
Abstract
Learning disability is commonly encountered in General Practice affecting between 1 and 2% of the Western world. Patients with learning disabilities have two and a half times as many associated medical problems. It often leads to functional impairment and increased need for lifelong support involving medical services. The care of patients with learning disabilities requires a holistic approach with awareness of the services available and knowledge of the barriers to health care faced by this patient group. This article aims to outline the definitions of learning disabilities and screening and diagnosis of these conditions in primary care, causes, principles of management and the difficulties and barriers in care delivery for these patients.
The GP curriculum and childhood learning disabilities
The GP curriculum statement 14 refers to the care of people with learning disabilities. It highlights that primary care is the main service provider for this group of patients with support from specialist community teams. This section emphasizes the knowledge, skills, attitudes and person-centred approach needed for a GP to manage people with learning difficulties.
In particular, GPs should
Be aware of likely associated conditions and know where to obtain specialist help and advice Understand how psychiatric and physical illness may present atypically in patients with learning disabilities who have sensory, communication and cognitive difficulties Use additional skills of diagnosis and examination in patients unable to describe or verbalize symptoms
GP curriculum statement 8 refers specifically to the care of children and young people. With particular relevance to children with learning disabilities, it stresses that GPs should:
Have an important role in child health screening and surveillance to target a programme of early support Be able to help children, young people and their parents cope with chronic illness and disability Demonstrate an understanding of multi-agency working Coordinate care with other professionals Take an advocacy position for the patient or family when needed Take a role in safeguarding children and young people
Definitions
The World Health Organization definition of mental retardation or learning disability, as it is now more frequently known, is a condition of arrested or incomplete development of the mind, which is especially characterized by impairment of skills manifested during the developmental period. This contributes to the overall level of intelligence, i.e. cognitive, language, motor and social abilities. The diagnostic and statistical manual of mental disorders IV (DSM-IV) includes three components: cognitive delay (as measured by IQ) impaired adaptive behaviour and onset before aged 18 years (see Fig. 1). Both of these definitions further classify learning disability as mild, moderate, severe and profound (see Table 1).
The classification of learning disability


DSM-IV definition of learning disability.
In addition to the above definitions of learning disability, there are specific learning disorders. There is considerable overlap between the specific learning disorders. IQ is often normal and there may be a family history. With all these disorders, assessment may incorporate hearing and vision and include input from educational psychologists, physiotherapists and occupational therapists. Treatment is directed towards improving skill acquisition with educational and information technology support. Box 1 contains further information about these disorders.
Types of learning disorder
Disorder of motor planning and execution with no neurological findings on examination. Affects 2% of the population. Common features include clumsiness, awkward gait, poor body awareness, difficulty dressing and eating, poor sense of direction and difficulty copying. The difficulties may affect self-esteem and educational progress suggesting that a child has greater academic difficulties than is the case.
This is a disorder of reading skills out of proportion with the child's IQ. It is often used if the child's reading age is more than 2 years behind their chronological age. It affects 3–5% of the population and is more common in males.
Rarer than dyslexia. A disorder affecting the handling of numbers and mathematical concepts.
Screening and diagnosis in primary care
Early diagnosis of learning disability ensures appropriate treatment, intervention and allows resources to be tailored to a child to aid their development and maximize their potential. There are many ways in which childhood learning disability can present to a GP. Parental concern is frequently one of these and this should not be belittled. Box 2 lists some of these. One of the first steps for a GP can be to consider at-risk individuals and to opportunistically screen for learning disability in this population. These risks include genetic, familial, prenatal, perinatal and post-natal factors. Severe or profound learning disability is usually apparent from infancy as global developmental delay. Moderate learning disability emerges when there is a delay in speech and language as motor milestones may be normal. Mild learning disability may not be apparent until school age.
In order to screen for developmental delay as a way of detecting learning disability in children, it is important for all doctors in primary care to have a good working diagnosis of normal developmental milestones (Fig. 2). The most sensitive marker for learning disability is language development. Box 3 includes the developmental milestones for speech and language development.
Developmental milestones for hearing, speech and language. Illustrations by Scott Jarvie.
