
Abstract
This paper describes the role of primary care clinicians in the management of people with psychosis. The paper uses the term ‘psychosis’ in the same way that severe mental illness is used in the Quality and Outcome Framework to mean those people who suffer from schizophrenia or bipolar disorder. The paper will cover some epidemiological characteristics of psychosis, features of people with acute psychosis, features of chronic psychosis and finally describe briefly changes to the Mental Health Act 2007 and the potential for these changes to affect the practice of medicine in primary care.
The GP curriculum and psychosis
This paper is compatible with the RCGP Curriculum Statement on Mental health (Curriculum Statement 13).
Describe specific interventions and guidelines for individual conditions, using
where appropriate best practice as described in the Scottish Intercollegiate
Guidelines Network or National Institute of Clinical Excellence guidelines Describe the varied ways that young people who are developing a first episode
of psychosis present Describe how to access health and social care organizations, both voluntary and
statutory, that are an essential component of managing people with mental
health problems Describe when it is appropriate to refer to and collaborate with the specialist
mental health services
Describe the concept of concordance that is particularly important in mental
health care Be able to present individuals with choices as to which intervention may work
best for themselves and understand that this ability to choose improves the
effectiveness of the intervention
Describe how to deal with the associated physical health problems of people
with mental health problems
Describe the extent and implications of stigma and social exclusion Demonstrate how to work in partnership with other agencies to secure
appropriate social interventions for individuals
Demonstrate sufficient knowledge of the current Mental Health Act to undertake
the responsibilities that this requires of general practitioners (GPs)
Epidemiology
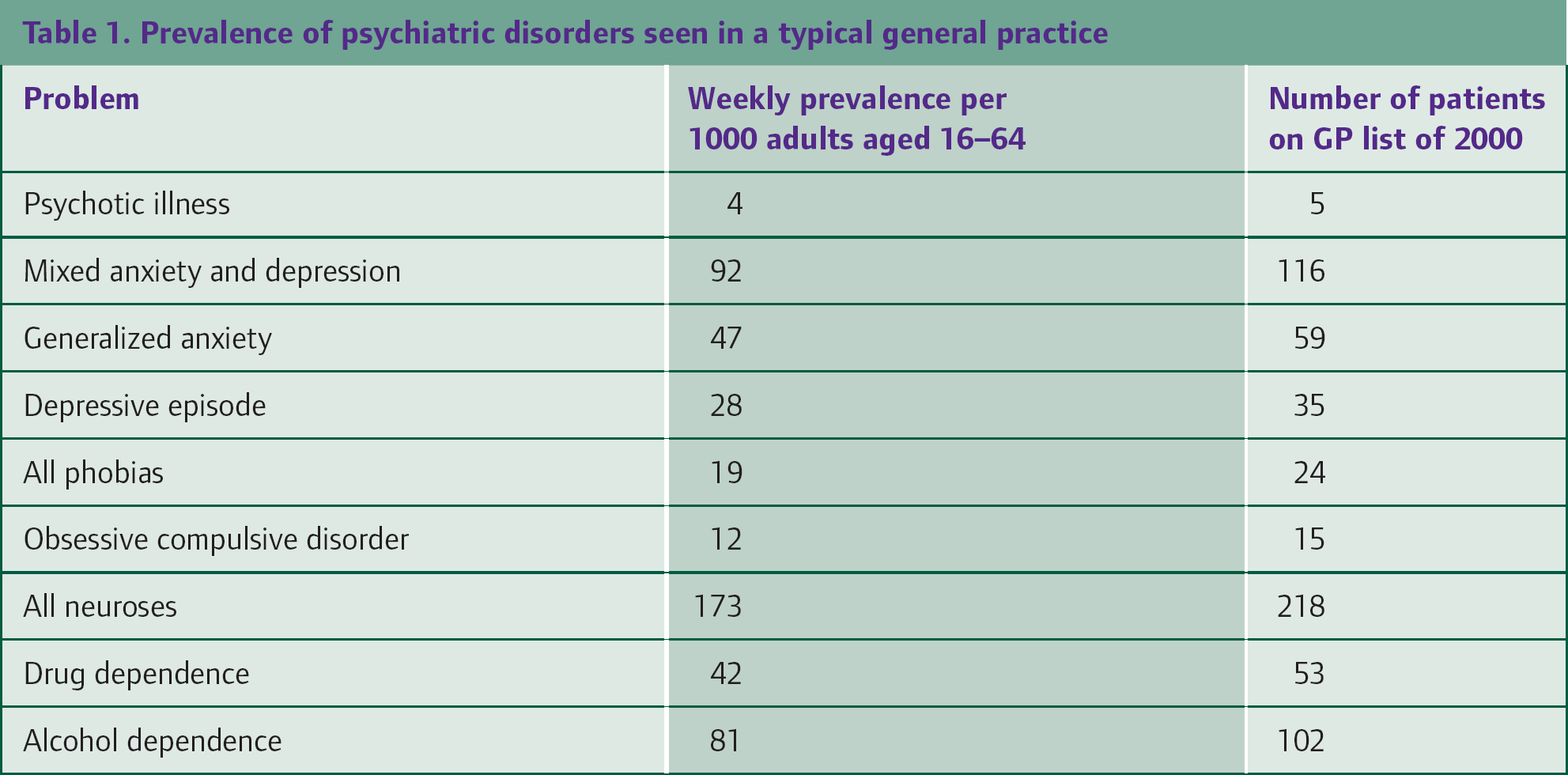
Table 1 shows the relative prevalence of mental health disorders in the community and the likely number of patients seen in an average practice with a list size of 2000. Although the absolute numbers of patients with psychosis are low, compared to depression or anxiety, their relative disability in terms of morbidity and mortality and social exclusion is great. Huxley and Thornicroft (2003) described some of the consequences of social exclusion (see Box 1).
Prevalence of psychiatric disorders seen in a typical general practice
The effect of this increased need on primary care services is reflected in the increased consultation rate (Burns and Cohen, 1998), which is about 3 times greater than the norm. There is also a responsibility on primary care services to ensure that there is effective working between primary care and specialist mental health services so that every patient, where appropriate, has the opportunity to benefit from both primary care and specialist mental health care. At least 25% of people with severe and enduring mental illness are not in contact with specialist mental health trusts and that may reduce their opportunity to benefit from the specialist care and knowledge that these teams can provide (Burns and Cohen, 1998).
