
Abstract
The term ‘personality’ refers to the enduring characteristics which influence the way a person thinks, feels or behaves in a wide variety of circumstances. A personality is deemed to be ‘disordered’ when it causes suffering to that person or to other people. The Department of Health estimates that 10–13% of the adult population have personality disorders, and it is therefore extremely important that GPs are aware of current thinking regarding the classification, diagnosis and treatment of these complex conditions.
The GP curriculum and personality disorders
screen, diagnose and manage people experiencing mental health problems in primary care, using specific interventions and guidelines where appropriate
describe early indicators of difficulty in the psychological well-being of children and young people
describe how to engage and build a rapport with people experiencing mental health problems
understand that our own attitudes and feelings are important determinants of how we react to people with mental health problems
assess risk/suicidal ideation
describe how to deal with the uncertainty that certain patients produce, such as chronic suicidicity in borderline personality disorder (BPD)
describe when it is appropriate to refer to, and collaborate with, specialist mental health services
Classification
The classification of personality disorders has long been a subject of debate and dispute. Some feel that personality is a wide-ranging continuum and that labelling a personality as ‘disordered’ is arbitrary and unhelpful. However, it is clear that there are people whose position on the personality spectrum results in distress and disturbance in all aspects of their lives. Existing definitions of personality disorder therefore describe ‘a severe and pervasive disturbance in experience or behaviour which causes distress and significant impairment in social and occupational functioning’.
There are also those who believe that the process of organizing personalities into groups is impossible because personality, by definition, is the combination of characteristics that make an individual unique. However, it is evident that patterns of personality problems are shared by large groups of people and the International Classification of Disease (ICD-10) and Diagnostic and Statistical Manual (DSM-IV) systems classify personality disorders into a number of different categories (Table 1). Patients rarely fall neatly into just one category and DSM-IV has provided a useful solution to this problem by grouping the categories into three broad clusters: Cluster A ‘Suspicious’; Cluster B ‘Emotional and Impulsive’ and Cluster C ‘Anxious’.
Summary of DSM-IV classifications of personality disorder

Note: Generally, the same terms are used in DSM-IV and ICD-10. Where there are differences, the ICD term is shown in parentheses.
Diagnosis
Increasingly, research is demonstrating that people with personality disorders can, and should, be offered treatment. In the past, mental health services have focused on conditions such as depression and schizophrenia. However, recent National Institute for Health and Clinical Excellence (NICE) guidelines on BPD have emphasized the need for specialist personality disorder units within trusts. These guidelines also highlight the important role of primary care in recognition of suspected cases and crisis management, as well as appropriate and timely referral to secondary diagnostic and treatment services.
There are a number of different diagnostic tools used in specialist personality disorder services. These generally consist of semi-structured clinical interviews with scoring systems, such as the Structured Clinical Interview for DSM-IV Axis-II Personality Disorders (SCID-II). The patient fills in a detailed personality questionnaire and then discusses it with a trained interviewer who asks further questions and codes the patient's responses. The process is extremely time-consuming and obviously well beyond the scope of a general practice consultation.
We do not yet have the equivalent of the patient health questionnaire (PHQ-9) for depression, and making a suspected diagnosis of a personality disorder in primary care relies on identifying recognized patterns of behaviour. There has been some research into developing a screening tool, and the Iowa Personality Disorder Screen is an 11 question interview which can reportedly be carried out in 5 minutes. The authors’ published study was of only 52 subjects but found that when compared with a standard structured clinical interview, the Iowa screen, with a sensitivity of 79% and a specificity of 86% was ‘a promising tool’ warranting further study (Tyrer, 2000).
Co-morbidity
Separately identifying personality disorders in those with other mental health problems is extremely challenging, as most mental illness distorts pre-morbid personality and research is limited due to the lack of data recording personality status prior to the onset of mental illness. However, a number of strong relationships have been demonstrated and it is felt that co-morbidity is much more common than currently recognized. Improved identification of co-morbidity in primary care could result in more successful treatment and better prognosis for these patients.
For example, cross-sectional studies have shown a strong link between substance misuse and Cluster B personality disorders (see Table 1), particularly BPD and antisocial personality disorder. Eating disorders, particularly self-induced vomiting, are also associated with Cluster B personality disorders, while neurotic disorders such as agoraphobia, panic disorder and generalized anxiety are associated with the Cluster C disorders.