Ways in which learning disability may present
Parental concern Antenatal screening Newborn hearing test Neonatal check (in hospital or primary care) — dysmorphic features and abnormal tone 6 week check — smile, vision, dysmorphic features and tone Developmental screening according to the child health promotion programme (8 and 18 months and 3 and 4 years) — developmental delay Concerns from the health visitor Concerns from nursery/preschool Opportunistic screening when the child/family presents to the GP for other reasons, e.g. illness and vaccinations Concerns raised by teaching staff Presentation with conditions associated with learning disability, e.g. epilepsy Follow up of ‘at-risk’ individuals, e.g. preterm infants
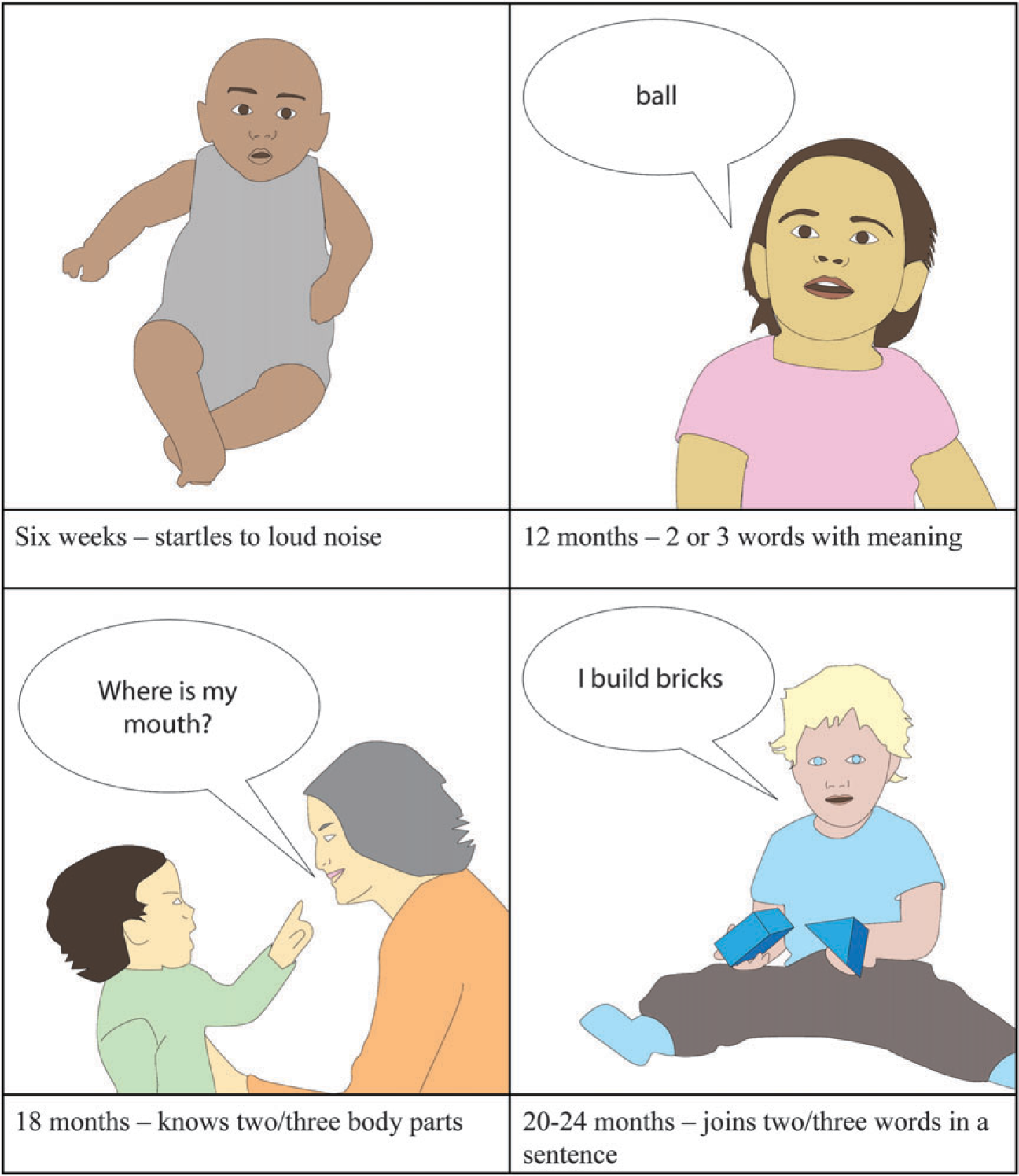
Developmental milestones for speech and language
6 weeks — startles to loud noise 3 months — localizes to sound 7 months — babbling in syllables 11 months — one word with meaning 1 year — understands phrases. Two/three words with meaning 15 months — points to objects he/she wants 18 months — knows two/three body parts 2 years — joins two/three words in a sentence 2.5 years — knows full name and sex 3 years — count to 10. Names three colours. Understands ‘on’, ‘in’ and ‘under’ 4 years — fluent conversation. Understands ‘in front of’ and ‘behind’ 5 years — knows age. Can tell time
Causes
Both genetic and environmental factors contribute. As mentioned previously, most children with moderate to severe learning disability will have an identifiable cause. This is in contrast to children with mild learning disability in which children from lower socio-economic classes are over-represented. Population studies have shown a male preponderance, which is felt to be attributable to X-linked genetic mechanisms.