Finally, it is worth recording that a recent review by Fearon et al. (2006) assessed the new diagnosis of psychosis in different ethnic groups: they found that Afro-Caribbeans and Black Africans were particularly more at risk than White British people. This too will have an impact on how primary care responds to people with psychosis, if the practice is located in an area with a high proportion of Afro-Caribbeans or Black Africans.
Consequences of social exclusion
The employment level of psychiatric patient populations rarely reaches more
than 10%, and when working they work fewer hours and earn only two-thirds of
the national average hourly rate People with mental disorders constitute 39% of all claimants of Severe
Disablement Allowance and 34% of Incapacity Benefit claimants, according to
recent figures Studies have found that about half the patients in contact with a community
mental health service in England were not receiving the full amount of
welfare benefits to which they were entitled
Acute psychosis
For a GP, managing a patient in an acute psychotic episode is both difficult and time consuming. Acute psychotic episodes are uncommon, but present a number of problems to the GP that are important to manage effectively. It is likely that a GP will only see a new psychotic episode perhaps once in every 2 years, and a first-ever episode of psychosis (FEP) once every 5 years in an average practice (Sainsbury Centre for Mental Health, 2004).
Features of acute psychosis
Psychosis usually emerges when people are young: 80% of FEP emerges between the ages of 16 and 30 years; the average age is about 22, slightly younger in males. Audits in the West Midlands have shown that 75% of people experiencing their first episode live with either parents or spouse, 29% have parenting roles and 41% are employed or in full-time education.
Shiers and Lester (2008) describe some of the features of acute psychosis. A prodromal phase heralds the onset of psychosis. This can last several months during which there may be varying psychological and social disturbances without clear-cut psychotic symptoms. Psychosis rarely presents with a neat symptom parcel. It is important to look for evidence of poor personal hygiene, delusional or bewildered mood, abstract or vague speech and outbursts of anger or irritation. Positive and negative symptoms are rarely volunteered spontaneously and may need to be actively sought. If you suspect the person may be developing a psychosis, ask about changes in social functioning, for example, problems in relationships with friends and family, problems with cognition, mood or thought content, suicidal ideas and drug misuse.
