
Abstract
Obsessive—compulsive disorder is a common psychiatric disorder characterized by intrusive thoughts or ‘obsessions’, which predispose to repetitive acts or rituals, known as ‘compulsions’. These compulsions are necessary to relieve the anxiety caused by the obsession. Patients have insight into the unnecessary nature of the symptoms but can find them hard to suppress. Inability to carry out everyday activities can lead to significant functional impairment. Many feel embarrassed and go to great lengths to conceal the disorder from others which can lead to a delay in diagnosis and management.
The GP curriculum and obsessive-compulsive disorder
GP Curriculum Statement 13 (Care of people with mental health problems) requires GPs in training to be able to
Manage people experiencing mental health problems in primary care, bearing in mind that several interventions may be effective for each mental health condition, including different forms of talking therapy, medication and self-help Describe specific interventions and guidelines for individual conditions such as obsessive-compulsive disorder (OCD), using best practice as described in National Institute for Health and Clinical Excellence (NICE) guidelines Demonstrate how to screen and diagnose people experiencing mental health problems, using effective and reliable instruments where they are available Describe how to access health and social care organizations, both voluntary and statutory, that are an essential component of managing people with mental health problems Describe when it is appropriate to refer to and collaborate with the specialist mental health services GP Curriculum Statement 8 (Care of children and young people) lists mental health problems in childhood in its knowledge base. It requires GPs in training to adopt a family-centred approach in dealing with patients, their families and their problems GP Curriculum Statement 3.5 (Evidence-based practice) requires GPs in training to demonstrate that they base their treatment and referral decisions on best available evidence.
This article describes the key features of obsessive—compulsive disorder (OCD) to help general practitioners (GPs) recognize patients with the disorder and provide a management strategy that can be used in the primary care setting to support them. As a GP, the ability to screen at-risk patients, diagnose those with symptoms, assess the severity of OCD, provide education and self-help strategies and referral appropriately to specialist mental health services is important. Although the course of OCD tends to be relapsing and remitting, effective control of symptoms can help to allow patients to live a normal life.
Prevalence of OCD
Estimates of the prevalence of OCD vary but it may affect up to 2—3% of the world population. There is a bimodal distribution with a peak of patients presenting in early adolescence and another in their mid-twenties to mid-thirties. Males and females are equally affected; however, males tend to present earlier than females. Only 15% of patients present after the age of 35.
Causes and pathophysiology of OCD
The precise causes of OCD are unknown. However, there are several recognized risk factors for development of OCD. A family history of OCD or other anxiety disorders makes the diagnosis of OCD more likely. Concordance for OCD is approximately 80% between monozygotic twins and 50% between dizygotic twins, so both genetic and environmental factors are likely to be important. Autoimmune mechanisms may also be involved. In children, an association has been noted between streptococcal infection and development of OCD.
The pathophysiology of OCD is also incompletely understood. Neuroanatomical variations such as increased amounts of grey matter have been noted in patients with OCD on imaging. Increased activity in the orbito-frontal cortex has been observed particularly when the patient is experiencing anxiety-provoking obsessions. Finally, abnormalities in serotonin levels are likely to be part of the pathological mechanism, as treatment with selective serotonin reuptake inhibitors (SSRIs) improves symptoms.
Symptoms and diagnosis
OCD is a clinical diagnosis based on the presence of
recurrent and persistent thoughts, impulses or images (obsessions) and repetitive acts or rituals (compulsions) which are carried out in order to reduce the anxiety provoked by the obsession
Obsessional thoughts are recognized as their own by patients and are often seen as ridiculous. However, they are often difficult to dispel and can be very distressing. The themes of these thoughts include fear of causing serious harm to themselves or others or thoughts around contamination. Some obsessions may be of a sexual or religious nature.
The action of carrying out a compulsion is not enjoyable but may temporarily relieve anxiety caused by the obsession. Compulsive acts are varied. Common rituals include excessive hand washing and cleaning and repeated checking. Patients may also feel compelled to ensure order and arrange items in a certain way or hoard unimportant objects. Compulsions are not necessarily actions and can be mental acts such as repeated counting or saying the same word silently over and over.
A vicious cycle of obsession and compulsion develops. For each obsession, anxiety gradually increases until a compulsion is carried out. The compulsion temporarily relieves anxiety but in the long term causes reinforcement of these thoughts and behaviours.
