
Abstract
Revalidation for general practitioners is about to become a reality. It is envisaged that the process will be live within 18 months and that GPs should already be accumulating evidence for use in the process. For many GPs the purpose of, and the process for, revalidation is shrouded in mystery.
The GP curriculum and revalidation
Statement 3.1 of the GP Curriculum (Clinical governance) requires GPs to be able to describe the relationship between clinical governance, continuing professional development and appraisal and revalidation.
InnovAiT editor Dr Chantal Simon discusses the immediate future with Dr Chris Price. Dr Price is an Associate Dean in the Wales deanery with responsibility for continuing professional development (CPD) and appraisal. He was the Royal College of General Practitioners (RCGP) CPD fellow and has worked on the development of the credits system for revalidation.
Chris, what exactly is revalidation?
Revalidation is the process by which doctors will be given a positive affirmation of their right to practice. In the case of general practitioners, the RCGP have proposed standards and methods for the revalidation of individuals. These proposals will need to be ratified by the General Medical Council (GMC) and are described in the online RCGP guide to the revalidation of general practitioners. Revalidation is a continuous process but a decision on the revalidation of an individual will be made at least once every 5 years. In November 2009, doctors on the GMC medical register at that time were entitled to a license to practice. All GPs practising in the UK are also listed on the general practice register. In order to successfully complete the revalidation process, a GP will have to produce evidence of their fitness to relicense (medical register) and recertify (general practice register).
Isn't revalidation about catching underperforming doctors?
No I really don't think so, ‘Medical revalidation — principles and next steps’ (2008) contains the key principle:
revalidation in the United Kingdom should be seen primarily as supportive, focussed on raising standards, not a disciplinary mechanism to deal with the small proportion of doctors who may cause concern
Clinical governance systems in the primary care organizations will continue to operate; the GMC performance procedures will remain. Underperformance will remain a function of these systems and revalidation will simply affirm demonstrated standards.
How will I collect evidence for revalidation?
Every doctor in the UK will be required to amass a portfolio of evidence. General practitioners will be required to produce an evidence set as required by the RCGP. There may be additional pieces of evidence that the GMC will require for the relicensing aspect of revalidation. It is expected that this evidence will be stored in an electronic portfolio. Much if not all of the evidence collected for the purposes of revalidation will form the basis of the five appraisals doctors will need to undertake during a revalidation cycle. The GMC have produced a working framework for appraisal and assessment which relates Good Medical Practice to four domains (Box 1). Each of these domains has three attributes and it is likely that a doctor will be required to demonstrate evidence of fitness to practice against each of the 12 attributes.
What evidence will I need in this 5 year period?
The current proposals are detailed on the RCGP website in the guide to revalidation of GPs. This may be subject to modifications by the GMC, and there may also be additions to complete the requirements for the licensing aspect. The RCGP have proposed the 13 evidence areas listed in Box 2. On face value this may appear an onerous task. This is, however, the evidence set for a 5 year cycle. Breaking down each evidence area in more detail:
The four domains of good medical practice
Attributes
Maintain your professional performance Apply knowledge and experience to practice Keep clear accurate and legible records
Attributes
Put into effect systems to protect patients and improve care Respond to risks to safety Protect patients and colleagues from any risk posed by your health
Attributes
Communicate effectively Work constructively with colleagues and delegate effectively Establish and maintain partnerships with patients
Attributes
Show respect for patients Treat patients and colleagues fairly and without discrimination Act with honesty and integrity
The 13 proposed evidence areas proposed by the RCGP
Evidence area 1: Statement of professional roles and other basic details Evidence area 2: Statement of exceptional circumstances Evidence area 3: Evidence of active and effective participation in annual appraisals Evidence area 4: A PDP from each annual appraisal Evidence area 5: A review of the PDP from each annual appraisal Evidence area 6: Learning credits in each year of the revalidation period and in the revalidation period overall Evidence area 7: MSF from colleagues Evidence area 8: Feedback from patients Evidence area 9: Description of any cause for concern and/or formal complaint Evidence area 10: Significant event audits Evidence area 11: Clinical audits Evidence area 12: Statement on probity and health Evidence area 13: Additional evidence for areas of extended practice
Evidence area 1: statement of professional roles and other basic details — This area requires an individual to provide basic details such as name, address, GMC number, etc. Importantly in addition to this, all professional roles, whether paid or voluntary, must be listed. A GP operating as a locum for many different practices should keep a record of sessions worked. The guide to revalidation of GPs states that this must include: ‘all current posts and those within the revalidation period — date started, time commitment, employer (including address).’