Perhaps, above all, where there are concerns, it is important to keep an ‘active watching brief’. This means ensuring that a line of communication, and offer of care, is maintained wherever possible through follow-up appointments, home visits or telephone calls.
In the audit in the West Midlands, between 60% and 80% of patients with psychosis presented through family members seeking help from their G P. This emphasizes the role of the GP in being sensitive to concerns being raised and the difficulty of providing care both to the family members and the patients themselves. Engaging patients may be difficult and arranging an appropriate referral which initially may be declined can also be frustrating. Many specialist mental health trusts now provide an Early Onset team whose role is to identify and manage the early stages of psychosis. Contact with this team by the GP is important so that an appropriate level of intervention to the patient and their family/carers is provided.
Duration of untreated psychosis
An important consideration is the duration of untreated psychosis (DUP). This is the period of time between the onset of psychotic symptoms and initiation of treatment. The reason why this is important is that the longer the DUP, the more likely the patient is to have poor pre-morbid functioning, poor psychosocial contacts, insidious presentations with predominantly negative symptoms and is more likely to be male.
Once the treatment has begun, those with a longer DUP are more likely to have a poorer functional outcome, poorer symptomatic outcomes, increasing behavioural difficulties, increasing family disturbance and more likely to have life-threatening behaviour. Birchwood et al. (1998) identified a ‘critical period’ early in the illness when therapeutic intervention and life experiences can have important long-term consequences; clinical progress in the first 2 years of treatment strongly predicts outcomes at 15 years (Harrison et al., 2001).
Early identification, and subsequent early treatment, is likely therefore to lead to improved long-term outcomes, as well as making it less likely for a patient to be compulsorily admitted to hospital under the Mental Health Act. In the past, compulsory admission under the Mental Health Act had usually been the patient's first contact with mental health services; the link between compulsion and the confusion associated with the mental illness may explain why such a significant number (at least 25%) chose not to be in contact with specialist services.
Management of the acute psychosis by the GP can be summarized as
To know how early the first episode of psychosis presents — it is usually a
family member/carer who presents rather than the patient themselves To know the early signs of psychosis To know how to contact the early onset team in the specialist mental health
trust, so that an early opinion can be sought To continue to provide support to both the patient and the family
member/carer as treatment continues over time
The Mental Health Act 2007
The Mental Health Act has recently been amended, and the changes enacted on 1 November 2008. The major change to the 1983 Act (which preceded the 2007 Act) is the introduction of a Community Treatment Order. Other changes less significant to primary care include the introduction of an Approved Mental Health Professional (AMHP) to replace the Approved Social Worker (ASW) and that the Responsible Medical Officer (renamed the Clinical Supervisor) may not necessarily need to be a psychiatrist, but for appropriate patients could be a psychologist. These changes all relate to the Act as it applies to England and Wales. The three sections that GPs are most familiar with are unchanged — Section 2, Section 3 and Section 4. The emergency section to be used by the police, Section 136, is also unchanged. The other changes that have been introduced are unlikely to have a significant impact on primary care and the role of GPs.
Sections of the Mental Health Act
There are four sections of the MHA (1983) which the GP and primary care clinician need to be aware of
Section 2: Admission for assessment for up to 28 days Section 3: Admission for treatment for up to 6 months in the first
instance Section 4: Admission as an emergency for up to 72 hours in the first
instance Section 136: The section which a police officer can enact to detain a
person, who is in a public place, that they suspect may have a mental health
disorder and who in their opinion is a danger to themselves or others. The
section also allows the transfer of that individual to a ‘place of safety,’
for assessment.
Section 2
Section 2 is intended for the admission of a patient with a mental disorder for whom the diagnosis is not known or for whom a period of assessment is necessary. The period of detention can be up to 28 days. Patients must represent a danger to themselves (either through self-injury or through self-negligence) or to others. The process for admission is that an application is made either by an AMHP appointed by social services (usually the duty social worker) or ‘nearest relative’. The application is supported by two medical recommendations. The medical recommendation for admission should precede or be contemporaneous with the application from the AMHP to the managers of the Mental Health Trust.
