appearance of a normal tympanic membrane.
Hearing loss can be a feature of certain types of otitis media, and if it is present, it is conductive in nature. Conductive hearing loss can be detected through the use of Rinne's and Weber's tuning fork tests.
In Rinne's test (Fig. 4), the tuning fork is applied to the mastoid process and then held in front of the ear. Normally, air conduction is louder than bone conduction (Rinne's positive); however, in hearing loss, which is due to otitis media, bone conduction is louder than air conduction (Rinne's negative), signifying a conductive deafness.

The Rinne Test.
In Weber's test (Fig. 5), the tuning fork is placed at the centre of the head. It is normally heard equally in both ears. If the ear which is giving cause for complaint hears the tuning fork less well than the normal ear, that signifies a sensorineural deafness. If it hears it louder than the normal ear, that signifies a conductive deafness, consistent with hearing loss related to otitis media. It is a very sensitive test and is lateralized to the side of a unilateral conductive deafness of as little as 10 — 15 dB.
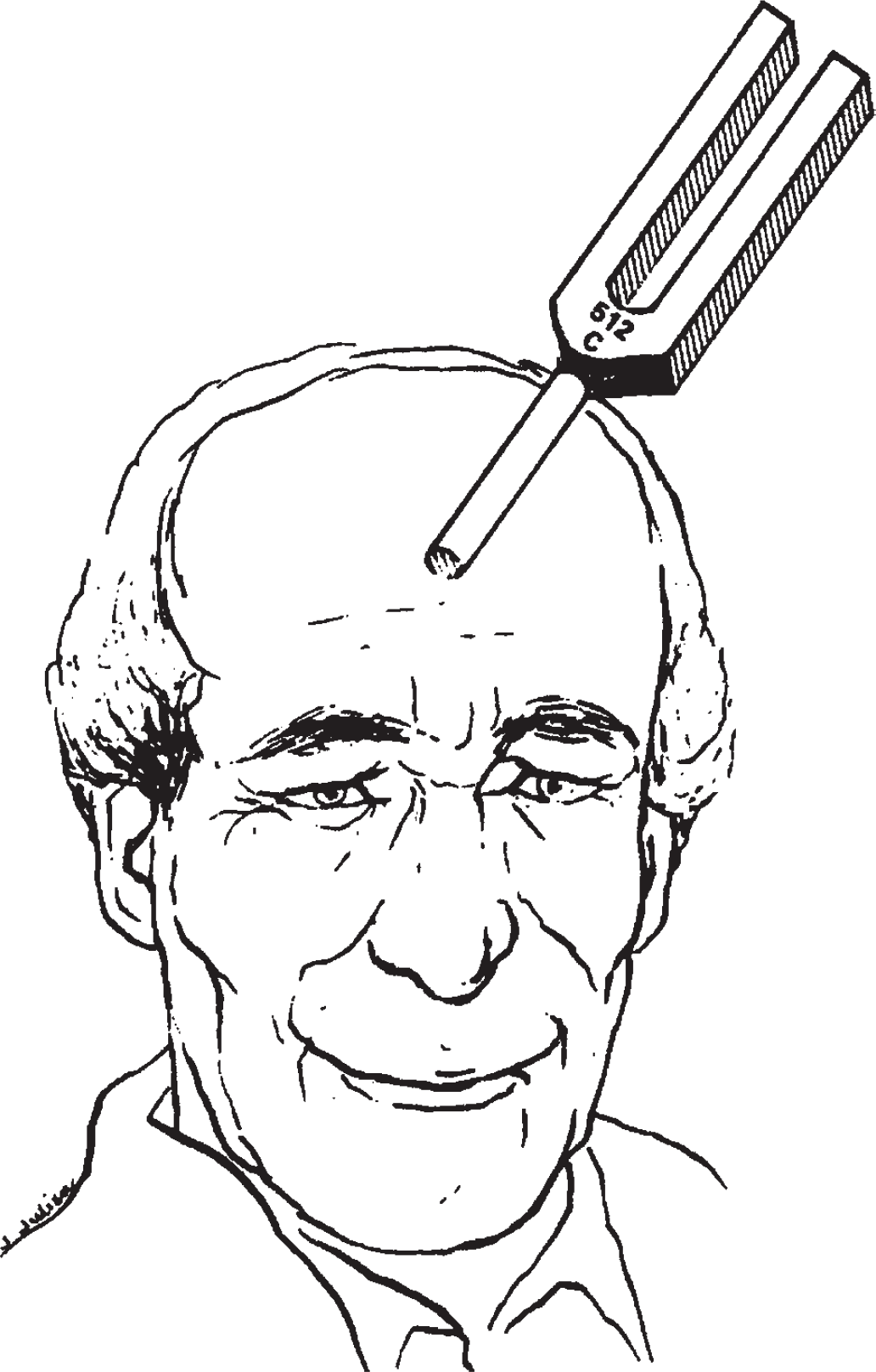
The Weber Test.
