
Abstract
Constipation in childhood is a common problem that is frequently seen in general practice. Constipation can be defined as an infrequent passage of stool or difficulty passing stools. The term also encompasses distress on defecation and a feeling of incomplete evacuation. The aims of this article are to provide an overview of how to approach constipation in general practice. This approach will include how to diagnose constipation, consideration of predisposing factors, treatment options and when to refer.
The GP curriculum and childhood constipation
Childhood constipation features as one of the conditions in the knowledge section of
GP trainees are expected to be able to provide parents and children with information to allow them to manage minor illnesses, such as constipation, themselves. GP trainees should be able to recognize delayed development and failure to thrive, both of which can be associated with constipation. They need to be able to prescribe safely for children, including calculating the correct doses and considering the risks and benefits of using medications.
What is constipation?
Constipation is common during childhood. It is thought that in the UK 5% of school children aged 4–11 years experience constipation lasting more than 6 months. These children and their families will require regular advice and help from their G P.
Frequency of bowel function and what is normal for a child varies among individuals. In children, frequency of bowel movement decreases with age. In babies of up to 3 months of age the average number of bowel movements is three per day if breastfed and two per day if formula fed. This gradually decreases with age so that a child over 3 years old will have an average of one bowel movement per day. However, it is entirely normal for breastfed babies not to have a bowel movement for several days. Generally, if the child is not in pain or distress, then a degree of infrequency of bowel movements is likely to be normal. Signs of straining in infants can also be normal, as children only gradually develop the muscles to assist bowel movements.
Constipation in childhood is usually functional. Functional constipation is constipation without a known cause. Secondary, or organic, constipation is constipation due to either an underlying medical condition or a drug. Recently, there have been attempts to agree criteria for the definition of functional constipation. These include the Rome Criteria III and the Paris Consensus on Childhood Constipation Terminology (PACCT). The following definitions in Box 1 are based on PACCT.
Definitions of constipation
Frequency of bowel movements less than three per week
More than one episode of faecal incontinence per week
Large stools in the rectum or palpable on abdominal examination
Passage of stools so large that they may obstruct the toilet
Display of retentive posturing and withholding behaviours
Painful defecation
Organic faecal incontinence is faecal incontinence resulting from organic disease, e.g. neurological damage or sphincter abnormalities
Functional faecal incontinence is faecal incontinence without organic disease that may be constipation associated or non-retentive faecal incontinence (non-constipation associated)
Overflow incontinence is the passage of loose stool around impacted faeces
Secondary constipation
If the child is more than 1 year old, then 95% of symptomatic individuals will have functional constipation. However, in infants and neonates constipation is much more likely to have an organic cause and it is important to ensure that the potential causes are excluded. Box 2 lists the most common secondary causes of constipation.
Causes of secondary constipation
Hirschsprung's disease
Cystic fibrosis
Metabolic conditions, e.g. hypothyroidism and
hypercalcaemia
Neurological disorders, e.g. cerebral palsy
Spinal cord abnormalities, e.g. spina bifida
Anorectal abnormalities, e.g. imperforate anus and anal
fissure
Cows' milk intolerance
Heavy metal poisoning, e.g. lead
Drugs
antiepileptics, e.g. carbamazepine, gabapentin and phenytoin
sedating antihistamines
opioids
oxybutynin
Hirschsprung's disease is absence of parasympathetic ganglion cells in the myenteric and submucosal plexus of the large bowel. It occurs in 1 in 5000 children. This usually presents with failure to pass meconium within 48 hours of birth. Abdominal distension and bile-stained vomiting can occur. In later childhood, it can present as chronic constipation that is resistant to usual treatments. In these older children there may be abdominal distension but there is not usually faecal incontinence. Growth failure can also occur with Hirschsprung's disease.
Congenital anal malformations such as imperforate anus may be present and can be diagnosed by external examination of the anus. Cystic fibrosis should be suspected in a child with failure to thrive, constipation and recurrent chest infections. Hypothyroidism should be suspected in children with constipation, failure to thrive, cold intolerance and bradycardia. Spinal cord abnormalities may be evident. For example, a dimple in the skin or tuft of hair could indicate spina bifida.
In children older than 1 year, functional constipation is most likely. In these situations it is important to consider what may have precipitated the constipation. Box 3 lists factors that may be contributing in functional constipation.