Section 2 requires that two doctors sign the medical assessment. At least one doctor should be approved as having special experience of managing mental illness and the Mental Health Act. The need for such a doctor is described in Section 12(2) of the Act, and the experience needed for the role is set out in guidance. A GP can be Section 12(2) approved if they have at least 3 years' experience as a principal and have had experience of managing compulsory admissions, with suitable references from at least one psychiatrist. The other doctor who signs the medical assessment should have previous knowledge of the patient, and it is usually this role that the GP fulfils. All psychiatric consultants are Section 12(2) approved as are most senior registrars.
Section 3
Section 3 is used to admit patients for compulsory treatment. It is used for patients in whom the diagnosis is already known. The section lasts in the first instance for 6 months, but thereafter can be renewed while the patient is still an inpatient for a further 12 months. The criteria for admission are the same as for section 2 — that patients are a danger to themselves or to others.
Section 4
Section 4 is the emergency admission process and can only be used when there is no possibility of obtaining a second medical recommendation. A single doctor can make a recommendation to an AMHP for compulsory admission for 72 hours. The application has to demonstrate, as it does for Section 2 or Section 3, that the patient is a risk to themselves or to others, it also has to demonstrate that the urgency of the admission precludes compliance with the safeguard of obtaining a second medical opinion.
A section 4 can be converted to a section 2 or 3 once the patient is on the ward. Section 4 is relatively unusual, as each Mental Health Trust should be providing a specialist on call to deal with such eventualities.
Supervised community treatment
Supervised Community Treatment (SCT) applies to patients who have been detained on Section 3 of the Act (not Section 2) or those who have been transferred from the criminal justice system (e.g. under sections 37, 48 or 51). There are specific criteria that must be applied for an individual to warrant SCT. The criteria broadly are that the individual must have a mental disorder and that there is appropriate treatment available. The clinical supervisor (was previously the Responsible Medical Officer) must determine if the patient meets the criteria and then seek agreement from the AMHP. The Mental Health Trust managers must liaise with the PCT and the Local Authority, to ensure that the services required are available prior to the patient leaving hospital.
SCT cannot be implemented directly from the community —there has to be an admission immediately prior to the community treatment being implemented. The SCT order may require that the patient resides at a specific address, makes themselves available for treatment or desists from specific actions/activities. The SCT order provides a power to the Clinical Supervisor to recall the patient to hospital if they become a danger to themselves or others, but there is no power if the patient fails to adhere to the other conditions. A patient that has been recalled, if detained for longer than 72 hours, must be referred to the Mental Health Tribunal for review.
The impact of this new section on primary care is unclear: the estimates are that there will be about 2000 new cases each year, but it is less clear as to how many will come off the section, so that there is some concern that the numbers will increase year on year. Secondary legislation has approved the Code of Practice, which describes, among other things, the role of the G P. The Code of Practice makes clear that patients who are being considered for community treatment should if at all possible be registered with a GP and that the GP is consulted at all times about the proposed community treatment order. Nevertheless, it remains unclear where clinical responsibility for a patient on SCT lies out of hours, an issue that is not clearly addressed by the Code of Practice.
Chronic psychosis
The role of the GP in caring for people with chronic psychosis depends in part on whether or not the patient wishes to remain in contact with specialist mental health services.
For patients who chose not to remain in contact with the specialist mental health team, the role of the GP is complicated. There has never been an intention that GPs can replace psychiatrists in their management of people with severe mental illness; psychiatrists and their community mental health teams have much more experience as well as access to services that will benefit their patients. So, for those patients who chose to not to remain in contact with a psychiatrist, the role of the GP must first be to ensure that the patient is making an informed choice. It is entirely appropriate to encourage at least an annual review of the patient by a psychiatrist and their team. It may be that this annual review would be sufficient to provide the expert overview that benefits the patient, without being unduly intrusive to the patient. Certainly, such continuing specialist review is recommended for other groups with long-term conditions such as diabetes or ischaemic heart disease. Effective communication with the mental health team can also provide a route to support the GP to care for a patient who refuses contact with a community mental health team, yet has continuing mental health needs. Such communication could be the regular meetings between mental health team and primary health care team, that is advocated in the Policy Implementation Guide for Community Mental Health Teams published by the Department of Health.
For patients who choose to remain in contact with specialist mental health services, the role of the GP is to manage the physical health needs of their patient and to ensure appropriate contact with the specialist mental health team.