Evidence area 2: statement of exceptional circumstances — This area allows a GP to declare unusual or difficult aspects of their working life during the 5 year cycle. Examples could include a sabbatical period, prolonged illness or a break-up/change of practice. Maternity leave would be covered under this evidence area.
Evidence area 3: evidence of active and effective participation in annual appraisals — The standard revalidation portfolio should include evidence of annual appraisal.
Evidence area 4: a personal development plan from each annual appraisal — A personal development plan (PDP) should be constructed and agreed at each annual appraisal. The revalidation guide does not give a minimum or maximum number of goals but describes:
‘A valid PDP must contain the following key elements for each goal:
a statement of the development need an explanation of how the development need will be addressed (the action to be taken and the resources required) the date by which the goal will be achieved and the intended outcome of the goal’.
Evidence area 5: a review of the PDP from each annual appraisal — Completion on PDP goals from the previous appraisal is required. The GP is required to reflect on the changes resulting from the achievement or the reason that the goal was not met.
Evidence area 6: learning credits in each year of the revalidation period and in the revalidation period overall — All medical Royal colleges will be utilizing learning credit systems. The requirements will be a minimum of 50 credits a year equating to 250 credits in the 5 year cycle. The RCGP is unique in proposing a system that is not wholly time-based but one that reflects the outcomes of learning (as discussed later).
Evidence area 7: multi-source feedback from colleagues — The RCGP has proposed two multi-source feedback (MSF) questionnaires from colleagues in the 5 year revalidation cycle. One within the first 2 years and one in the final 2 years. The MSF must use a validated tool, and currently only the GMC's MSF instrument reaches college requirements. Reflection on the outcome of these surveys is required and, if appropriate, an action plan must be formulated to address issues that arise from the feedback.
Evidence area 8: feedback from patients — The RCGP proposes either two patient surveys (must be from patients actually consulting the individual), or, if the first patient survey is satisfactory, a review of consulting skills may be substituted (e.g. a properly conducted analysis of videotaped consultation).
Reproduced with kind permission from Clarity Informatics.
Evidence area 9: description of any cause for concern and/or formal complaint — If, during the revalidation period, an individual has been identified as a cause for concern, a full description of the circumstances and the outcome must be included. All complaints that have activated (or indeed should have activated) a formal complaints procedure must also be fully described. The guide to the revalidation of general practitioners includes a chapter that sets out the processes for this.
Evidence area 10: significant event audits — The requirement in this area will be for five significant event audits in the 5 years. It is not expected that one will be produced each year; however, there should be a spread across the revalidation period. The revalidation guide describes a significant event audit as:
‘An account of a significant event audit should not allow patients to be identified and should comprise:
title of the event date of the event date the event was discussed and the roles of those present description of the event involving the GP what went well? what could have been done better? reflections on the event in terms of:
•knowledge, skills and performance safety and quality communication, partnership and teamwork and maintaining trust what changes have been agreed:
for me personally and for the team changes carried out and their effect’.
Evidence area 11: clinical audits — The requirement in this section is for two full cycle audits in the 5 year revalidation period. One audit needs to take place in years 1–3 and the other in years 3–5. They need to contain an initial audit, change implemented and the demonstration of improvement in the second audit.
Evidence area 12: statement on probity and health — GPs will be expected to verify a standard statement regarding probity and health; they may choose to provide an alternative statement. The statement must cover:
a declaration of a lack of probity issues in their work a statement that health issues do not impact on their work a statement that they are in a position to receive independent and impartial medical advice and evidence of medical indemnity cover
Evidence area 13: additional evidence for areas of extended practice — It is likely that some GPs will have nothing to add to this area. The GP should include all roles for which they receive regular remuneration. The RCGP highlight the following examples:
‘There is a group of common activities for which the evidence should be straightforward:
teaching of undergraduates — a statement from the university department vocational training — a statement from the postgraduate organization (deanery etc.) including the date and outcome of the last trainer approval visit research (including collaboration in research studies) — a statement from recognized research institution(s) involved and a statement from the Research Governance Team in the local Primary Care Organization (PCO) appraisers — a statement from the employing PCO and out-of-hours work — a statement from the out-of-hours provider’.
What will happen in the early years?
