
Abstract
This competency is about aspects of care beyond managing straightforward problems, including the management of co-morbidity, uncertainty and risk, and the approach to health rather than just illness.
In this article, we look at the second part of the performance area described above and will consider uncertainty and risk separately although in real life, they overlap.
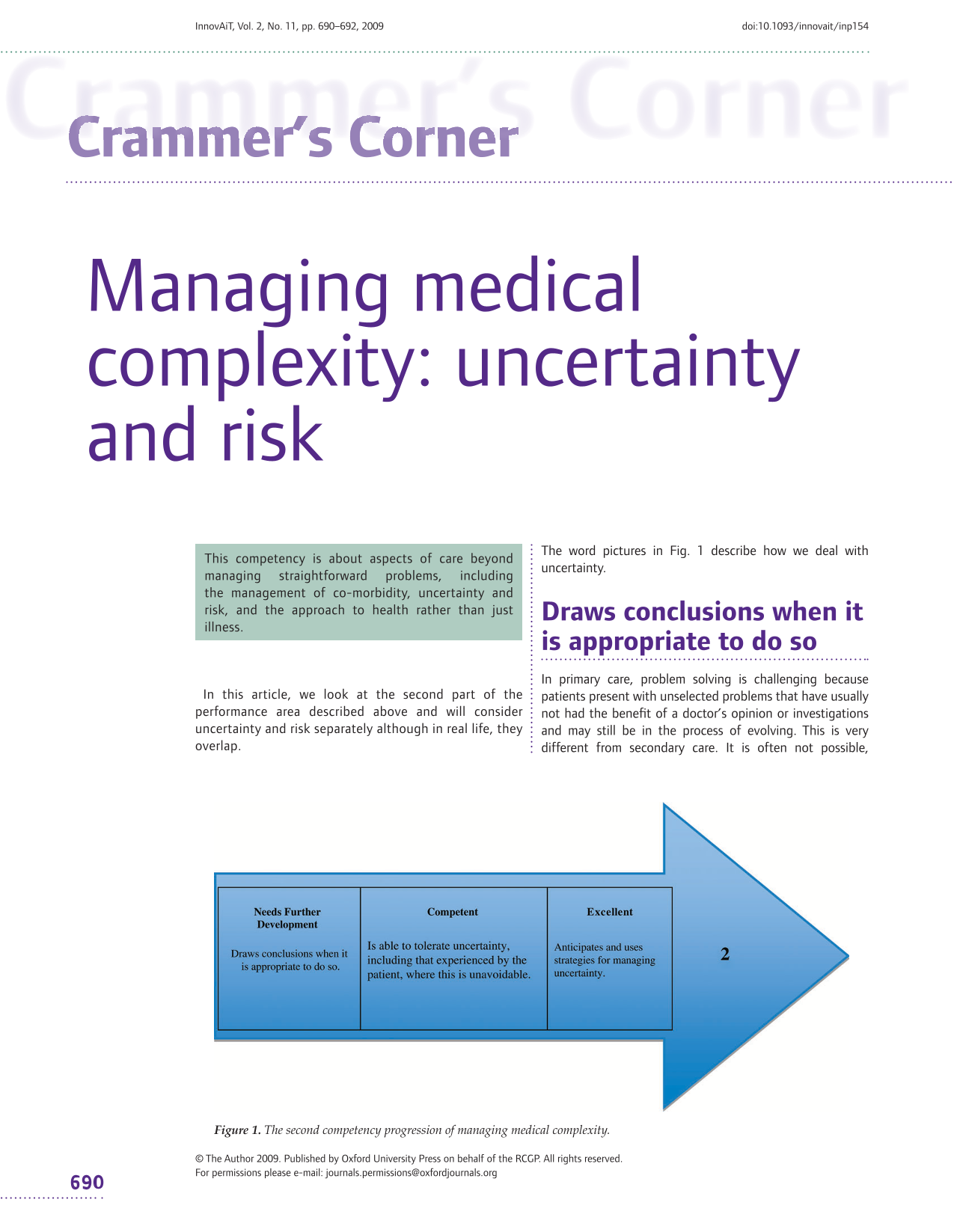
The word pictures in Fig. 1 describe how we deal with uncertainty.

The second competency progression of managing medical complexity.
Draws conclusions when it is appropriate to do so
In primary care, problem solving is challenging because patients present with unselected problems that have usually not had the benefit of a doctor's opinion or investigations and may still be in the process of evolving. This is very different from secondary care. It is often not possible, therefore, to exclude a serious condition at the initial consultation and this creates anxiety for both patient and doctor.