Factors predisposing to constipation
Low-fibre diet
Dehydration because of poor fluid intake or an acute febrile illness
Obesity
Lack of physical exercise or immobility
Withholding behaviour
Children may withhold defecation by contracting their external anal sphincter and pelvic floor muscles. Children may withhold defecation for a number of reasons. There may be fear of pain associated with defecation, for example, due to anal fissures, perianal skin infection or passage of hard stools. Children may also withhold if there is coercive toilet training. Withholding may be because of restricted access to toilets or fear of using toilets, such as at school or because of limited privacy. Psychological stress, for example, following bereavement or moving house, can contribute. Sexual abuse is a rare cause of withholding but it is important to consider it.
Complications of constipation
Chronic constipation can lead to faecal retention and distension of the rectum. A rectum loaded with faeces over time dilates and habituates to distension so that the sensation of the need to defecate is lost. A distended rectum contracts regularly causing a reflex relaxation of the internal sphincter. This allows any soft stool around the internal sphincter to leak and cause faecal incontinence. It should be explained to the parents in these cases that the incontinence is involuntary. It may take some time for recovery of normal rectal size and for normal sensation to return.
Faecal loading and impaction not only leads to faecal incontinence but also leads to urinary tract infections, anal fissures and rectal prolapse. It can also result in school refusal and other problematic behaviour.
History, examination and investigations
It is important to take a detailed history from the child and parents. You need to ascertain what exactly they mean by constipation. Constipation can be diagnosed if there is infrequent or difficulty in passage of stools. The stools may be large or small. Parents may also notice their child has a poor appetite, lacks energy or appears irritable. The child may have abdominal pain or pain on defecation. If there is faecal incontinence, then suspect impaction and overflow faecal incontinence. Rectal prolapse is common if there is severe constipation with straining but this can also be a sign of cystic fibrosis or inflammatory bowel disease.
In infants it is important that the perineum is inspected to exclude an anorectal abnormality. An imperforate anus should be checked for and the position of the anus should also be inspected. The normal position is midway between the coccyx and posterior part of vulva or scrotum. Erythema of the perianal skin may be present. This could be a sign of streptococcal infection of the perianal area, which is common in infants. It is associated with sudden onset of painful defecation together with inflammation and reddening of the perianal skin.
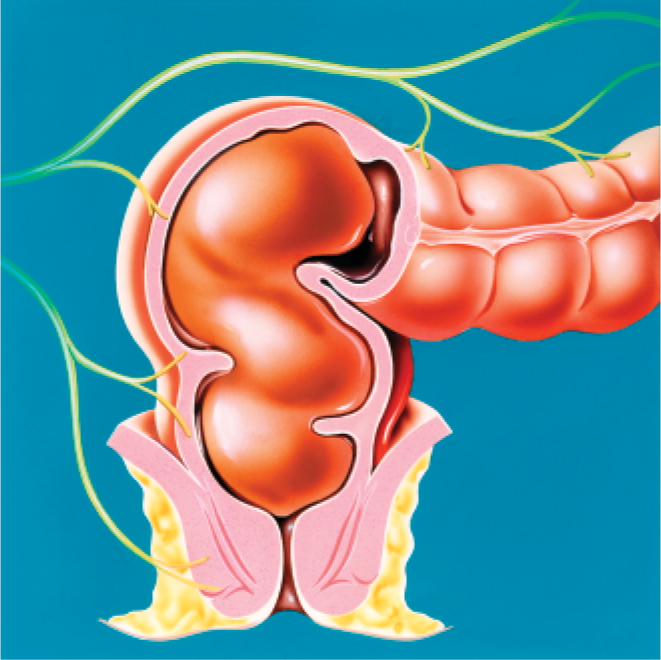
Faecal impaction.
In primary care, internal rectal examination is rarely necessary. However, hard faeces in the rectum can often be felt on perianal or abdominal palpation. Anal fissures are often associated with fresh red blood on the nappy or paper on wiping. A clue pointing towards an anal fissure is the finding of skin tags on examination. In older children with fissures, it is important to consider if there may be associated inflammatory bowel disease. If there is rectal bleeding but no fissure then the child should be referred as this could be a sign of Meckel's diverticulum or inflammatory bowel disease.
A neurological examination and inspection of the spine is important to exclude causes such as cerebral palsy or spina bifida. It is important to use a growth chart to exclude failure to thrive, which may, for example, be a sign of cystic fibrosis or hypothyroidism. No investigations are usually necessary unless an organic cause of constipation is suspected. If all causes of secondary constipation are excluded, then functional constipation can be diagnosed. Box 4 lists questions to ask when taking a history from a child with constipation.
Management
The most important initial step before commencing any treatment is to ensure that the constipation is not secondary to an undiagnosed underlying condition. This should include stopping any potentially constipating medicines, treating any painful anal condition and addressing psychological causes.