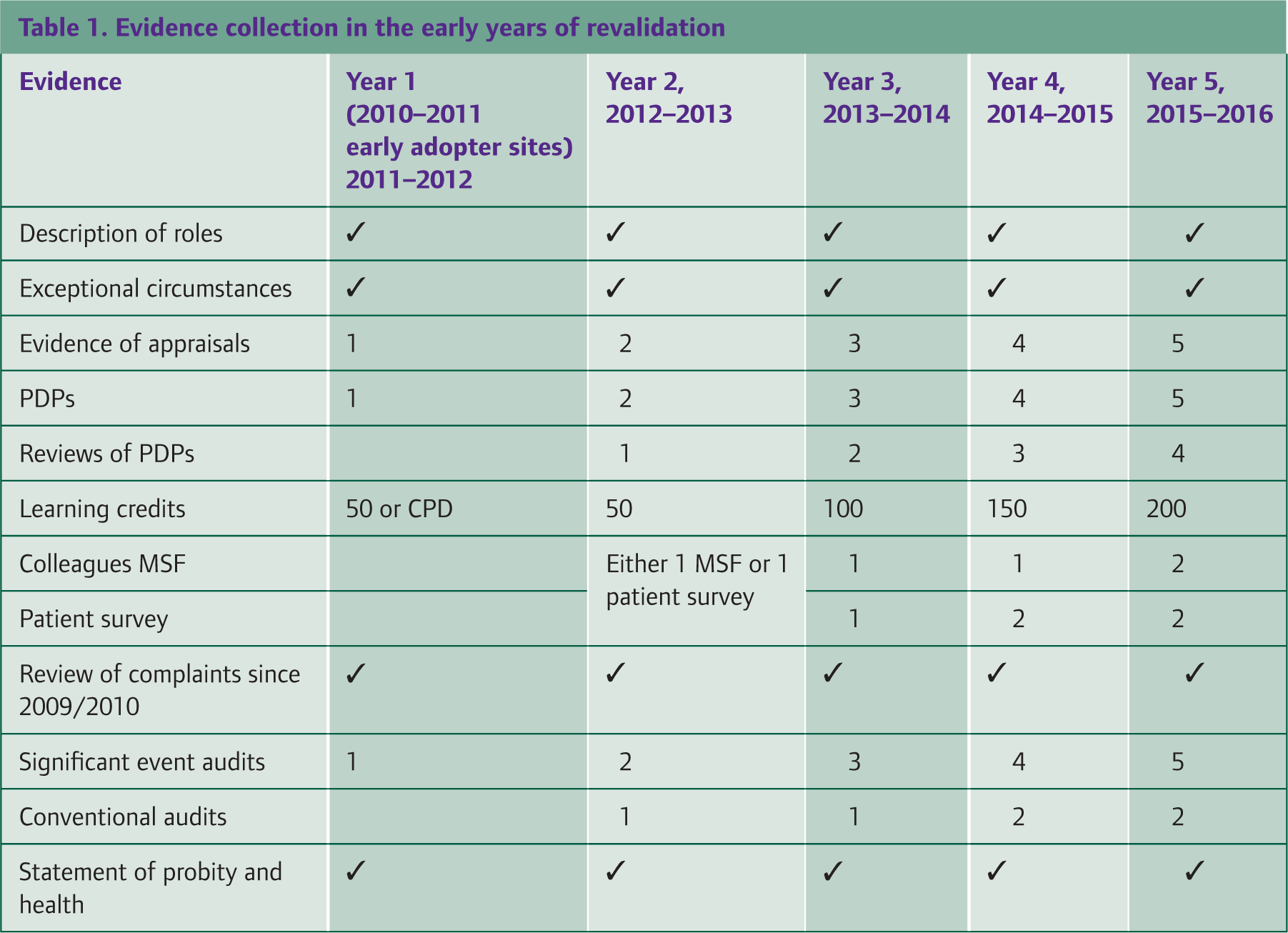
In the early years of revalidation, GPs may not have 5 years of evidence. It is still unclear how revalidation will roll out, and it is likely that some regions of the UK will be more ‘revalidation ready’ than others. The RCGP has addressed the issue of evidence. Its recommendations for the evidence required in the early years is reproduced in Table 1.
Evidence collection in the early years of revalidation
You mention CPD Credits, how will this system work?
The RCGP Credit-Based System for Continuing Professional Development is a mechanism for GPs to record their CPD based on the time spent on the activity and the impact it has on the doctor, their patients and the service. Credits are self-assessed and verified at appraisal and account should be taken of the need for GPs to use their CPD to ensure that they are up to date in all areas of their work. The system will help GPs meet their revalidation needs by providing a mechanism for collecting and demonstrating their CPD Credits.