Post-traumatic stress disorder has been linked with BPD with the suggestion that the Cluster B disorders create, or at least predispose to, an increased rate of life events with subsequent adjustment disorders. The relationship between schizotypal personality disorder and schizophrenia has long been assumed but rarely shown in practice, again due to the lack of pre-morbid personality data. Interestingly, the rate of co-morbidity between BPD and depression is not nearly as great as one might expect and studies of patients with BPD have demonstrated that their diagnosis does not change to one of depression over time and they do not respond particularly well to antidepressants.
Borderline personality disorder
The rest of this article will focus on BPD, as it is a condition that is commonly encountered in primary care and creates enormous challenges, particularly in terms of maintaining the doctor—patient relationship and managing risk and uncertainty. It is also the most extensively researched of the personality disorders and the subject of recent NICE guidance.
Louise Williams/SPL.
Recognition in primary care
The American Psychiatric Association suggests nine diagnostic criteria, five of which should be met in order to reach a diagnosis of BPD (Table 2). Many GPs feel that they do not have the skills, training or resources to diagnose and provide ongoing care to patients with personality disorders. However, in primary care we are in fact uniquely placed to do both. We have the privilege of caring for patients from birth to adulthood and of caring for entire families. We therefore have insight into our patients' backgrounds and family relationships and may even have visited them at home. We can be a point of contact for concerned family members even if patients do not seek help themselves. We also receive information from other services, such as Accident and Emergency departments, hospital clinics and social services which, alongside our own experience of dealing with the patient, can be pieced together to suggest a possible diagnosis.
American Psychiatric Association diagnostic criteria for BPD

In patients with existing diagnoses of BPD, long-term attachment and stable support systems are crucial. Many lack this stability, both in their personal lives and in the chaotic (and often negative) encounters that they have with health care professionals. Most patients will not have continuous secondary care support and GPs therefore have an extremely important role in providing continuity of care and supporting patients through difficult transitions. We can also be a first point of contact at times of crisis, and coordinate managing the crisis for both patients and their families, paying particular attention to the needs of vulnerable children.
Case study
Ms J.G. is a 22-year-old, unemployed woman who comes to see you requesting a termination of pregnancy.
Her mother had come to see you the previous week regarding her own low mood and expressed concern that her daughter might be using drugs and was involved in a series of intense and sometimes violent sexual relationships, none of which lasted more than a few months.
From your background knowledge of the family, you know that Ms J.G. was sexually abused by her mother's partner as a child. When looking back through her notes, you also see two Accident and Emergency discharge summaries describing minor incidents of self-harm, usually following arguments with her partner.
You have seen Ms J.G. on a number of previous occasions and find that she is sometimes easy to talk to and sometimes difficult and uncooperative. You generally have a sense of unease and helplessness and feel that you are not managing to deal with the array of life crises that she places before you.
All the information taken together suggests a diagnosis of BPD and you decide to refer her to the local specialist personality disorder service for confirmation of this diagnosis and advice regarding treatment.
Aetiology
The term ‘borderline’ is misleading for patients and non-specialists alike. It originates from early psychoanalysis, when the condition was thought to be a pathology lying between neurosis and psychosis. Since then, there have been numerous attempts to explain it as a variant of an Axis I disorder, thereby redefining it as a condition with an established method of treatment. For example, there have been proposals that it is a variant of unipolar depression, a complex form of post-traumatic stress disorder and a variant of bipolar disorder. Evidence has not supported these theories and research is now focusing on BPD as a condition in its own right.
Studies investigating the aetiology of BPD have looked at biological, psychological and social factors (Table 3). Many take a multifactorial approach and believe that it arises from a mixture of innate temperament, challenging childhood experiences and neurological and biochemical dysfunction.
Aetiology of BPD

Over the past decade, research has focused on the importance of childhood experience and more particularly the primary attachment relationship between infant and caregiver in the subsequent development of BPD in later life. Recent studies are based on the ‘attachment theory’ of the 1960s, which stated that parents who were available and responsive to their infant's needs established a secure and dependable base from which that child could explore the world.
Research suggests that the ability to accurately recognize mental states in the self and others develops in the context of these early attachment relationships. Failure to form these relationships in early life results in this process being undermined and inadequate ‘mentalization’ in adulthood. Inadequate mentalization is thought to explain a number of the behaviours displayed in BPD, including the process of ‘splitting’, whereby patients are unable to integrate the good and bad aspects of both the self and the others.
Professionals are therefore viewed as all good or all bad at different times, depending on whether they are gratifying a patient's needs or frustrating them. This can be extremely challenging and create friction both within the doctor—patient relationship and between professionals. Recognizing that ‘splitting’ occurs, and understanding why, is extremely important in order to minimize its impact on the stability that a patient with BPD so desperately needs.
