
Abstract
The hormonal, physiological and physical changes that occur during pregnancy can lead to a number of skin conditions being exacerbated, occurring for the first time or appearing in an altered form. In addition to this, there are a number of systemic infections in which skin symptoms or rash may be the presenting complaint. It is important to be able to distinguish between those rashes which represent potential complications for the pregnant woman and developing foetus and those which do not. Where the diagnosis is unclear, it is useful to have a management strategy to exclude serious causes.
The GP curriculum and rashes in pregnancy
Dealing with problems and potential infections in pregnancy comes mainly under curriculum heading 10.1. A GP should demonstrate knowledge of women's health problems, conditions and diseases. This includes the ability to
Describe how practice management issues impact on the provision of care to women including choice and availability of female doctors Maintain patient records that are accurate, facilitate continuity of care Describe the importance of informing patients of results of screening and ensuring follow-up Manage normal pregnancy and pregnancy problems including intrauterine infection, intrauterine death and foetal abnormality
At the beginning of pregnancy
It is important that specific enquiries are made at the booking visit as to whether the woman has had chickenpox and/or shingles in the past. If there is no clear history of previous infection, she must be advised to contact her GP urgently if she has contact with chickenpox or shingles or develops a chickenpox-like rash. As there are a number of infections which may present with skin signs, all pregnant women should be advised to inform their midwife or GP if they develop a rash or have contact with anyone who has a rash.