At its simplest, each recorded hour spent on a CPD activity, which can include planning and reflection, counts as a credit. However, the RCGP has recognized that a wholly time-based credit system will not recognize the true value of CPD. A system based on the impact of a developmental activity and to a lesser extent the challenge involved in completing the activity was piloted between September 2008 and May 2009. Lessons learned as a result of that pilot informed the development of this system, which is based partially on time spent on the learning but with the opportunity to gain further credits by demonstrating the outcome (Impact) of the learning.
Impact in this context refers to:
Impact on patients (e.g. a change in practice, implementing a new clinical guideline, initiating a new drug for the first time) Impact on the individual (personal development e.g. development of a new skill or further development of existing skills) Impact on service (e.g. developing and implementing a new service, becoming a training practice, teaching others.) and Impact on others (teaching, training, National Health Service locally or nationally).
Impact, therefore, can be claimed for a range of clinical and non-clinical activities. An example of clinical impact is reproduced in Box 3. Non-clinical impact may be gained for example by becoming a training practice, teaching others, writing or reviewing an article or even developmental activities in a role within a PCO.
How will revalidation affect my relationship with my appraiser?
Many of the elements required for revalidation will be presented as evidence at appraisal. The appraiser will need to validate a number of items. This, in my mind, will strengthen the value of appraisal to the doctor. It is important to distinguish between the role of the appraiser in assessing some of the evidence and the role of the responsible officer (RO) making a revalidation decision. The evidence an individual collects during a revalidation period will not be presented to a single appraiser; two or more appraisers will be utilized in the 5 year cycle.
The doctor will require of their appraiser an objective judgement on the evidence. This judgement will need to be made against defined standards. The doctor and the appraiser will in fact be working together to ensure that the evidence presented at appraisal is of sufficient quality to meet the revalidation requirements.
Example of the way in which the credit system will work
A CPD Credit is defined as being based on an hour of learning activity (including planning and reflection) recorded in such a way that it demonstrates the learning achieved relevant to the working situation of the GP.
In its simplest form, 1 hour of activity equates to one credit. Credits are self-assessed, and although a certificate of completion or attendance may be used as evidence of activity, it is the demonstration of learning achieved and relevance to the work that the GP undertakes that defines the credit. In short, the RCGP does not advocate the collection of certificates, rather a collection of self-assessed-acquired knowledge relevant to the individual's working situation.
The acquisition of knowledge in itself does not necessarily lead directly to patient benefit; under this system, demonstrating impact is rewarded by a multiplication factor of 2 applied to time spent.
An individual attends a meeting (1 hour) on heart failure, acquires the knowledge that certain beta-blockers are beneficial in this condition and then records this within their appraisal documentation.
Credits claimed = 1 – this demonstrates the acquisition of knowledge and as yet there is no demonstration of personal, practice or patient benefit.
A different individual attends the same meeting. They record the same acquisition of knowledge; however, they include two patient case studies demonstrating the introduction of beta-blockers in heart failure.
Credits claimed = 1 × 2 (
A third individual attends the same meeting. The acquisition of knowledge is recorded, however in their appraisal folder an audit is planned after consideration of current practice (1 hour), they demonstrate audit of their patients with heart failure, changes are made appropriately following discussion with colleagues (1 hour) and a second audit cycle demonstrates an improvement in care.
Credits claimed = 1 (initial meeting (1 hour)) + 2 (planning (1 hour) and discussion associated with audit (1 hour)) × 2 (Impact) = 6.
It is my personal feeling that the appraiser should be asked to choose between validating a piece of evidence as sufficient or encouraging further work possibly through the PDP. I do not think that this will be a negative relationship, the supportive and educative role of appraisal can be maintained. In order to ensure this, there are three prerequisites:
appraisal training focusing on supporting individuals in this context the publication of explicit standards by which pieces of evidence will be judged. These standards will need to be illustrated using real-life examples. Individual GPs will need to understand the importance of appraisal in the revalidation process.
What proportion of GPs are likely to have insufficient evidence on appraisal?
I suspect that initially a minority of GPs may find it alien or difficult to supply the evidence. The important factor here would be the skill of the appraiser in negotiation with the individual over their subsequent year's PDP. Revalidation is a continuous process, and as such, if an individual is failing to produce evidence towards revalidation repeatedly, there will need to be mechanisms in place to identify such individuals at an early stage. Supportive resources such as tutors, examples of suitable evidence, CPD events and targeted mentoring need to be in place across the UK to a minimum level.