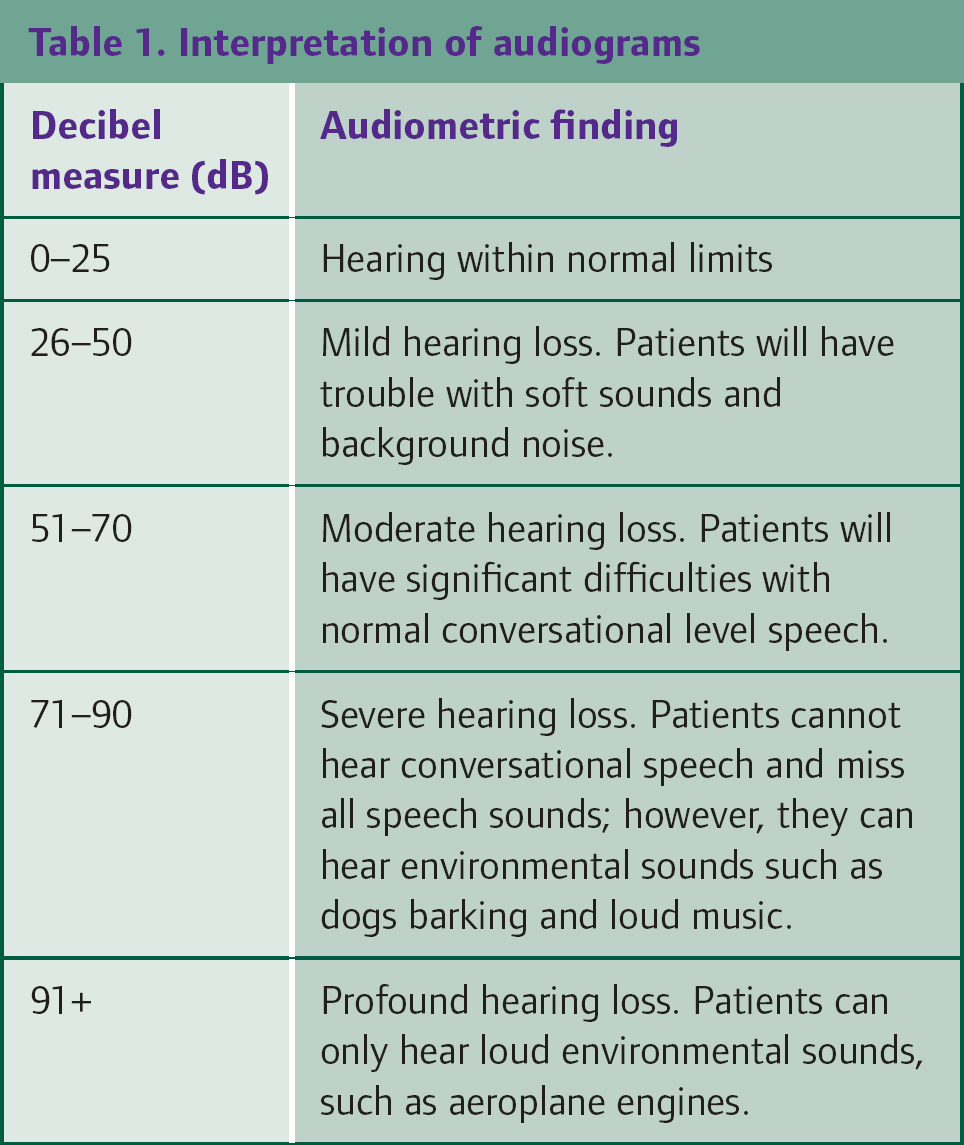
Hearing can be more carefully assessed through the use of pure-tone audiometry and tympanometry. In a child above the age of 4, hearing can be tested using conventional means. Younger children can be conditioned to carry out a particular action (e.g. building a tower with bricks) in response to sound, and very young children (under 2 years) are assessed by distraction audiometry, where sounds lead to turning of the head. General guidelines for the interpretation of audiometric findings are shown in Table 1.