Exposure to rash illness in pregnancy
Consultations or requests for advice when a pregnant woman has had contact with a rash illness are not uncommon. It is useful to have a management plan for this situation to ensure post-exposure prophylaxis is given where required (see Algorithm 1).

Pregnant patient who has been exposed to a person with rash illness.
Presentation with a rash in pregnancy
The differential diagnosis of rash in pregnancy includes all causes of a rash in a non-pregnant patient. Consider infectious causes (including rubella, parvovirus B19, varicella zoster, measles, enteroviruses and streptococcus); common skin conditions (such as eczema, urticaria and contact dermatitis) and pregnancy-related conditions (including pemphigoid gestationis and polymorphic eruption of pregnancy). Algorithm 2 summarizes investigation of rashes in pregnancy.
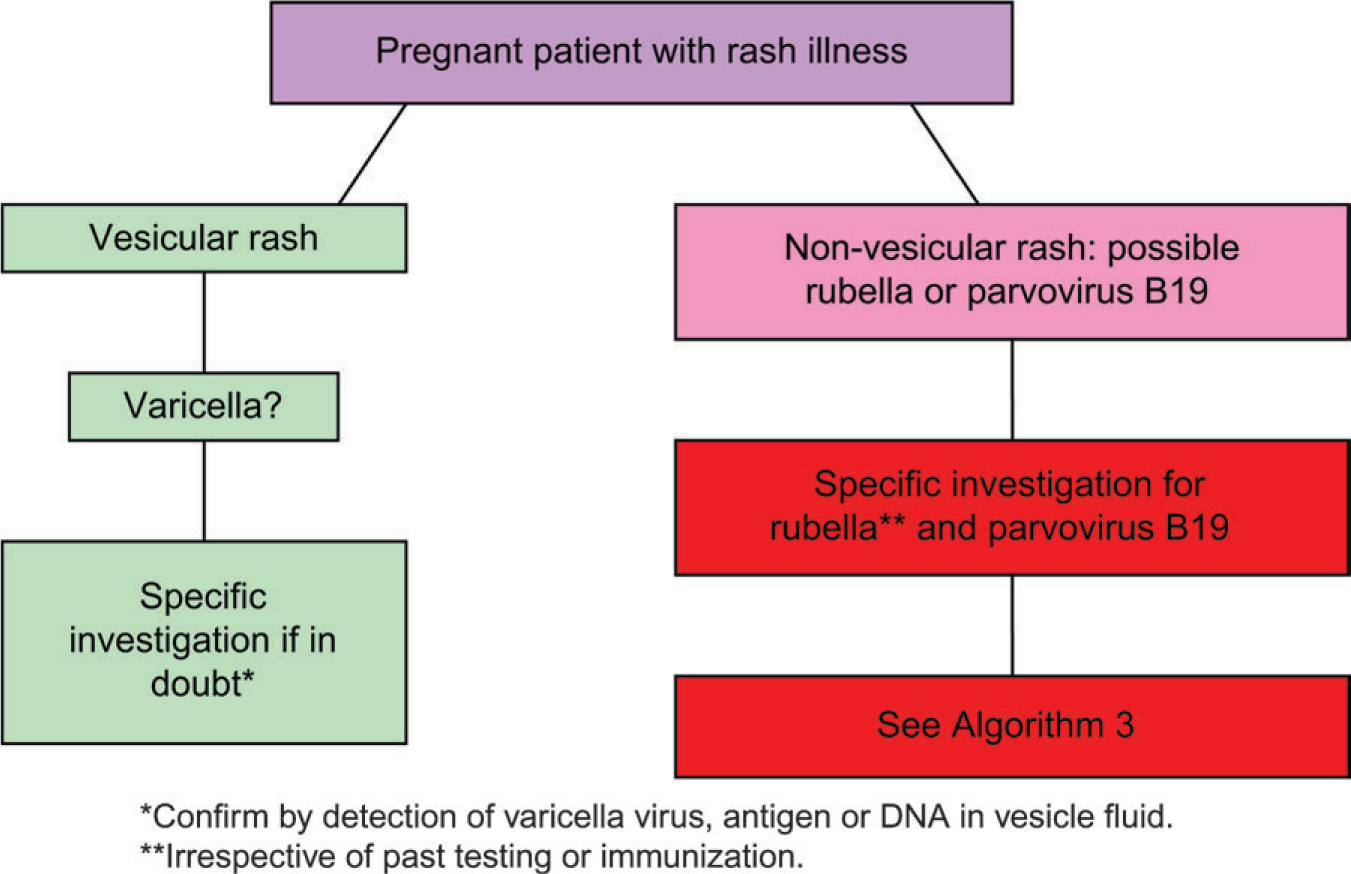
Investigation of a pregnant woman with rash illness.
Rubella
Key features
Rubella is rare in the UK, in part due to the childhood vaccination programme. As a result, only 1–2% of adult women are susceptible. However, 50% of mothers infected with rubella may be asymptomatic. Asymptomatic reinfection can also occur in those who have been vaccinated so always send serology if a rash is compatible with rubella.
Rubella presents with fever, lymphadenopathy (including suboccipital nodes) and a pink maculopapular rash (see Fig. 1) lasting approximately 3 days. The incubation period is 14–21 days, with the infected person being infectious from 7 days before to 10 days after the rash appears.