Constipation can be difficult to cure and sometimes requires years of treatment. One recent study by Borowitz et al. (2005) found that after 2 months of treatment 40% of constipated children remained symptomatic. Acute constipation therefore needs to be treated promptly to prevent it developing into chronic constipation. The study also found that primary care doctors tend to undertreat constipation and found that children treated more aggressively were more likely to respond to treatment. It is thought that more than 3 days gap between passage of stool is enough to cause pain on passing stool and lead to anal fissures. This eventually results in a learned response to avoid defecation. Faecal impaction needs to be diagnosed and cleared if present. A regular bowel pattern needs to be established with bowel movements once or twice a day in which the stools are soft and passed without discomfort. Treatment needs to be continued longer term if impaction was present, to prevent recurrence of symptoms.
History
What does the patient mean by constipation
Frequency and consistency of stools
Size of stools
Any associated pain or bleeding
How long has the child had symptoms
Diet and fluid intake
Any contributing medication
Behaviour at time of opening bowels
Any soiling
Any rectal prolapse
Did they have the neonatal blood spot screening (includes testing for cystic fibrosis and hypothyroidism)
Is growth normal
Delayed passage of meconium or in older children abdominal distension
Recurrent chest infections
The child and parents need to understand the diagnosis and be involved in agreeing the management plan. Constipation can be stressful for the parents. Reassuring parents that constipation is common and can be resolved is often useful. Guiding the child and his family towards other resources can help them manage the problems themselves. One example is the website for Education and Resources for Improving Childhood Continence (ERIC) at www.eric.org.uk.
Treatment
Infants under 1 year old
Treatment of infants will depend on whether they have started weaning. If unweaned and bottle-fed, then the parents can be advised to give extra water between feeds but not to dilute the formula. Rarely, there may be cow's milk intolerance causing the constipation. If this is suspected, then hydrolysed or hypoallergenic milk formula can be trialled. Bicycling the infant's legs or abdominal massage may also help. If the infant is breastfed, then constipation is unusual and an organic cause is likely. In breastfed infants, the mother should be encouraged to continue breastfeeding.
In infants who have begun weaning, encourage extra fluid either as water or as diluted fruit juice. Fruits with a high sorbitol content can also help (e.g. apples, pears, grapes and prunes) and high-fibre cereals for older infants.
For all infants, if the above measures fail, then consider prescribing an oral laxative. First line would be an osmotic laxative such as lactulose. Glycerol suppositories may be used to clear faecal impaction. The infant should be referred to a paediatric specialist if these measures fail.
Treatment of children over 1 year old
As with younger children, the initial management of constipation in children 1 year old and above is to increase fluid and fibre intake. Unprocessed wheat bran or oat bran can be added to food or fruit juice. Alternatively finely ground bran can be taken as bran bread or biscuits. Advise the parents about the importance of regular meals, optimal fluid intake and exercise. Encourage parents to try and minimize any stress and conflict associated with toileting and establish a regular toileting routine where the child does not feel hurried. Explain the reasons behind constipation and faecal incontinence and that the child should not be blamed. If constipation continues despite dietary measures, consider using laxatives. If there is faecal impaction and overflow incontinence, then it is unlikely that dietary measures alone will cure the constipation.
Laxative use
The following advice on laxative use in children is based on recommendations from the British National Formulary for Children (2009).
Bulk-forming laxatives
Bulk-forming laxatives such as ispaghula husk can be used to increase the dietary fibre intake. They work by increasing the faecal mass, which then stimulates peristalsis. It is important to ensure that there is a good fluid intake with bulk-forming laxatives to avoid intestinal obstruction. Bulk-forming laxatives can take several days to work. They are often difficult to administer to children. They are generally not advised for younger children. For example, ispaghula husk is not licensed for use in children under 6 years except on specialist advice.
Osmotic laxatives
If measures to increase fluid and fibre intake are not sufficient to cure the constipation, an osmotic laxative containing macrogols or lactulose can be used. Osmotic laxatives work by increasing the amount of water in the large bowel. This is achieved either by drawing fluid from the body into the bowel or by retaining the fluid with which they were administered. Lactulose is a disaccharide, which is not absorbed from the gastro-intestinal tract. It can take up to 48 hours to act. Macrogols are inert polymers of ethylene glycol, which sequester fluid in the bowel. It is important to give fluid with macrogols to try and reduce the dehydrating effect that can otherwise occur.