To identify a problem, we need to allow time for a recognizable pattern to emerge. How long this takes depends upon our
skill in collecting information from history taking, examination and investigation and mental library of patterns against which the emerging information can be mapped
There are obvious dangers with jumping to conclusions, e.g. a premature diagnosis of hypertension leading to the adverse consequences of labelling, treatment and surveillance. However, it may be risky to wait before taking action even though the information available is scanty. An example of this is when we act on the basis of red flag symptoms or signs, whereby a single symptom such as an isolated postmenopausal vaginal bleed may be enough to trigger referral.
Is able to tolerate uncertainty, including that experienced by the patient, where this is unavoidable
This competency is thought by educators to be particularly significant in this performance area.
The ‘threshold’ for making a diagnosis is often not clear-cut. For example, when does a painful toe with a normal serum uric acid become probable gout?
The ‘patients’ used in research are often not representative of patients in the community. For example, many studies on depression excluded patients who were taking other drugs, had other chronic health problems or drank alcohol. How many depressives do you deal with who fall into this category?
The ‘treatments’ used in research are often binary because this suits trial designs like randomized control trials, whereas treatment strategies in primary care are usually multifactorial. For example, children treated for otitis media may have a combination of parental advice, antipyretic and antibiotic but much of the research only considers the antibiotic element.
Building from the previous competency, in which we demonstrated our ability to judge when to wait and when to act, this competency looks at our ability to cope with the pressure that uncertainty puts upon us.
Uncertainties should be tolerated in proportion to the evaluation of risk. The judgment may not be appropriate if we are overconfident. Keep a check whether you are overconfident through feedback from colleagues and through your portfolio of assessments.
Assessing risk means knowing the red flags (specific symptoms and signs that indicate further action is required), for example in back pain, dyspepsia and headache.
A reflective diary recording consultations where you feel a high degree of uncertainty will help you see where your DENs (doctor's educational needs) lie.
We also have to live with the patient's uncertainty. For example, the patient may want an X-ray for reassurance, but if it is not clinically indicated we have to resist the temptation to reduce our anxiety by investigating more than the situation warrants. Clearly, communication skills are vital if the patient is also to be helped to live with the uncertainty caused by not having (unnecessary) tests.
Anticipates and uses strategies for managing uncertainty
We are in a good position to influence patient expectation because of our knowledge of probabilities. Therefore, we might anticipate and prevent problems by talking through the natural history of the condition or the way in which it might evolve. This also educates patients about ‘deviations’ from the expected path that should be brought to our attention. An early discussion about upon the diagnostic ability of the tests will also help to prevent expectations becoming inappropriate.
Reducing uncertainty is not done at a single point in time, but is a continuous process.
In the longer term, uncertainty diminishes through experience as we internalize more scripts of how problems evolve and how the significant deviations from what appears ‘benign’ come to light (e.g. how does dizziness start to look like an acoustic neuroma? and how does anxiety start to look like obsessive—compulsive disorder?)
One of the ways of dealing with uncertainty is to learn to manage risk. This is described in Fig. 2.

The third competency progression of managing medical complexity.
Appropriately prioritizes management approaches, based on an assessment of patient risk
The management approaches that are discussed with the patient should, first and foremost, be the safest available given the known facts.
Assessing patient risk is not simply a matter of establishing the medical diagnosis. Patients may also be at risk for social reasons, for example if they are depressed and cannot self-manage or if they cannot be adequately supervised.
Risk assessment also comes into play when deciding on the pros and cons of treatment. For instance, a decision on the drug management of depression might be influenced by an objective depression score. Formal risk assessment is becoming a more prominent feature of chronic disease management as a method of gauging the overall impact of many factors on disease progression.
Communicates risk effectively to patients and involves them in its management to the appropriate degree
As we progress, the challenge is to explain the risk factors, put them in proportion with each other and, importantly, prevent misunderstanding. For example we may need to explain to patients with chronic kidney disease category 3 that they are not suffering from kidney failure and in need of dialysis or a renal transplant!
Often, the explanation of risk will cover what might happen (particularly, what might go wrong) in different situations including what might happen if ‘nothing’ was done. We might also discuss the possible timescale. Sometimes, the explanation may require a diagram or picture and occasionally the use of numbers and percentages. If we remember to ask, patients can usually guide us about which approach they prefer.
Uses strategies such as monitoring, outcomes assessment and feedback to minimize the adverse effects of risk
In practice, much of risk reduction depends upon the quality of our follow-up arrangements and safety netting. Record keeping is vital so that both patient and clinicians are aware of the degree of risk, the timescale for improvement and the circumstances under which the patient should be reviewed.
When the risk is more complicated or potentially more serious, the management approach may need to be explained to the patient more detail, with supporting information and possibly with another family member or carer sitting in the consultation. For example, think about an asthmatic with cardiac failure who is being initiated on a beta-blocker.