Rubella.
Risk to the foetus
Risk to the foetus is dependent on gestation, with risk of transmission and severity of effect on the foetus both being highest in the first trimester (Table 1). The adverse foetal effects include cataracts, deafness, cerebral palsy, microcephaly and microphthalmia.
Risk to the foetus of transmission and adverse outcome for pregnant women with rubella infection

Management
Where a patient has been in contact with a non-vesicular rash (which may be rubella), assess as in Algorithms 1 and 3. In cases of a pregnant patient with a non-specific, non-vesicular rash or in suspected rubella infection, send serology as per Algorithm 3. If IgM and IgG are not detected in the first test, recheck serology 1 month later.
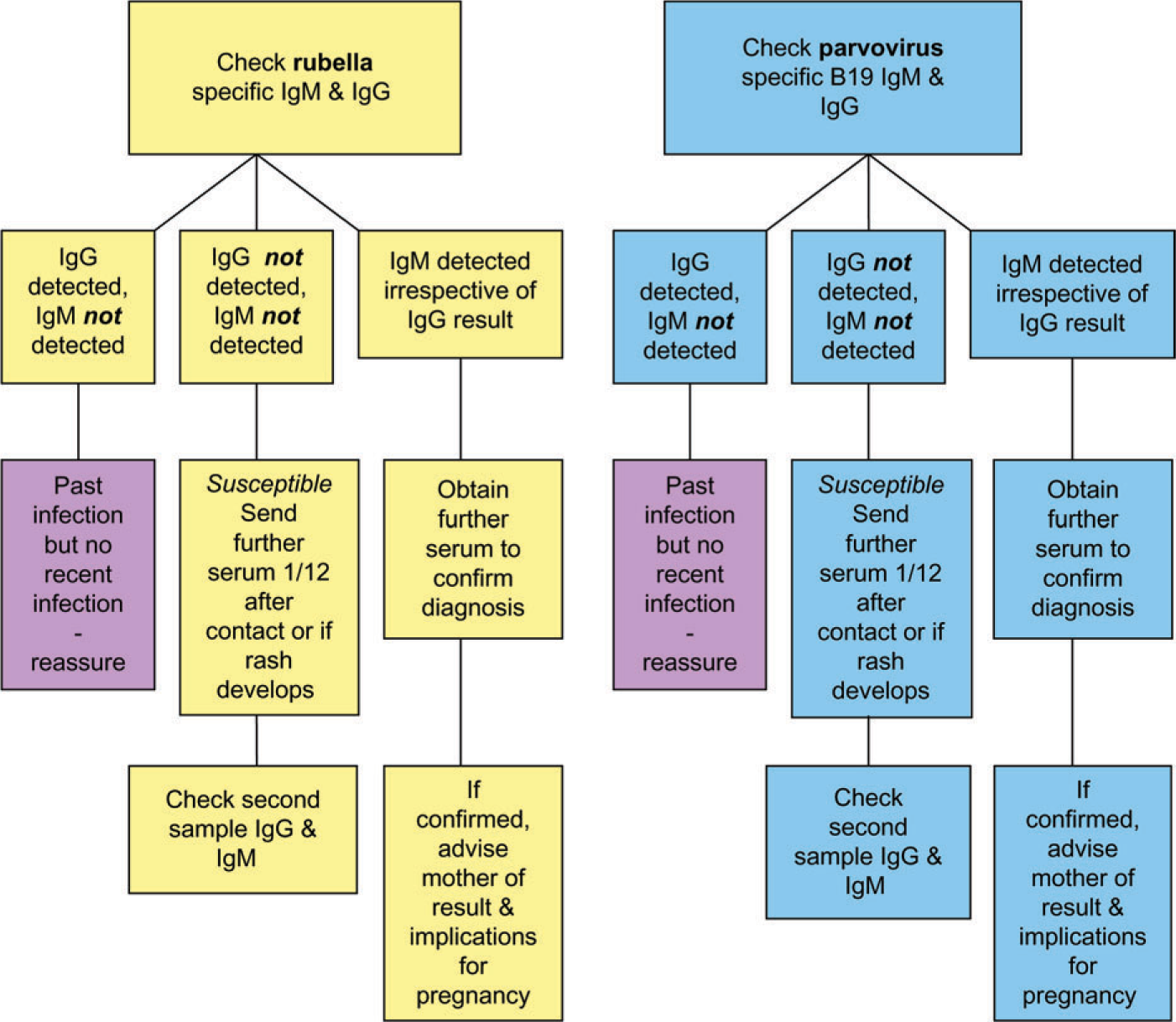
Specific investigation following significant exposure to a non-vesicular rash or with a rash suggestive of possible rubella/parvovirus B19.
In cases of proven infection, refer the patient for specialist obstetric care. Women infected before 20-week gestation may be offered termination of pregnancy after investigation and counselling regarding the risks to the foetus.
Parvovirus B19
Key features
Approximately 50% of young women in the UK are not immune to parvovirus B19 and the risk of infection in pregnancy is roughly 1 in 400. The risk of transmission from a child with Fifth disease (‘slapped cheek’, see Fig. 2) to a non-immune mother is also approximately 50%.

Parvovirus B19 ‘slapped’ cheek.
Fifth disease presents with a febrile illness, often with tenderness of the joints and arthritis, especially of the hands, wrists and knees. A fine'lace-like’ rash is often seen over the trunk and extremities (see Fig. 3). The arthralgia usually lasts for 1 or 2 weeks but 1 in 10 of those affected have continuing symptoms for several months. The incubation period is between 13 and 18 days and the patient is infectious from 10 days before the rash appears to the day of rash onset.