In the UK, revalidation for GPs will not rely on single pieces of evidence, the portfolio an individual presents may meet all the standard criteria however there are plans for non-standard portfolios of evidence (e.g. for those with short- or medium-term career breaks). These are detailed in the revalidation guide and the guidance will no doubt develop with time. The RO within the PCO will need to judge the adequacy of the portfolio of evidence. The portfolio will be judged against criteria developed by the RCGP and eventually agreed by the GMC.
The proportion of GPs who produce insufficient evidence can only be guessed at. I suspect that 10–20% may have non-standard portfolios. With support and remediation in place, the proportion that will fail to produce evidence sufficient for revalidation is likely to be lower than that.
What happens if I fail an appraisal?
Technically an individual cannot fail an appraisal. The revalidation guide describes a situation where an appraisal meeting takes place and the appraiser feels they cannot sign off the GPs participation as active and effective. In this situation, one such appraisal in a revalidation cycle may be acceptable if an investigation takes place locally. Two such appraisals in a revalidation cycle should trigger referral to the RCGP's national adjudication panel. This should ensure that consistent national standards are applied.
Who decides if I am to be revalidated?
This area is perhaps still less than clear; the current understanding is that a RO will be appointed by each PCO. This RO will be a senior clinician and is likely to be the medical director. It is envisaged that the RO will, in the case of GPs, sit with an RCGP representative, a lay person, and if the RO is not a GP, there may be an independent GP to give the RO advice. This panel would normally sample folders containing sufficient evidence and examine in detail any folders that have raised issues. The RO will decide what the final revalidation recommendation to the GMC will be.
What happens if I fail revalidation?
Again this is an area of uncertainty. It is likely that an individual will not fail revalidation but fail to produce sufficient evidence for a positive revalidation decision to be made. I think it must be reiterated that revalidation is not a method of policing performance, it is simply a mechanism for a doctor to produce sufficient evidence in order to maintain their professional right to practice. Remediation systems are proposed in both the White Paper and the Next Steps documents, yet they are neither available in each area across the country nor has a mechanism for funding been proposed.
Sessional GPs may find it difficult to collect evidence; do you have any comment on this?
It is quite obvious that the different working situations of many GPs will make evidence collection either easier or more difficult. GPs working in well-organized practices will find audit, MSF and patient surveys easier to obtain. A peripatetic locum or sessional GPs in unsupportive practices may find these processes more difficult. The RCGP has recognized this in the second iteration of the revalidation guide and make a number of practical suggestions within that second edition. It is clear that audit in the situation of the locum may need to be different when compared with the longitudinal care achieved in practice. Suitable subjects are being developed as part of pilot work within the RCGP.
Some GPs have little or no clinical contact-how will this affect them?
The Revalidation guide suggests a minimum of 200 sessions per 5 year period. The RCGP is working with the GMC to identify solutions for GPs with no clinical contact who still perform at a high level within primary care (e.g. medical directors of PCOs). I would refer individuals who are concerned that they may be engaged in non-standard general practice to the online revalidation guide.
Do you have any last thoughts to share regarding revalidation?
Personally I regard revalidation as a positive affirmation of practice. I have long involvement in CPD and to a lesser extent appraisal within the Wales deanery. I envisage that revalidation will strengthen the requirements for CPD and indeed as argued above, for appraisal. I believe that the quality management of the processes is vital. This will ensure that an appraisal decision in John O'Groats will match one in Lands End. The new generation of registrars achieving CCT through the nMRCGP should have no problems in collecting and demonstrating information. The previous generation-myself included-will initially find it alien to present evidence in this way; however, as with the numerous changes that happen in general practice, I am confident the profession will adapt.
Key points
Revalidation is the continuous process by which doctors will be given a positive affirmation of their right to practice once every 5 years In order to successfully complete the revalidation process, a GP will have to produce evidence of their fitness to relicense (medical register) and recertify (general practice register) Every doctor in the UK will be required to amass a portfolio of evidence of fitness to practice, probably in an electronic portfolio This evidence must cover each of the 12 attributes of the four domains of Good Medical practice set by the GMC, and will be reviewed every year at the GP's annual appraisal and The RCGP has proposed that a GP will be required to amass evidence in 13 categories over a 5 year period