Interpretation of audiograms
Tympanometry is based on the amount of sound reflected back from the tympanic membrane when a tone is introduced into the sealed ear canal and the pressure in the ear is varied. When the pressure in the middle ear corresponds with the pressure in the ear canal, the tympanic membrane will be at its most compliant and will absorb the most sound. A flat tympanogram indicates either a perforated drum or lack of compliance due to a middle ear effusion. This is demonstrated in Fig. 6.

Tympanograms.
Acute suppurative otitis media
This is the most common form of otitis media, seen predominantly in children, with a peak incidence between 3 and 6 years. Three quarters of cases of acute otitis media occur in children aged below 10. Thirty percent of children aged under 3 will visit their GP with acute otitis media each year, and about 10% of children will have an episode of otitis media by 3 months of age.
Acute otitis media (Fig. 7) typically presents with ear pain or pulling/rubbing at the ear, pyrexia and irritability or restlessness, commonly with a history of upper respiratory tract infection. Other possible symptoms include nausea and vomiting, loss of appetite or poor feeding and hearing loss. However, a number of children with otitis media present non-specifically rather than with ear-related symptoms. Otoscopy reveals inflammation of the tympanic membrane with loss of normal landmarks, and as the disease progresses, bulging of the eardrum and ultimately perforation with purulent otorrhoea. However, single clinical features alone are not enough to diagnose acute otitis media. Instead, the diagnosis should be made by looking at a combination of symptoms and signs. The diagnostic criteria for acute otitis media requires all of the following three to be present:
Sudden onset of symptoms Signs of middle ear inflammation: e.g. erythema of the tympanic membrane, otalgia Signs of a middle ear effusion: e.g. bulging or immobile tympanic membrane, air fluid level behind the tympanic membrane, otorrhoea

Acute otitis media.
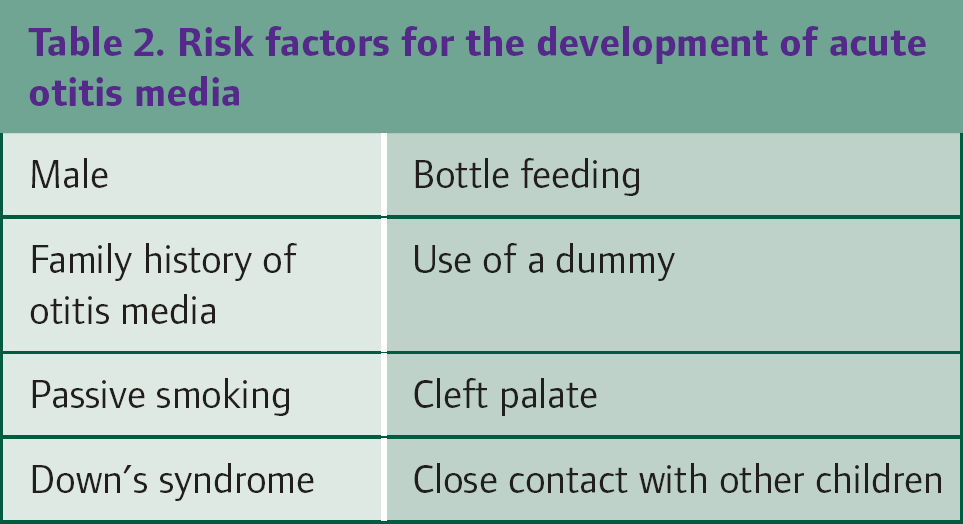
Over 90% of cases of acute otitis media are bacterial in origin, and in over 40% of viral causes, there is co-existent infection with bacteria. The main bacterial pathogens are Strep pneumoniae and Haemophilus influenzae, and occasionally Moraxella catarrhalis can be isolated. Less commonly found are Group A Strep, Staph aureus, Mycoplasma pneumoniae, Chlamydia pneumoniae and Chlamydia trachomatis. Associated viruses include respiratory syncitial virus (RSV), parainfluenzae, influenza virus, rhinovirus and enterovirus. Table 2 shows other factors that have been shown to be associated with the development of acute otitis media.