Parvovirus B19 rash with ‘lacy’ appearance.
Risk to the foetus
Again, risk to the foetus from parvo virus infection is dependent on gestation; however, unlike with rubella, the probability of transmission increases with gestation (before 4 weeks the risk is 0%, increasing to 15% between 5 and 16 weeks and rising to anything from 20 to 70% above 16 weeks). No treatment is known to prevent transmission.
If infection occurs before 20-week gestation, there is a 9% increase in the rate of miscarriage. Three per cent of affected foetuses (14–56 cases per year in the UK) go on to develop foetal hydrops, of which 50% die. Infections that do not cause miscarriage or foetal hydrops are not linked to any long-term effects on the pregnancy outcome.
Management
See Algorithm 1 for management of pregnant women who have been in contact with a non-vesicular rash. If the patient presents with a rash and serology confirms parvovirus B19 infection, refer for specialist care. This will usually involve
Serial ultrasound scan (USS) commenced 4-weeks post-onset of illness (or post-seroconversion) and repeated at one to two weekly intervals up to 30-weeks gestation If USS findings are consistent with hydrops foetalis, the mother is referred to a Regional Fetal Medicine Unit for consideration of intrauterine transfusion (which has been shown to reduce the chance of foetal death) If no foetal abnormality is detected at or later than 30 weeks, the pregnancy is unlikely to be affected.
Chickenpox (varicella zoster)
Key features
Reported contact with chickenpox in pregnancy is common. The incubation period is between 14 and 21 days. An affected person is infectious from 2 days before the appearance of the rash (see Fig. 4) until all the vesicles (see Fig. 5) have crusted over.

Chickenpox.

Chickenpox vesicles.
If the exposed mother has a definite history of chickenpox, there is no risk to her or the foetus. In the absence of a clear recollection of chickenpox, send serum to check the mother's immunity. Around 80% of adults will have antibodies from previous silent infection.
Risks to the mother
Chickenpox infection complicates 3 in every 1000 pregnancies. The risk of developing chickenpox-related pneumonia is up to 10% in pregnant women, severity increasing with advancing gestation. The mortality associated with maternal complications is estimated to be 1 per 1000 infections in pregnancy.
Effects on the foetus and newborn
Chickenpox transmission rates to the foetus increase as pregnancy progresses, from 5–10% before 28 weeks to approximately 50% above 36 weeks. Infection causes different presentations depending on the gestation:
<20 weeks
Increased risk of miscarriage has been reported in some sources 1–2% risk of foetal varicella syndrome (FVS) — dermatomal skin scarring, eye defects, hypoplasia of the limbs and microcephaly 20–37 weeks
Intrauterine infection with chickenpox in early childhood FVS has been reported following maternal infection up to 28 weeks but is thought to be extremely rare Rash developing 1 week before to 1 week after delivery
The baby may require VZ-Ig, with or without aciclovir Seek specialist advice The baby is particularly vulnerable if the onset of the rash is within 4 days before to 2 days after delivery (20% risk of overwhelming neonatal infection)
Management
One element is to recognize those ‘at-risk’ post-exposure. VZ-Ig needs to be given to the mother and/or baby ideally within 10 days to modify disease severity and reduce mortality. The baby is particularly at risk under the following circumstances:
The mother develops chickenpox from 7 days before to 7 days after delivery Exposure to chickenpox less than 7 days after delivery with a non-immune mother Immune mother but potential for inadequate transfer of maternal antibodies, for example:
Birth before 28-week gestation Birth weight less than 1 kg Repeated blood sampling and replacement with packed red cell infusions Neonatal intensive care unit or prolonged special care baby unit requirement
Consider referral for urgent specialist assessment if
Fever persisting or rash continues cropping for more than 6 days Arrange admission if
Chest symptoms Neurological symptoms (other than headache) Haemorrhagic rash, bleeding elsewhere or severe disease (dense rash and/or multiple mucosal lesions) Significantly immunosuppressed (e.g. HIV infection) Consider admission if
Pregnancy is approaching term Poor obstetric history Smoker Known chronic lung disease Poor social circumstances These babies can be given VZ-Ig without antibody testing but testing is still advisable where possible It is important to note that the duration of protection from a dose VZ-Ig is limited. If further exposure occurs more than 3 weeks after the first dose and mother-baby are still at risk, a second dose may be given (although antibody status should be checked beforehand). A further element is the management of a pregnant woman who develops chickenpox. If a woman presents within 24 hours of the rash developing and is over 20-week gestation
Give aciclovir 800 mg five times daily or valaciclovir 1 g three times daily for 1 week. Note: the use of aciclovir before 20-week gestation is not known to be harmful but British National Formulary states ‘…use when potential benefit outweighs risk’. If infection develops before 28 weeks, refer for detailed foetal USS 5 weeks after onset to look for signs of FVS Monitor daily and be aware of criteria for admission (see Box 1) Advise patient to avoid those at risk of developing severe chickenpox, particularly other pregnant women and neonates
Criteria for admission with chickenpox in pregnancy
Measles
Key features
Measles is rare in the UK since incorporation of measles, mumps and rubella into the routine childhood vaccination schedule. It presents with coryzal symptoms, lymphadenopathy, conjunctivitis and a disseminated maculopapular rash (see Fig. 6), which becomes confluent.