Genetics
The genetics of learning disability are becoming better understood. They include mutations in X-linked genes, imprinting as is seen in Prader—Willi and Angelman's syndromes, trinucleotide repeat expansion as seen in Fragile X, rearrangements involving subtelomeric regions and trisomy, such as that seen with Down's syndrome. Box 4 lists some of the commoner well-known genetic causes of learning disability.
Genetic causes of learning disability
Affects one in 600. Accounts for one-third of cases of severe learning disability.
Affects one in 3000. Severe/profound learning disability is uncommon. Autistic features and attention deficits are common.
Affects one in 3000. Physical and behavioural characteristics alert the clinician to the need for genetic testing. Deficits in motor skills and inhibitory control are common as are autistic features and attention deficits. Girls have a lower rate of problems.
Loss of paternal contribution of chromosome 15. Distinct physical and behavioural characteristics.
Loss of maternal chromosome 15.
XXY. Often gives rise to mild learning disability.
Environmental factors
Environmental factors are also associated with learning disabilities. Lead and mercury poisoning can give rise to learning disability even at a low dose. Other neurotoxins to the developing brain include alcohol and sodium valproate.
Prematurity
Prematurity is a well-established risk factor for learning disability particularly a birth weight of less than 1000 g. Even birth weights of less than 3000 g raise the likelihood of school-identified learning disability. Each week of gestational age before delivery significantly reduces the chance of learning disability.
Other causes of learning disability occurring in the neonatal, infancy or early childhood period include congenital hydrocephalus, meningitis, encephalitis, traumatic brain injury, radiation and chemotherapy. Despite the implication of chemotherapy as a cause for learning disability, most children surviving treatment for acute lymphoblastic leukaemia have very few signs of cognitive impairment.
A Child with Down's syndrome

Metabolic causes
Various metabolic and inborn errors of metabolism can give rise to learning disability. One of the more common endocrine problems associated with learning disability is hypothyroidism. If this is recognized and treated early, then children may achieve their full potential or have only very mild delay in achievement areas. Other rarer causes include phenylketonuria, homocystinuria, galactosaemia and mucopolysaccharide disease.
Associations with other medical conditions
Important associations exist between learning disability and other medical conditions. These associations have important implications for health care professionals and services. Epilepsy is much more common among people with learning disability with rates of about 30% quoted. Prolonged seizures and status epilepticus are much more frequent than in the general population.
In 2001, the International Association of Scientific Study of Intellectual Disability published guidelines for the management of epilepsy in patients with learning disability. Epilepsy combined with learning disability is a strong indicator of psychiatric and behavioural problems.
Cerebral palsy is more common in patients with learning disability and about 60% of patients with cerebral palsy will have an associated learning disability.
Visual and hearing problems are common among the learning-disabled population with over 30% having visual problems and 30% having hearing problems. There is a high risk that these perceptual problems are overlooked especially in those with severe learning disability.
Hypothyroidism is common in people with Down's syndrome and should be screened for. If left untreated, it can lead to learning disability. Fortunately, our newborn screening programme tests for hypothyroidism and phenylketonuria, another preventable cause of learning disability.
Patients with learning disability have an increased incidence of psychiatric illness and behavioural problems. Psychotic conditions, attention deficit hyperactivity disorder (ADHD) and autistic behaviours, self-injurious behaviours, violent outbursts, eating disorders and pica are all much more common.
Autism can occur in all levels of intellectual functioning. Initially, it was felt that 75% of patients with autism had learning disability. This is probably an overestimate and 15% is a more reasonable figure. However, the converse is true; learning disability is strongly associated with autism. One in three of those with severe learning disability and one in 10 of those with mild learning disability meet the criteria for autism. It is usually detected from 2 to 4 years. It is a triad of impaired social interaction, speech/language disorder and restricted interests with ritualistic behaviour.
The role of the GP
In diagnosis
The initial role of a GP in management of children with learning disability can be to detect when a child's development is abnormal or delayed and refer to the child development team or service. This is why it is imperative for GPs to be able to perform a basic developmental assessment. The concept of limit ages can be useful as these signal the need for referral for a more detailed developmental assessment. Box 5 lists some of these. It is, however, important to remember that parental concern should be taken seriously and a one-off subjective assessment is not always completely reliable. Box 6 lists some other reasons for referral to the child development team.
Limit ages for development
4 months — no head control 9 months — unable to sit without support 13 months — unable to pull to stand 18 months — unable to independently walk
3 months — unable to fix and follow 6 months — unable to reach for objects 8 months — unable to transfer objects 12 months — no pincer grip
7 months — no polysyllabic babble 10 months — no consonant babble 18 months — unable to say six words with meaning 2 years — unable to join words 2.5 years — unable to make three-word sentence
8 weeks — no smile 2.5 years — no symbolic play 3.5 years — no interactive play
Reasons for referral to the child development team
Concerns about development in any of the four developmental spheres (including vision and hearing) Worries about autism or ADHD Children with long-term disability needing assessment or services Children with behavioural difficulties not responding to primary care support Children looked after by local authorities
The paediatrician will complete a detailed development assessment, using tools such as the Griffiths development scales and establish whether there is an underlying, and perhaps even treatable, diagnosis. They may, if deemed appropriate, use some of the investigations listed in Box 7.