Risk factors for the development of acute otitis media
Despite the frequency of a bacterial aetiology in otitis media, the prescribing of antibiotics remains a contentious issue. This is because acute otitis media is usually self-limiting, rarely has a poor outcome and the use of antibiotics is associated with side effects and individual and community bacterial resistance. About 80% of episodes of acute otitis media will resolve within three days without antibiotics. In one trial of over 300 children, half were treated immediately with antibiotics and the other half were given a prescription for a delayed antibiotic to be collected at 72 hours if the child had not improved. Immediate antibiotics provided symptomatic benefit mainly after the first 24 hours, when symptoms were already resolving. However, they also increased the incidence of diarrhoea by 10%. In the group with a delayed prescription, only 24% actually used antibiotics. Most guidelines reflect this scenario and state that antibiotics should not be routinely prescribed as initial treatment in acute otitis media. Instead, adequate analgesia, for which there is some evidence that non-steroidal anti-inflammatories are better than paracetamol, together with watchful waiting is a preferred treatment strategy. The use of a delayed prescription is an acceptable alternative.
In July 2008, NICE published guidance on antibiotic prescribing in respiratory tract infections, including acute otitis media. This guidance states that at first presentation to primary care, in addition to history and examination, the patient's or parent's/carer's concerns and expectations regarding antibiotics should be addressed. Then one of three strategies can be agreed — no prescribing, delayed prescribing or immediate prescribing. When concluding no or delayed prescribing, reassurance should be given that antibiotics are not immediately necessary as they make little difference to symptoms and may have side effects such as diarrhoea, vomiting or rash. Advice should then be given about when to use the delayed prescription, and about re-consulting if the symptoms worsen or are prolonged, including after the use of any delayed prescription.
The guidance also recommends that immediate prescribing should be considered for particular subgroups, depending on the severity of the infection. These groups are children under 2 years old with bilateral acute otitis media, and children with otorrhoea and acute otitis media. Following the agreed treatment strategy, all patients should be informed of the usual natural history of the illness and that the average total illness length in acute otitis media is 4 days.
It is suggested that the first-line antibiotic is amoxicillin, or if the patient is penicillin-allergic, erythromycin or clarithromycin (better tolerated and twice daily dosing). A 5-day course is recommended. There is no evidence to demonstrate any benefit from decongestants, mucolytics or antihistamines, and given the increased risk of side effects, these should not be prescribed for children with acute otitis media.
Box 1 lists the complications of otitis media. Hearing loss as a result of acute otitis media is a transient conductive deafness. This occurs due to the middle ear effusion. This is usually only mild to moderate in severity, but hearing returns to normal when the effusion resolves. Permanent hearing loss can occur as a result of recurrent acute or chronic inflammation.
There are various possible outcomes from a perforated tympanic membrane — healing, resolution of acute otitis media (AOM) but persistence of perforation and persistence of both the AOM and the perforation (chronic suppurative otitis media). Most perforations spontaneously heal within 2 weeks. Therefore, a review of the patient should be planned for this time frame. If the perforation has not healed, the child should be monitored closely for any worsening of symptoms. Refer to an ear, nose and throat surgeon if symptoms worsen or if there is a persistent defect at 6 weeks.
Disturbance of balance and motor function relates to the presence of a middle ear effusion. The most common of the serious complications, mastoiditis, occurs in less than 1:1000 cases of acute otitis media not treated with antibiotics.
Recurrent otitis media
This is defined as three or more episodes of otitis media in 6 months, with complete resolution of symptoms between attacks. There may be a persistent effusion in the middle ear, which facilitates the growth of bacteria. In patients with recurrent acute otitis media, other foci for infection, such as sinusitis, and immune deficiency should be considered. Long-term antibiotic prophylaxis has been shown to prevent recurrences, although there is little evidence for which antibiotic to use or how long it should be used for. Most commonly, antibiotics are used for a period of 6 months. Recurrent otitis media warrants referral to ENT for review and planning of further management.