Stimulant laxatives
Stimulant laxatives increase intestinal motility. If there is evidence of minor faecal retention, the addition of a stimulant laxative may overcome withholding but may lead to abdominal cramps or, in the presence of faecal impaction in the rectum, an increase of faecal overflow. They are contraindicated in intestinal obstruction. Stimulant laxatives include bisacodyl, sodium picosulphate, senna and dantron (danthron). The indications for dantron are limited to constipation in terminally ill children because of its potential carcinogenicity. Docusate sodium probably acts both as a stimulant and as a softening agent. Glycerol suppositories act both as a lubricant and as a rectal stimulant because of the mildly irritant action of glycerol.
The British National Formulary (BNF) for Children advises that stools should be softened by increasing dietary fibre and fluids or with an osmotic laxative before giving a stimulant laxative. In chronic constipation, especially where withholding of stool occurs, additional doses of a stimulant laxative may be required. Long-term use of stimulant laxatives is sometimes necessary but excessive use can cause diarrhoea and related effects such as hypokalaemia.
Faecal impaction
In children with faecal impaction, macrogols such as Movicol Paediatric Plain are used to clear out the bowel and overloaded rectum. It is important not to use stimulant laxatives initially in children with faecal impaction without first making sure that the rectum is completely cleared as this can worsen soiling. If faecal impaction is not successfully treated with macrogols, then referral to hospital may be necessary. Administering enemas can be stressful for children and may in itself lead to withholding. Because of this they are used only when other methods have failed and are usually given under sedation in hospital. Alternatively, a bowel cleansing solution can be tried. In severe cases, or where the child is afraid, manual evacuation under anaesthetic may be appropriate. Long-term regular use of laxatives is essential to maintain well-formed stools and prevent recurrence of faecal impaction.
Movicol Paediatric Plain is not licensed for use in faecal impaction in children under 5 years, or for chronic constipation in children under 2 years. However, it is generally accepted that, if clinically appropriate, it can be used in younger children and the BNF for Children includes a suitable dose for a child 1 year old or above.
Chronic constipation
It is important to use laxatives such as lactulose or macrogols regularly after faecal impaction to prevent recurrence. This will help to keep the stools soft and prevent painful defecation. A high-fibre diet should be continued. If withholding recurs, it may be necessary to add a stimulant laxative. Parents and carers of children should be advised to adjust the dose of laxative in order to establish a regular pattern of bowel movements in which stools are soft, well-formed and passed without discomfort. The dose should only be reduced if the stool is too loose or too frequent. The time at which laxatives are likely to have an effect should fit in with the child's toileting routine. Some children require additional doses of a stimulant or osmotic laxative every 4 days or at weekends to ensure complete emptying of the rectum and regular bowel movements.
Management of anal fissures
Anal fissures should be treated with a stool softener and the short-term use of a topical preparation containing a local anaesthetic. Topical local anaesthetics can be absorbed through the rectal mucosa and can cause sensitisation of the anal skin. They should only be used to relieve the pain of an anal fissure for a maximum of 3 days. Local anaesthetics can cause stinging initially and this may aggravate the child's fear of pain. Children with chronic anal fissures should be referred to see a specialist. At this point a topical nitrate may be used or surgery might be considered.
Behavioural therapy
Behavioural therapy may be considered in order to address the psychological aspects of constipation and to help establish a pattern of regular defecation. The parent or child can be asked to keep a diary of stool frequency. This can be combined with a reward system for the child for adhering to toileting routines, taking medication and for successful defecation.
When to refer?
Refer for assessment by a specialist when
An underlying organic cause is suspected (e.g. distended abdomen, failure to thrive and blood and/or mucus in stools)
Treatment is unsuccessful
There are more severe psychological issues either causing or as a consequence of the constipation
Faecal incontinence or rectal prolapse is frequent
There is severe faecal impaction needing treatment
There are chronic anal fissures
Childhood constipation may continue beyond puberty in up to one-third of children. Children aged 2–4 years have a higher rate of recurrence and require more prolonged treatment and support than younger children.
Key points
Childhood constipation is common
Chronic constipation can lead to complications such as overflow incontinence, rectal prolapse, anal fissures and urinary tract infections
In neonates and infants, a secondary cause is likely and needs to be carefully excluded
In children over 1 year old, functional constipation is most likely
All children should receive lifestyle advice, including increasing fluid and fibre intake and regular exercise
Children are often undertreated and families need to be aware that laxatives can take a few days to work
Faecal impaction is initially treated with macrogols
Consult the BNF for Children for advice on which laxatives can be used at different ages and for correct dosages