Screening
Patients with OCD usually have insight into their condition. They are often embarrassed by their symptoms and go to great lengths to hide the disorder from colleagues, family and friends. They are frequently reluctant to tell health care professionals about their symptoms for fear of being labelled as ‘mad’. As a result, patients with OCD may present in varied ways to general practice and often not directly with symptoms of OCD. This may lead to inappropriate referrals to other specialist or community services before a diagnosis of OCD is made. For example, a patient may present to general practice with stubborn hand dermatitis and be referred to dermatology, when in fact the dermatitis is caused by excessive hand washing performed as a compulsion to counter obsessional thoughts of contamination.
A simple screening tool has been developed which can help to identify those who may have OCD (Box 1). Use of this screening tool is recommended by the NICE to improve recognition of OCD by health care professionals.
Diagnosis
For those suspected to have OCD on screening questions, formal diagnosis with further questioning is needed. Box 2 summarizes the ICD-10 diagnostic criteria for OCD.
Screening questions for OCD
Do you wash or clean a lot? Do you check things a lot? Is there any thought that keeps bothering you that you would like to get rid of but cannot? Do your daily activities take a long time to finish? Are you concerned about orderliness or symmetry? Do these problems trouble you?
Severity
The severity of OCD depends on the amount obsessions and compulsions interfere with normal life and the amount of distress that they cause. The Yale-Brown Obsessive Compulsive Scale (Y-BOCS) (Box 3) is a reliable and consistent scoring system that can be used to categorize OCD as mild, moderate, severe or extreme. A score is assigned for each question from 0 to 4 (0 = none, 1 = mild, 2=moderate, 3=severe, 4=extreme). A score of 0–7 indicates subclinical OCD, 8–15 mild symptoms, 16–23 moderate symptoms, 24–31 severe symptoms and 32–40 extreme symptoms. There are several freely available online scoring systems (e.g. that found at website: www.brainphysics.com/ybocs.php) that can be used in the surgery with the patient to calculate this score.
Definitions and diagnostic criteria for OCD
Definitions
Obsessional thinking—recurrent persistent thoughts (Have I turned the gas off?), impulses (e.g. to shout obscenities) and images (often of an obscene/violent nature) causing anxiety or distress.
Compulsive behaviour—repetitive behaviours, rituals (e.g. hand washing, checking doors are locked) or mental acts done to prevent or reduce anxiety.
For a diagnosis of OCD to be made:
Obsessive thoughts/compulsive actions must be present on most days for at least 2 weeks The patient must recognize that the thoughts come from within him/herself (i.e. there are no passivity symptoms) Obsessive thoughts and compulsive rituals must have been unsuccessfully resisted in the past Thoughts and actions are unpleasant—if only due to repetition—and a source of distress or interference with activities
The Yale-Brown Obsessive Compulsive Scale
Time spent on obsessions Interference from obsessions Distress of obsessions Resistance to compulsions Control over obsessions Time spent on compulsions Interference from compulsions Distress from compulsions Resistance to compulsions Control over compulsions
Differential diagnosis
An important differential diagnosis of OCD is psychotic illness. In OCD, patients recognize that obsessive thoughts are their own. This differentiates patients with OCD from those with psychotic disorders such as schizophrenia which are characterized by thought disorders and particularly disorders of thought possession, where the patient feels that a thought has been planted in his head by someone else.
Obsessive—compulsive personality disorder is a separate diagnosis from OCD and another important differential diagnosis. Patients with obsessive—compulsive personality disorder have a need for rules, control and order. Changes to routine may cause significant distress or withdrawal. People with this disorder are often perfectionists and high achievers but find it difficult to delegate tasks or trust others.
Body dysmorphic disorder (BDD) requires similar intervention to OCD and is included in the NICE guideline for OCD management. Patients with BDD are concerned by perceived defects in their appearance and may spend disproportionate amounts of time looking in the mirror or trying to hide the abnormality.
Co-morbidities
Other psychiatric conditions commonly coexist with OCD and it is important to look for these when assessing patients for a possible diagnosis of OCD. Patients with co-morbidities may respond less well to treatment and may require more complex intervention:
Up to 50% of patients with OCD also have depression Phobias including social phobia and eating disorders can occur in up to 20% of patients with OCD Alcohol dependence and panic disorder are more common in patients with OCD
Management of OCD
OCD can be a very frightening and lonely condition and patients may be reluctant to discuss their symptoms with others. As a result, you as a GP may be the first person that patients with OCD have ever discussed their symptoms with. Being empathic and addressing concerns is therapeutic in itself.