Investigations to be considered for a learning-disabled child
Amino acid studies Metabolic screening Genetic studies—karyotype and fluorescence in situ hybridization Electroencephalogram Audiometry Magnetic resonance imaging of the head Thyroid function tests
Establishing a cause can be important for a number of reasons. Firstly, there may be treatment available for the underlying cause. Secondly, it allows parents to be informed about the likely level of disability and any expected co-morbidities. It can determine whether genetic counselling is necessary and may affect management in future pregnancies. If a child is diagnosed with a condition, it is useful to find out about this in order to optimize your care as the GP for this child.
The role of the GP at the time of diagnosis is to fully inform the family of the reasons for referral and explain the local system as well as which services are responsible for what. It can also be to direct the family to helpful reliable information and support groups. In addition to this, the carers need adequate information about benefits and allowances. Box 8 lists some reliable web-based sources of information.
Useful websites for further information
www.intellectualdisability.info (web-based learning resource about intellectual disability)
www.mencap.org.uk (mencapisthe UK's leading learning disability charity)
www.dsmig.org.uk (Down's syndrome Medical Interest Group)
www.fragilex.org.uk (Fragile X Society)
A Child with Angelman's syndrome Maria Platt-Evans/SPL

In established learning disability
The key to managing children with established learning disability is to use a multidisciplinary approach. Child development services often include a paediatrician, physiotherapist, occupational therapist, speech and language therapist, clinical psychologist, health visitor and social worker.
It is important as the GP to communicate with the members of the child development service. It is essential to ensure that these children have hearing and visual screening if there is any suggestion of any problems with sensory perception. Mental health promotion is paramount for both the child and the family. GPs should be alert to identifying and referring psychiatric disorders. Problem behaviours are common and initially GPs should aim to illicit exacerbating factors such as medications and concurrent illness but they may need specialist expertise.
One of the main roles of the GP is to manage medical problems not related to the disability such as sore throats and to ensure that health promotion such as vaccinations are carried out. It is important for primary care professionals to maintain an open mind and not allow frustration hinder medical care. Medical illness in a patient with learning difficulty may present with frustration or behaviour change and often it requires patience to reach a diagnosis. Carers can be very helpful in helping the child communicate. As the GP, it is also necessary to be alert to child protection issues that are more common in children with disabilities.
Another role for the GP is to promote compliance with medications and to regularly review patients' medications. For future pregnancies, if genetic causes are identified, GPs may be involved in referring for preconceptual counselling. Box 9 summarizes the main roles of the GP in caring for a child with learning disability
The role of the GP
Refer to community services Manage medical problems Communicate with patient and carer Health promotion including mental health in child and family Early detection of any associated conditions Preconceptual/antenatal counselling for the family in future pregnancies Ensuring carers receive information about benefits/allowances
Difficulties and barriers in care delivery
Several difficulties and barriers of care delivery have already been touched upon. Firstly, often the attitudes and values of health care professionals towards patients with learning disabilities can impact on care delivery. Frustration, lack of knowledge, confidence and training in dealing with patients with learning disability can impact negatively. In a study in 2004 relating to care provision for patients with intellectual disability, many GPs felt inadequately trained in behavioural and psychiatric conditions, human and sexuality issues, complex medical problems and preventative and primary health care.
Other barriers are explained by the concept of diagnostic overshadowing. This is when a patient's symptoms are attributed to their learning disability rather than seeking another potentially treatable cause such as physical problems (toothache), psychiatric causes (depression) or social causes (abuse).
In primary care, the health needs of a learning-disabled patient may not be met for several reasons. Firstly, patients are less likely to self-present even when they have a potentially treatable medical problem. Secondly, specific health needs associated with their learning disability may not be addressed, for example, screening for hearing problems in the severely learning disabled and thyroid screening in Down's syndrome. Thirdly, a lack of uptake of health promotion in this group of patients, for example, blood pressure monitoring and smear tests. Hopefully, however, after reading this article, you will feel more confident in managing patients with learning disability and will be more aware of the reasons for these barriers and steps you can take to minimize them.
Key points
The quality of care for people with learning disabilities is strongly affected by the attitudes and values of the professionals working with them Certain medical conditions occur with increased frequency in patients with learning disability and GPs should be aware of these There are many barriers to optimal care delivery for patients with learning disability and steps should be taken to minimize these Intervention and management are multidisciplinary, including education and social services