The physical health needs of those with a severe mental illness are significant. The physical health of people with schizophrenia and bipolar affective disorder is significantly poorer than a comparative population without these conditions. The OPCS psychiatric morbidity survey (2000) found that 62% of those with psychosis reported a physical condition, compared to 42% of those without psychosis.
People with schizophrenia and bipolar disorder die more frequently than people without these disorders. The standardized mortality rate (SMR) was described in a paper by Harris and Barraclough (1998). They found that the SMR for respiratory disease in people with schizophrenia and bipolar disorder was 250, for infectious diseases was 500 and for cardiovascular disease was 250.
The Disability Rights Commission, now included as part of the Human Rights Commission, undertook a formal investigation into the physical health of people with mental illness. This review in 2005 represents the most up to date and complete analysis of the physical health needs of people with a severe and enduring mental illness. The findings are summarized in Box 2.
Schizophrenia and bipolar disorder co-morbidity
The reasons for these co-morbid conditions are complex and not just related to the use of specific medication. People with a severe mental illness tend to become excluded from society; they are less likely to be in employment, less likely to have family support and more likely to have accommodation problems. They are more mobile and tend to move towards areas of inner urban deprivation. With less money, poor opportunities and poor accommodation, the effects of poor nutrition predisposes towards obesity, which compounds their mental health problems.
A characteristic of the early stages of severe mental health problems is the increase in risk-taking behaviour; people are less likely to engage in safe sex and are more likely to use drugs and alcohol to mediate the unpleasant effects of their disorder. As a consequence, hepatitis C is up to 15 times more common and HIV up to 8 times as common as compared to the general population.
Nicotine acts on the dopaminergic receptors in the brain, also believed to be the site of the paranoid hallucinations characteristic of schizophrenia. It is this mechanism that attempts to explain the fact that 80–90% of people with schizophrenia smoke, whereas only 20–30% of people with bipolar disorder smoke. The consequence of such a large proportion of people smoking is clear in the effect on respiratory disease and cardiovascular disease.
Psychotropic medication clearly has an impact on some of the conditions described above. The new atypical antipsychotics are described as diabetogenic, but the mechanism is not clear. Certainly, the medication does cause an increase in body mass index (BMI) which itself is diabetogenic. However, the first descriptions of an increased proportion of people with schizophrenia who suffer from diabetes was published in the 1920s, even before the invention of standard antipsychotics, so another mechanism is thought to be partly involved. Antipsychotic medication also causes a prolongation of the QT interval in electrocardiograms, which can cause arrhythmias —further exacerbating a potential for cardiovascular disease. Finally, antipsychotics cause a rise in serum prolactin levels, which can cause further endocrine disturbances. The risks associated with lithium are well recognized, as is the need for the blood level to be kept within a therapeutic window.
Health promotion data for people with severe mental illness
Some characteristics of the health of people with psychosis were described by Burns and Kendrick in 1997. They found that 25% were obese (with BMI of over 30), 53% were smokers and 11% were hypertensive (with systolic blood pressure over 160 mmHg or diastolic blood pressure over 90 mmHg). There is no data on other aspects of health promotion, but some information on the frequency with which information is recorded (Burns and Cohen, 1998): smoking is recorded in about 23% of patient records, a blood pressure within the previous year in 38%, a cervical smear in 28%, mammography in 8%, alcohol use in 20%, BMI in 27% and cholesterol in only 2.5%. It should be noted that these studies preceded the introduction of the Quality and Outcome Framework (QOF) domain for Mental Health.
QOF mental health domain
Table 2 shows how the mental health domain of the QOF has changed from 2004 to 2006. There is greater specificity in who should be included and who should not, a reduction in the emphasis on lithium, and new indicators that encourage the application of a care plan, and the planned follow-up of people who might otherwise have defaulted from care.
The Mental health domain of the QOF

Indicator MH8: As the guidance from the NHS Employers makes clear, the changes to this indicator specify which diagnoses are to be included in the register. The intention is that people with schizophrenia and bipolar affective disorder are to be included as well as the much smaller number with an as yet unspecified form of psychosis. People with chronic depression, personality disorder and other conditions are excluded, as are children (unless they have one of the above conditions) and older people with dementia (for whom there is a separate domain).
The Read codes to use for the register are either 9H8 or 9H6. 9H7 is the code to designate that the individual has been excluded from the register. These codes are unchanged from the 2004 QOF.