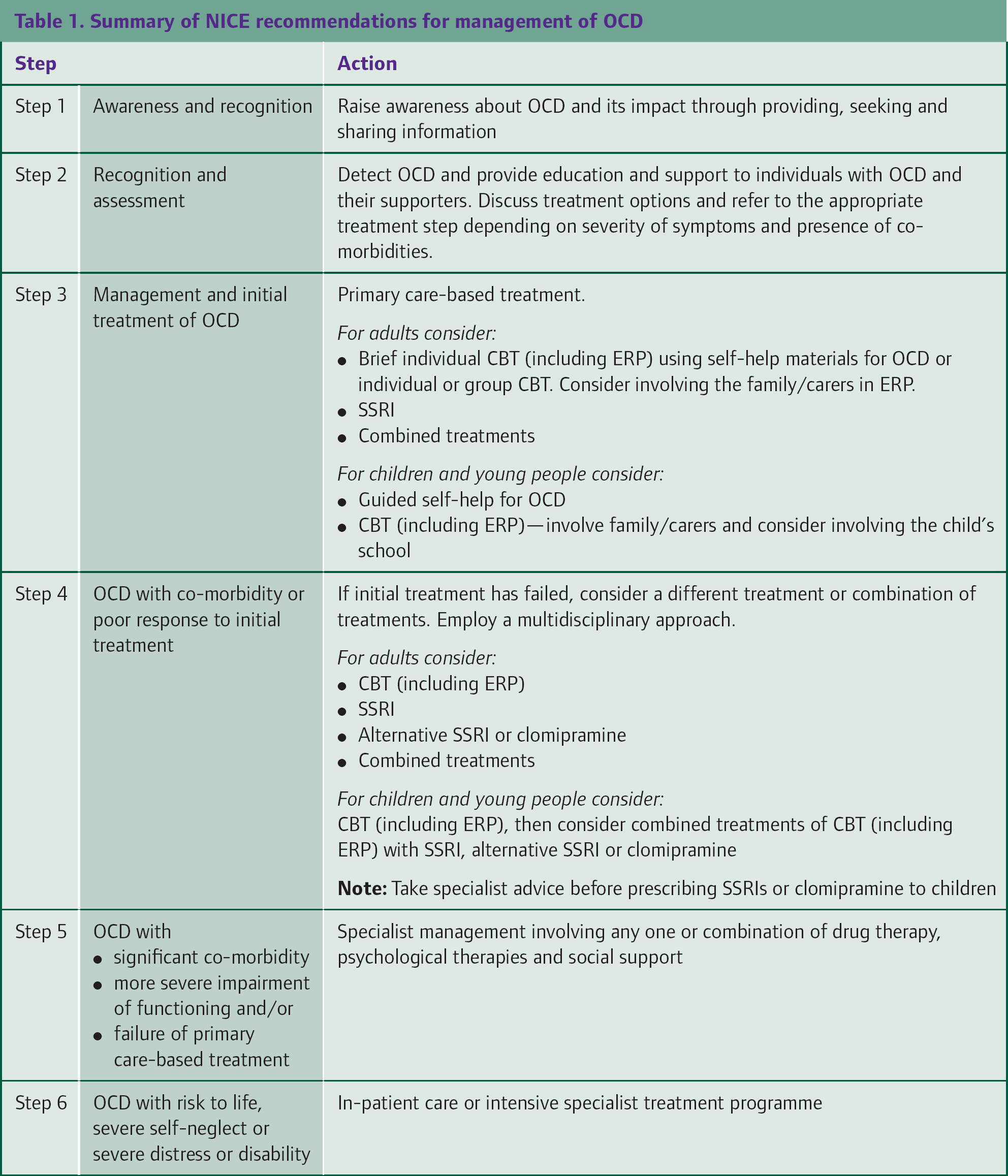
Once the diagnosis of OCD has been made, there are a variety of management options available. Choice of treatment depends on the severity and functional impairment of the patient and any associated co-morbidities. The NICE guideline for OCD advocates a stepped care model as shown in Fig. 1. Table 1 describes the suggested treatment options at each step.
