
Abstract
Depression is the most common mental illness in the elderly, with an estimated 15% of the elderly population living in the community having clinically significant depressive symptoms. It is of medical and social importance as it is associated with increased morbidity and mortality, poor quality of life and increased social dependence. Recognition of depression in this age group has been found to be poor, with more patients presenting with somatic physical symptoms. Treatment can also be difficult compared with younger patients, with increased prevalence of side effects of medication, polypharmacy and poor compliance. Primary care practitioners are therefore crucial in the detection and early instigation of appropriate treatment. This article looks at the risk factors, presentation and treatment options for depression in the elderly age group.
The GP curriculum and depression in the elderly
Knowledge of the holistic bio-psychosocial ‘whole’ that is the patient
Understanding of the physical, psychological and social changes that may occur with age and relating them to the adaptations that an older person makes and to the breakdown of these adaptations
Understanding of the special factors associated with drug treatment in the elderly
Effective screening and diagnosis of patients with mental health problems and awareness of patients at risk of developing disease using appropriate screening tools
Knowledge of management of mental health conditions, including medication and talking therapies
Knowledge of when to refer to specialist care
Knowledge of the principles of mental health promotion
Definitions
The definition of ‘the elderly’ varies somewhat but is generally taken to be older than 65 years, although in some definitions older than 55 or 60 years, with the ‘old-old’ being over 75 or 80 years. There are also various mood disorders under the umbrella of ‘depression’ according to International Classification of Disease (ICD-10) criteria: mild, moderate or severe depressive disorder, dysthymic disorder, depression within bipolar disorder, organic depressive disorder and psychotic depression (Box 1). Furthermore, within the depressed elderly, an episode can be a first presentation or a recurrence of depression experienced at a younger age.
Aetiology and pathophysiology
The aetiology of depression in later life is complex. There are various neurological, biological, social and personality factors that contribute to the development of a depressive episode. Some of these risk factors are similar to those for depression at any age; however, there is some evidence that development of depression in later life should be looked at as a distinct clinical entity as there are aetiological factors that are specific to this age group. It is important that primary care practitioners are aware of these pathological processes and risk factors as they have implications for prevention and screening in high-risk groups of patients and a basic understanding will help when considering treatment options.
Neurobiological vulnerability
The neurobiological control of mood and emotion has been the subject of much research in recent years. It is thought that affective regulation is governed by several limbic and prefrontal structures and their interconnecting circuits, including the amygdala, the hippocampus and areas of the prefrontal cortex, anterior cingulate cortex, ventral striatum and the nucleus accumbens. Their locations and putative roles are shown in Fig. 1.
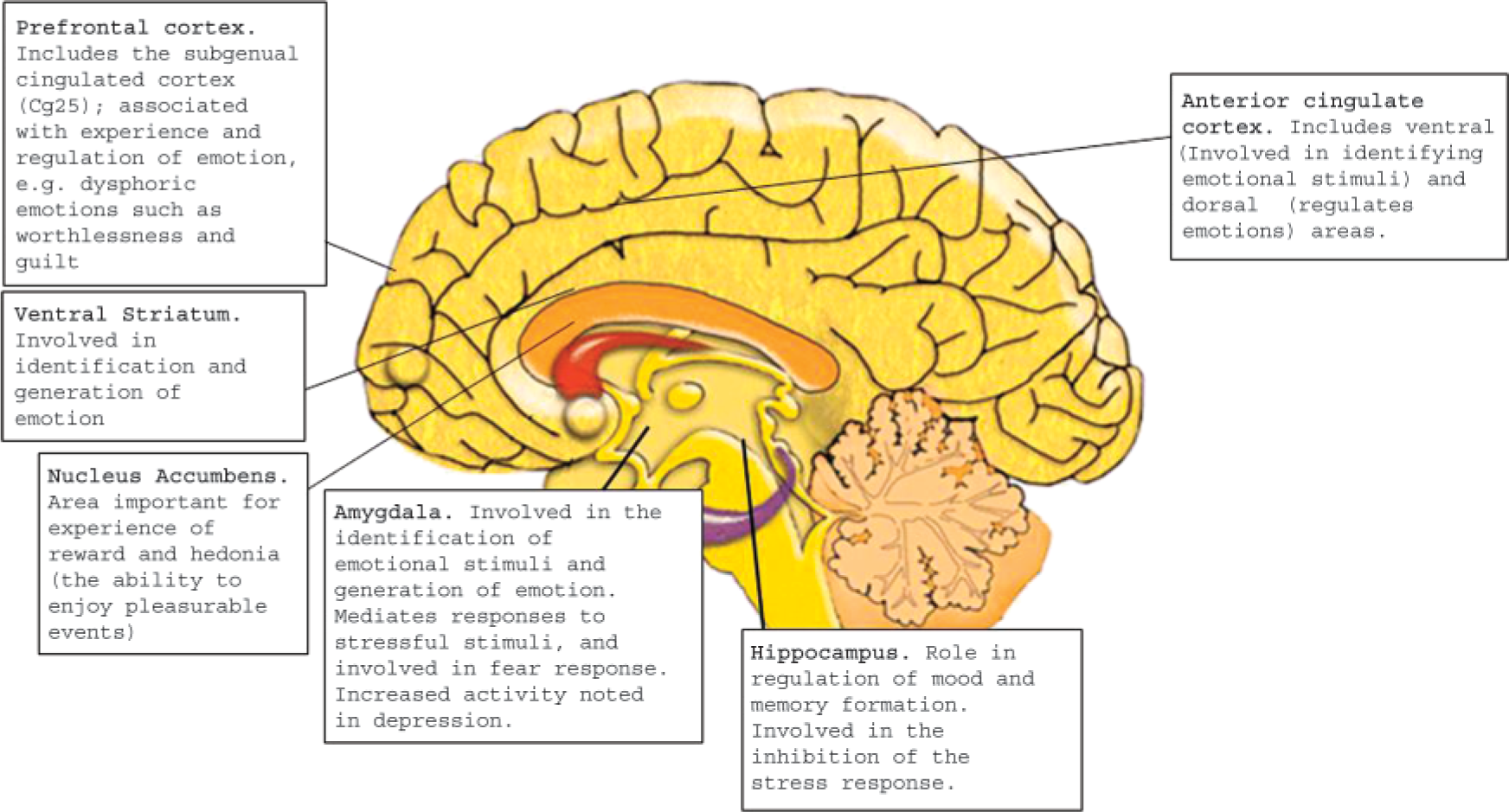
Important structures within the brain that are involved in the regulation of mood and their putative roles.