Crisis management in primary care
maintain a calm and non-threatening attitude
try to understand the crisis from the patient's point of view
explore the patient's reasons for distress using empathic open questioning, including validating statements
avoid minimizing the patient's stated reasons for the crisis
assess risk to the patient and others: ask the patient directly about deliberate self-harm and suicidal ideation; use experience of previous crisis behaviour and discuss level of risk with other involved professionals
ask about previous episodes and effective management strategies used in the past
the patient may have a personal ‘Crisis Plan’ which can be consulted
seek to stimulate reflection about solutions and encourage the patient to identify manageable changes that will enable them to deal with the current problems
consider cautious, short-term use of sedative drug treatment (see below)
offer appropriate follow-up within an agreed timeframe
explore community-based options, such as crisis resolution and home treatment teams, or other locally available alternatives to admission
only consider admission to an inpatient ward if risk cannot be managed effectively in the community
the decision to admit should be based on an explicit joint understanding of the potential benefits and likely harm that may result from admission
the length and purpose of admission should be agreed in advance
in extreme circumstances, patients with personality disorders
Service provision
The provision of services for patients with personality disorders can be divided into tiers, illustrated by Fig. 1. The recently published NICE guidance on BPD clarifies the roles of health care professionals at the lower service tiers.
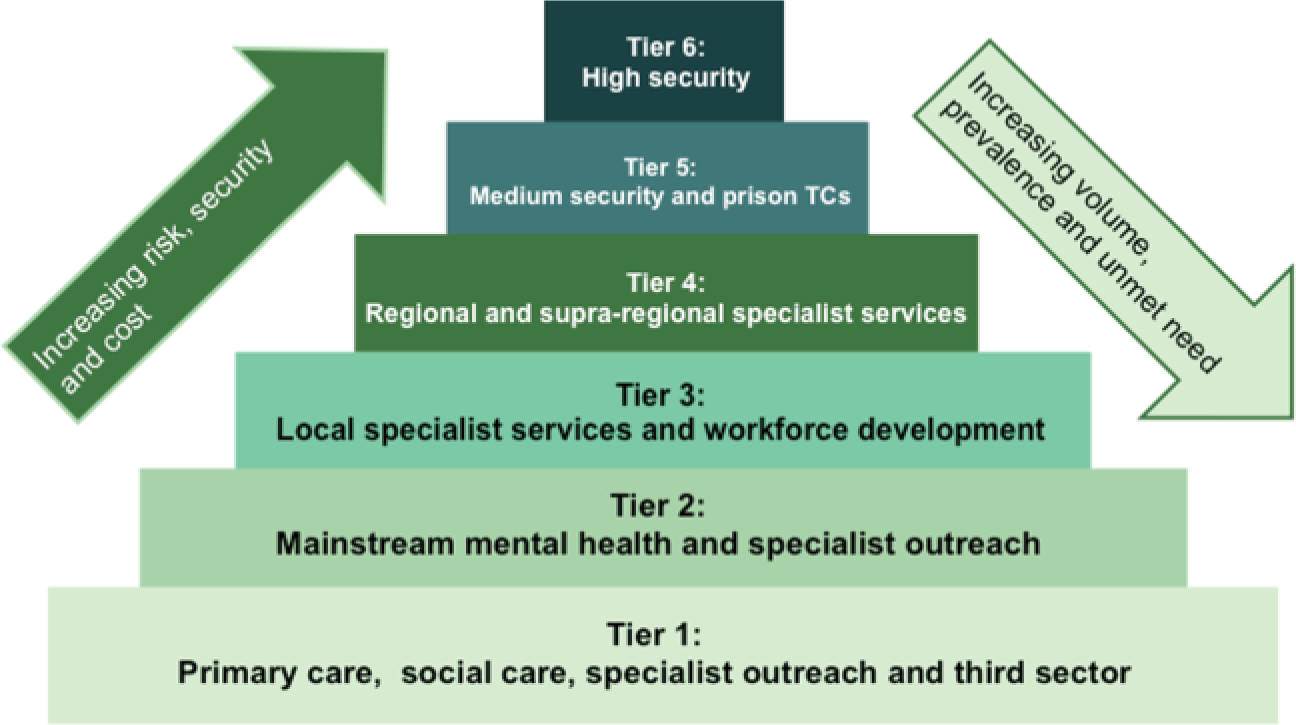
Service tiers for personality disorders.