Chronic suppurative otitis media
In chronic suppurative otitis media, the middle ear infection persists, and there is continuation of a mucopurulent discharge, which may be bloodstained. There is also a conductive hearing loss. Pain is not usually a feature, and its presence should raise suspicion of a more invasive intracranial pathology. The most commonly isolated bacteria are Pseudomonas aeruginosa, Staph aureus and Proteus species.
There are two types of chronic suppurative otitis media, and they are defined based upon the location of the perforation. In tubotympanic, or ‘safe’ disease, the perforation is located in the pars tensa of the tympanic membrane (Fig. 8). In atticoantral, or ‘unsafe’ disease, the perforation is located in the pars flaccida of the tympanic membrane, and it may indicate the presence of a cholesteatoma (Fig. 9).
Large perforation of pars tensa.

Cholesteatoma
Initial management of safe chronic suppurative otitis media is similar to that of otitis externa. A swab is taken of the discharge, and it is important to bear in mind that when an individual has received multiple courses of antibiotics, the swab will always grow pseudomonas. Good aural toilet is essential in successful management of chronic suppurative otitis media, not least to allow topical treatments to adequately reach the middle ear.
Topical antibiotics are more effective than systemic antibiotics, plus they have lower incidence of side effects, particularly of antipseudomonal antibiotics. Topical aminoglycosides are potentially ototoxic, although sensorineural deafness due to topical antibiotic use in chronic secretory otitis media (CSOM) is rarely reported. Topical ofloxacin is also available, which is as effective without the potential ototoxicity. If medical treatment is ineffective, or if there is persistent hearing loss following effective treatment of the infection, referral to ENT is indicated for further management of the infection and consideration for tympanoplasty.
Complications of otitis media
Common
Hearing loss Otitis media with effusion Recurrent acute otitis media Perforation Otitis externa Disturbance of balance and motor function
Uncommon/serious
Mastoiditis Labyrinthitis Meningitis Intracranial sepsis Facial nerve palsy
In unsafe chronic suppurative otitis media, there may be a cholesteatoma developing in the pars flaccida, which may lead to local destruction of bone. A cholesteatoma is the presence of squamous epithelium in the middle ear cavity. This occurs either due to retraction of the tympanic membrane or due to migration of squamous cells from the tympanic membrane. The danger arises from expansion causing damage to dura, the lateral sinus, the facial nerve and the semicircular canals. A cholesteatoma presents as an offensive discharge, unresponsive to antibiotic therapy, and hearing loss. Other symptoms may include vertigo, headache, facial nerve palsy, cerebral abscess formation and cerebellopontine angle syndrome. As cholesteatomas may be fatal, they should be referred to ENT for aggressive treatment. In established cholesteatoma, mastoidectomy is almost invariably necessary, following which the ear should be dry and trouble-free.
Glue ear
Following acute otitis media, a non-infected middle ear effusion persists at 1 month in 50% of cases, 2 months in 20% of cases and 3 months in 10% of cases. When it persists more than 3 months, it is known as otitis media with effusion, chronic serous or suppurative otitis media or glue ear. It is considered by many to be part of the same disease as acute otitis media and the risk factors for the development of acute otitis media, as shown in Table 2, are the same for the development of otitis media with effusion. The most common symptom is hearing loss.
In an adult, chronic serous otitis media, i.e. the presence of a unilateral middle ear effusion for more than 3 months, has to be assumed to be due to a nasopharyngeal tumour until proven otherwise. Refer for urgent ENT review. However, in children it is much more common and benign in nature.