Summary of NICE recommendations for management of OCD
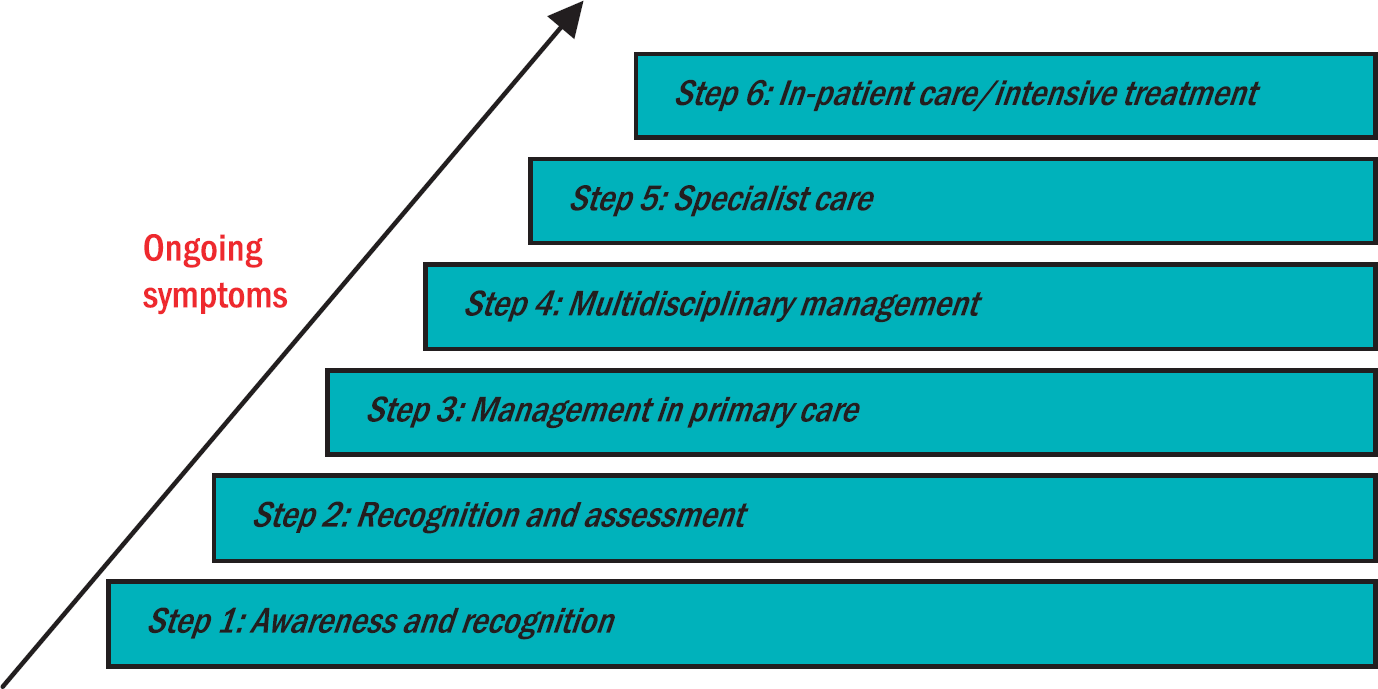
Stepwise approach to care of patients with OCD.
Education
Patients are likely to be less anxious about their symptoms of OCD if a clear explanation of their symptoms is provided. A discussion of the process of reinforcement caused by compulsions carried out in response to obsessions to alleviate anxiety may be helpful to allow understanding of the underlying mechanisms of the disease and enable the patient to engage effectively in self-help strategies. Reinforce verbal information with written information. Good leaflets about OCD are available from the Royal College of Psychiatrists (www.rcpsych.ac.uk), Clinical knowledge summaries (www.cks.nhs.uk/obsessive_compulsive_disorder#-361030), patient.co.uk (www.patient.co.uk/showdoc/23069002/) and patient self-help groups (Box 4).
Self-help
Guided self-help is an appropriate starting point for managing those with mild OCD. Discussions around the disorder and strategies to deal with symptoms (Box 5) as well as written materials, for example self-help books, or computer-based cognitive behavioural therapy (CBT) (such as OC.Fighter available from website: www.ccbt.co.uk/ocfighter.html) can be helpful. In the case of children or young people, it is important that the family is involved in this process both to understand and support the patient and also to prevent reinforcing the condition by being complicit in some compulsion behaviours.