Measles with Koplik spots.
Risks to the mother
Not exclusively to pregnancy, measles can be complicated by pneumonia, otitis media and encephalitis.
Risk to the foetus
Maternal infection during pregnancy can lead to intrauterine death and preterm delivery but is not associated with congenital infection or other abnormality.
Cytomegalovirus
In the UK, cytomegalovirus is actually a more common cause of birth defects than rubella (5 in 1000 live births), and 10% of those affected develop a significant handicap. The developing foetus is most vulnerable when maternal infection occurs in early pregnancy.
There is no effective prevention strategy. The diagnosis is often made retrospectively (after foetal anomalies noted) as maternal infection may be asymptomatic or present as a mild flu-like illness, most often without a rash.
Other rash infections
There are some viral infections, including Epstein-Barr virus, which may cause a non-specific viral exanthem and are not known to affect the foetus. Enteroviruses, including Coxsackie viruses A and B, echovirus and enterovirus 68–71 may cause diseases such as hand, foot and mouth, which is associated with intrauterine growth retardation or spontaneous abortion if maternal infection occurs in the first trimester. Some enteroviruses can also cause severe neonatal infection so prophylactic immunoglobulin may sometimes be required. If in doubt, seek specialist advice.
Skin conditions exclusive to pregnancy
Polymorphic eruption of pregnancy
Also known as pruritic urticarial papules and plaques of pregnancy (PUPPP), polymorphic eruption of pregnancy is an itchy rash that starts in the abdominal stretch marks during the last 3 months of pregnancy (see Fig. 7). Theories suggest that it develops as a type of ‘allergic’ response to the stretching of skin during enlargement of the fundus. Observations supporting this ‘stretch theory’ are that it is most common in first pregnancies, usually starts near to the umbilicus and most frequently presents in the last 5 weeks of gestation.

Pruritic urticarial papules and plaques (PUPPP) of pregnancy in abdominal striae.
Treatment is symptomatic with emollients, topical steroids and anti-histamines until delivery. Delivery ‘cures’ the problem. Recurrence in a future pregnancy is uncommon and tends to be much less severe.
The baby is occasionally born with a milder version of the same rash on the face but this quickly fades. It is not associated with any adverse foetal outcomes.
Pemphigoid gestationis
This is a rare autoimmune condition which classically occurs during the second and third trimesters. An itchy, blistering rash initially develops around the umbilicus (see Fig. 8) before spreading to the rest of the body (but not usually affecting the head, palmar-plantar surfaces or mucous membranes). This condition is also known as herpes gestationis but does not have any association with the herpes viruses.

Pemphigus gestationis starting in classical distribution.
It is confirmed after skin biopsy and direct immunofluorescence. Treatment is dependent on severity; topical or oral steroids may be required in conjunction with anti-histamines (to treat itch).
Although complications are rare, these can include secondary infection (with resultant scarring), premature delivery and transient blistering on the infant (which resolves at 3–4 months of age with clearance of maternal antibodies).
In some women, it may occur for the duration of their pregnancy. In this case, the rash may temporarily lessen or spontaneously resolve towards the end of the pregnancy but 75–80% of women will experience a flare around the time of delivery. In almost all cases, the rash resolves days after giving birth (at which point treatment can be tapered off and stopped). For an unfortunate minority, the disease remains active for months or years afterwards. Once a woman has had pemphigoid gestationis, the start of the menstrual cycle, use of oral contraceptives or further pregnancies may cause flare-ups.
Key points
Consultations with exposure to or development of rashes in pregnancy are common If an infectious cause is considered, send serology and seek advice The likelihood of parvovirus infection in pregnancy is higher than that of chickenpox Maternal risks of chickenpox in pregnancy are greatest at later gestations and close monitoring is required Risk of FVS development following maternal infection is relatively low (less than 1%) Skin rashes exclusive to pregnancy are uncommon but may require specialist input