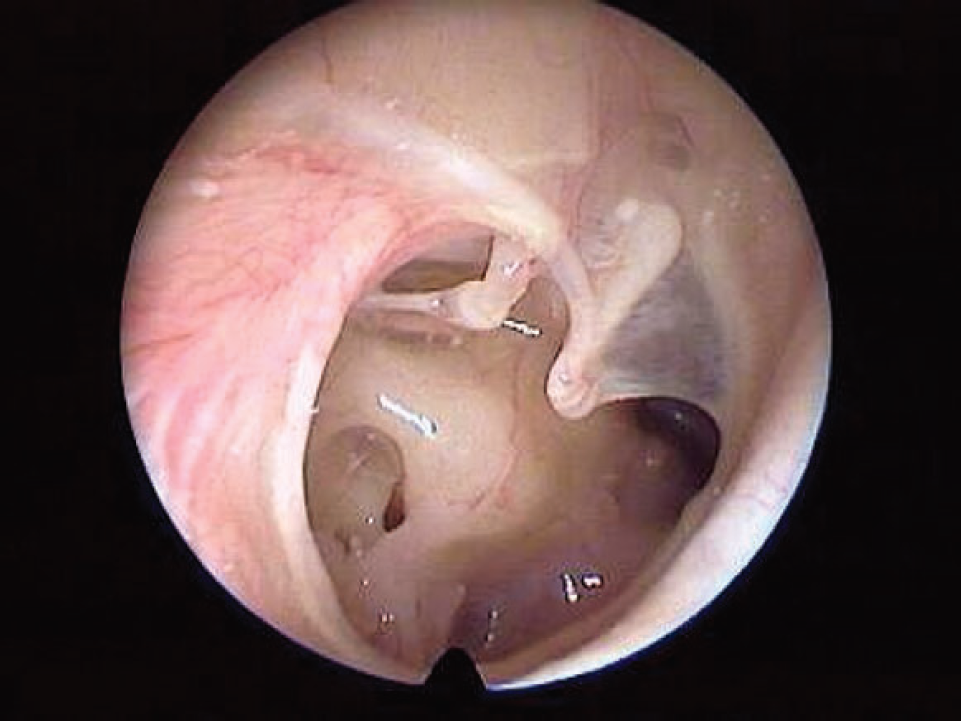
Chronic secretory otitis media or glue ear is the most common cause of hearing loss in childhood. It is important to detect as it can cause speech and language delay, behavioural difficulties and poor educational progress (Box 2). Eustachian tube dysfunction or obstruction, e.g. due to tonsillar hyperplasia, and recurrent throat or ear infections are implicated. Examination reveals a dull, retracted drum, with a fluid level and/or air bubbles behind the drum (Fig. 10). Audiometry shows a conductive hearing loss, and tympanometry shows a flat tympanogram due to the immobile tympanic membrane.

Chronic secretory otitis media.
Children under the age of 3, with persistent bilateral otitis media with effusion and hearing loss of 25 dB or less but no speech and language, development or behavioural problems can be safely managed with watchful waiting. However, the child should undergo audiometry to exclude a more serious degree of hearing loss.
Indications for assessment of children for glue ear
Poor listening skills Indistinct speech Delayed language development Inattention Behaviour problems Hearing fluctuation Recurrent ear infections Recurrent upper respiratory tract infections Balance problems and clumsiness Poor educational progress
Children with persistent bilateral otitis media with effusion who are above 3 years old or who have speech and language, development or behavioural problems should be referred to ENT for consideration of surgical intervention, in the form of grommets. If surgery is contraindicated or not acceptable, these children should be offered hearing aids. There is no evidence for the use of decongestants, antihistamines, mucolytics or antibiotics. The function of grommets is to ventilate the middle ear rather than draining it. They therefore replace the function of a blocked eustachian tube. They typically spontaneously extrude after a period of 6–18 months. Following expulsion, the tympanic membrane heals and there is often calcification of the drum at this site. Reinsertion of grommets is required in a minority of cases. Grommet insertion is not a contraindication to swimming — it does not increase the frequency of acute otitis media.
There is a sharp decline in the prevalence of otitis media with effusion after 7 years of age, which reflects improved eustachian tube function and maturation of the immune system. Treatment is aimed at reducing the impact of symptoms until natural resolution occurs.
Key points
Antibiotics are not routinely indicated as initial treatment in acute otitis media Delayed prescriptions are a useful alternative treatment option, and the antibiotics are only used in a minority of cases Recurrent otitis media warrants referral to ENT and benefits from long-term antibiotics Perforation of the pars tensa of the tympanic membrane is a relatively benign disease and is managed initially as for otitis externa Perforation of the pars flaccida of the tympanic membrane is potentially fatal and needs referral to ENT Unilateral persistent middle ear effusion in an adult is due to a nasopharyngeal tumour until proved otherwise The treatment of glue ear is aimed at reducing the impact of symptoms until natural resolution occurs Swimming with grommets is not a problem.