OCD self-help organizations and books
Obsessional Thoughts and Behaviour: Help for Obsessive-compulsive Disorder by Frederick Toates, HarperCollins.
Understanding Obsessions and Compulsions: A Self-help Manual by Frank Talis, Sheldon Press.
Overcoming Obsessive-Compulsive Disorder: a Self-help Book using Cognitive-behavioural Techniques by David Veale and Robert Willson, Constable and Robinson.
A simple self-help strategy for patients with mild OCD
Carefully recognize your unwanted thoughts-obsessions—and the actions that you take to put them right—compulsions Gradually face some of the things that you fear. Work out an anxiety ladder to help you to do this (i.e. grade a list of unpleasant situations in terms of unpleasantness for you). Begin with the easiest step. Do not carry out any compulsions to reduce or neutralize your anxiety when you are facing the feared situation Break the obsession compulsion cycle Challenge gloomy or critical thoughts that you may have about yourself
Cognitive behavioural therapy
CBT consists of a combination of
Behavioural therapy that aims to change behaviour. Usually the therapist uses a system of graded exposure combined with teaching a method of anxiety reduction and response prevention [known as exposure and response prevention (ERP)]. The patient is encouraged to experience feared thoughts or situations and then resist any attempt to carry out a compulsion to release anxiety. This helps to break the cycle of reinforcement which is set up by reacting to obsessions with compulsions to temporarily relieve anxiety—a process called habituation. Cognitive therapy that focuses on peoples' thoughts and the reasoning behind their assumptions on the basis that incorrect assumptions lead to abnormal reactions which then reinforce these assumptions further (a vicious cycle).
There is evidence to show CBT is an effective treatment for OCD. For patients with mild functional impairment due to OCD, NICE recommends brief intervention (usually less than 10 hours) with CBT including ERP and guided self-help. If this is inadequate or the patient has moderate impairment, more intensive CBT may be offered.
Medications
The pathogenesis of OCD has been linked to abnormal serotonin levels. Drugs which increase levels of serotonin in the brain have been shown to improve symptoms of OCD in randomized controlled trials (RCTs). A recent Cochrane review (Soomro et al., 2008) of 17 RCTs comparing SSRIs with placebo showed that symptom severity, measured using Y-BOCS, was significantly reduced in patients taking an SSRI compared with placebo. SSRIs included citalopram, fluoxetine, fluvoxamine, paroxetine and sertraline. There was no significant difference in effectiveness between these drugs. Side effects included nausea, headaches and insomnia.
The tricyclic antidepressant clomipramine, which also increases serotonin levels, is effective too. However, it is more toxic in overdose than the SSRIs and can cause cardiac toxicity in children, so is reserved for use as a second line drug if SSRIs are ineffective.
The NICE guidelines recommend an SSRI for patients with moderate OCD or for those with mild impairment where a brief CBT intervention has been ineffective. A combination of CBT and SSRI can be offered for patients with inadequate response to treatment at 12 weeks after multidisciplinary review or for patients with severe functional impairment. If patients do not respond, a different SSRI or clomipramine should be tried.
Surgery
Some neurosurgical techniques have been tried in patients with refractory OCD. The principal of surgery is to disconnect neuroanatomical pathways thought to be involved with the pathogenesis of OCD. There is some evidence of reduction in severity of symptoms; however, as with any surgical procedure, there are perioperative risks and also postoperative side effects which include seizures and headache. This approach is reserved only for the most resistant cases and is unusual in the UK.
Long-term outcomes
Relapse and remission is common in OCD and many patients will never be free of the disease. Strategies to cope with symptoms and limit functional impairment are key to allow patients to work, socialize and coexist with other family members. Negative emotions expressed by family members towards patients are associated with worse outcomes following treatment.
Key points
OCD is a common psychiatric disorder which can lead to significant functional impairment Screening is important to identify patients who may not be forthcoming about OCD symptoms to health care professionals During diagnosis, it is important to assess severity and identify any coexisting psychiatric disorders Treatment depends on the degree of functional impairment and includes education, patient self-help, CBT and medication Symptoms are likely to relapse and remit, so treatment should be aimed at maintaining maximal function to allow patients to continue daily activities