In primary care, we are expected to be actively involved in the recognition of BPD. We are also required to initiate appropriate referral to mental health services but clearly we cannot refer every patient with features of BPD, as the numbers would be overwhelming. There are no clear guidelines indicating which patients to refer and which to manage in primary care, but the general impression is that, given recent developments in treatment and specialist service provision, we should have a lower threshold for referring. A referral should be considered if
we feel that the condition is significantly impairing social, occupational or other important areas of functioning or
if levels of risk or distress are increasing/failing to subside or
if a patient requests specialist input
Crisis management is our third key area of involvement (Box 1). We should be able to assess current levels of risk to self or others (particularly dependent children) and discuss management strategies (with the patient, with relatives and with other professionals in the primary and secondary health care teams). We should arrange appropriate follow-up and refer on to mental health services if the crisis is failing to subside or the levels of risk are increasing.
If a patient is referred to the community mental health services, a full assessment should be carried out by them, which should address:
psychosocial and occupational functioning
co-morbid mental disorders
the need for psychological treatment/social care/occupational rehabilitation and
the needs of dependent children
A multidisciplinary care plan should then be developed which is shared with the GP and patient. This should clarify the roles of professionals involved and include long- and short-term treatment aims and crisis plans.
Local specialist services should act in their traditional way as a point of call for colleagues in both primary and secondary care, providing diagnostic services and advice, as well as psychological and social interventions for patients with particularly complex needs or high levels of risk. However, in addition, NICE suggests that specialist adult services should:
monitor provision of services for minority ethnic groups to ensure equality of service delivery
work with child and adolescent mental health services to develop transition protocols for children and young people moving into adulthood
support, participate in and lead local and national development of treatments including multi-centre research and
develop training programmes on diagnosis and management of BPD and implementation of guidelines
Psychological management
A number of different psychological treatments are available for patients with personality disorders. Certain patients will respond better to certain forms of therapy but it is generally agreed that brief psychological intervention (of less than 2 months) is not recommended.
NICE suggests that deciding which treatment to use should be based on a number of factors. These include: the choice and preference of the patient; the degree of impairment/severity of disorder; the willingness of the patient to engage with therapy and the patient's motivation to change; the ability of the patient to remain within the boundaries of a therapeutic relationship and the availability of personal and professional support.
Some patients may benefit from straightforward counselling or cognitive behavioural therapy, which can be provided in the primary care setting. Specialist services may use specific forms of psychotherapy such as mentalization-based treatment (MBT). This is based on the idea that a core problem in BPD is the limited ability to perceive mental states in the self or others accurately, which can be improved with specific therapy.
Dialectical behaviour therapy (DBT) is another approach, which combines cognitive behavioural therapy techniques with ‘mindful awareness and distress tolerance’. The programme involves individual therapy and group work focusing on behavioural skills training. There are also a few remaining National Health Service-run inpatient therapeutic communities where residents are involved in group discussions and individual therapy and share responsibility with staff for tasks and decisions.
Drug treatment
Drug treatments are not recommended for the general management of BPD; however, cautious short-term use of sedative medication is acceptable during crises. NICE advises that this should be for no longer than a week and that a single drug should be used initially, such as a sedative antihistamine. Before prescribing, consider risks such as alcohol and illicit drug use, as well as the risk of overdose. A plan should be agreed with the patient including monitoring and anticipated duration of treatment, and there should be communication and agreement between the professionals involved (such as the GP and Community Mental Health Team).
Natural history
BPD was only formally recognized as a diagnosis in 1980. Since this time, it has been commonly thought that the disorder ‘burns out’, with manifestations becoming less apparent in the fourth and subsequent decades. More detailed investigation suggests that although impulsivity certainly appears to decline with age, affective disturbances and interpersonal difficulties remain problematic. These, although less alarming for clinicians, can be equally disabling for patients.
Key points
Personality disorders are common, affecting 10–13% of the adult population
They are no longer considered ‘untreatable’ and recognition in primary care and appropriate referral is therefore extremely important
Making a suspected diagnosis in primary care currently relies on recognizing typical behaviours but there may be a role for screening questionnaires in the future
Co-morbidity between personality disorders and other mental health conditions is common and under-recognized
There is a tiered approach to provision of services for personality disorders, and the roles of health care professionals at each tier have been clearly defined by recent NICE guidance on BPD
The management of BPD is mainly psychological, with drug treatment having a limited role during crises
Footnotes
Acknowledgements
I thank Dr Az Hakeem, Consultant Psychiatrist, Personality Disorder and Forensic Psychotherapy, The Dartmouth Park Unit and The Portman Clinic, and Dr Stephen Amiel, GP Partner, The Caversham Group Practice.