Indicator MH9: It is appropriate to review the physical health annually of people on the mental health register. The type of review that needs to be undertaken is dependent on the personal circumstances of the individual, but consideration should be given to the following interventions for the co-morbidities described earlier.
All the interventions that have been undertaken should be recorded in the patient's electronic record, using the standard code for these interventions. The interventions can often be undertaken by a practice nurse or other suitably qualified professional.
The date of the annual review should be recorded, even though this is done automatically by the practice software. The Read codes to be used for the annual review are 6A6… and 8BM0.
Indicators MH4 and MH5: There are no major changes to the rationale or recording related to these indicators. Relatively few patients are taking lithium, but for those who are, it is important that there is clarity as to
Who is prescribing the medication Who is responsible for monitoring the medication and How frequently the patient is required to have appropriate blood tests that
monitor renal and thyroid function
Indicator MH6: About 25% of patients with a severe mental illness, including those on the Mental Health register (MH8) are managed entirely in primary care. People with schizophrenia and bipolar disorders have complex disorders that affect not only their mental health, but their physical health and their social functioning including employment and accommodation opportunities. A care plan provides the opportunity to review the needs of the patient and identify those individuals best able to provide the care required to meet those needs. The GP in this case acts not as the person who is going to provide all the interventions, but as the person who will co-ordinate care. The Care Programme Approach (CPA) for those people who are in contact with specialist mental health services sets out the same principles and can be used by the practice as evidence of a comprehensive care plan.
For those people who are not in contact with specialist mental health services, there are two alternatives. Either, with the agreement of the patient, refer to specialist mental health services, where a CPA will be generated. Alternatively, develop a practice-based ‘Patient-Centred Audit’ (PCA) which addresses the needs of the individual and who will deliver those needs. The principles of either CPA or PCA are exactly the same: an assessment of need, an agreement as to who can fulfil that need and a review date (to complete the audit cycle). CPA or PCA documents need the agreement of the patient (and/or their carer when appropriate) and should cover the areas described in Box 3.
Items to include in the care plan
Physical health needs Social care needs, including accommodation and employment Psychological needs, including talking therapies and medication and
compliance with medication Identifying relapse, including any ‘early warning signs’ and recording the
patient's wishes in case of relapse—similar to an advanced directive
CPA documentation always includes the name and contact details of the key worker — who is the first point of contact for patients who are in the care of specialist mental health teams. For individuals who elect to remain under the care of their GP and with whom a PCA plan is agreed, the equivalence of the key worker is the GP. It should be made clear that this does not mean that the GP is the key worker, has the training to become a key worker or is taking on the responsibility of a key worker. It means that the GP and the practice is the first point of contact for that patient as and when it is necessary. Care plans need to be reviewed at least annually, when both the physical health needs and broader psychological and social needs can be assessed. The Read codes that describe the presence of a care plan (CPA or PCA) are 8CR7 and 8CM2.
Indicator MH7: The practice will need to develop a system to
identify people on the mental health register — MH8 Invite them for at least an annual review — MH9 Record the date of that appointment Record that the patient did not attend Record that the patient was followed up in some way
The code to use for non-attendance for the annual review is 9N4t. Follow-up can be undertaken by any member of the practice team; follow-up can be either a telephone call or a visit, depending on circumstances.
The number of non-attendances is in itself not a ‘QOF scoring’ indicator; the points are earned by the follow-up within 14 days of the non-attendance. Experience in other clinical areas is that non-attendance rates are significantly reduced if patients are sent reminders before the appointment that they need to attend. Some practices have become very experienced and innovative in this, for example, using text messages sent to mobile phones to remind people to attend their appointments. Such a system may be very effective for people in this target group.
Key points
For patients with acute psychosis, early identification and early referral
to a specialist team will deliver benefits for the patient, in both the
short and long term Patients with chronic psychosis have increased morbidity and mortality
associated with physical health problems — the GP is best placed to provide
care for these physical health problems Changes to the Mental Health Act 2007 include the introduction of a new
Community Treatment Order. It is unclear what impact this will have on
primary care and the role of the GP The Mental Health QOF translates evidence of effective interactions into
specific quality interventions with the aim of enhancing both the physical
and mental health of patients with psychosis