ICD-10 symptoms and diagnostic criteria for depressive disorders
Lowering of mood
Reduction of energy
Decrease in activity
Capacity for enjoyment, interest and concentration is reduced, and marked tiredness after even minimum effort is common
Sleep is usually disturbed and appetite diminished
Self-esteem and self-confidence are almost always reduced
Ideas of guilt or worthlessness
Mood is unresponsive to circumstances
‘Somatic’ symptoms: such as loss of interest and pleasurable feelings, waking in the morning several hours before the usual time, depression worst in the morning, marked psychomotor retardation, agitation, loss of appetite, weight loss and loss of libido.
Two or three of the above symptoms are usually present. The patient is usually distressed by these but will probably be able to continue with most activities.
Four or more of the above symptoms are usually present and the patient is likely to have great difficulty in continuing with ordinary activities.
An episode of depression in which several of the above symptoms are marked and distressing, typically loss of self-esteem and ideas of worthlessness or guilt. Suicidal thoughts and acts are common and a number of ‘somatic’ symptoms are usually present.
An episode of depression as described above but with the presence of hallucinations, delusions, psychomotor retardation or stupor so severe that ordinary social activities are impossible.
Recurrent episodes of depression as described above and without episodes of mood elevation (mania).
A chronic depression of mood, lasting at least several years, which is not sufficiently severe, or in which individual episodes are not sufficiently prolonged, to justify a diagnosis of severe, moderate or mild recurrent depressive disorder.
Currently displaying symptoms of depression as above and has previously had at least one authenticated manic, hypomanic or mixed affective episode in the past.
Disorders characterized by a change in mood or affect, usually accompanied by a change in the overall level of activity, depressive, hypomanic, manic or bipolar but arising as a consequence of an organic disorder.
In depression there is disruption to these structures and the circuits that connect them. For example, post-mortem examinations of depressed patients have shown a decrease in grey matter of the hippocampus and prefrontal cortex, while there is increased activity in the amygdala. Recent research into late-life depression has theorized that structural vascular changes within the brain may be responsible for this disruption, and it has been shown that areas such as the hippocampus are particularly vulnerable to age-related changes. Studies have found that patients with late onset depression are more likely to have cerebrovascular disease, and rates of depression in patients after a cerebrovascular accident are high. However, these vascular changes, while common, are not universal and are thus thought to predispose patients to the development of depression rather than inevitably cause it.
Generation and regulation of emotions within these pathways and structures are also in part mediated by the monoamine group of neurotransmitters: noradrenaline, dopamine and serotonin. A decrease in the function of these neurotransmitters has been found in depression, and current antidepressants work to increase their transmission, for example, by preventing their reuptake into neurons [selective serotonin reuptake inhibitors (SSRIs)].
Social factors
Several social factors are important risk indicators in this age group, with increasing prevalence in the elderly:
Social isolation/loneliness
Bereavement
Low socio-economic status
Caring role
Low educational achievement
Recent bereavement puts patients at high risk of subsequently developing depression, tripling the risk compared with the non-bereaved. Negative emotions will almost always be experienced after loss, but symptoms lasting for more than 2 months may be suggestive of a depressive disorder. Other stressful life events can also be a risk, such as financial difficulties or a change in living arrangements. A good social network is protective, and factors that disrupt this such as chronic illness, poor mobility and loss of function, poor social support and bereavement predispose to depression.
Many older people find themselves in carer roles. This also carries a high prevalence of depression, and around 40% of informal carers of patients with chronic disabilities, such as dementia, Parkinson's disease (PD) or stroke have levels of psychological distress in keeping with depression. Again, having a supportive social network is protective against development of depression.
Gender
Women are twice as likely as men to develop depression in this age group, and this contributes to the finding that depression is more common in the ‘old-old’ as they are more likely to survive to this age and outlive their partner.
Poor physical health
It is known that chronic medical illness of any kind can increase the likelihood of a patient developing depression, with rates of depression as high as 25%. There are complex interactions between physical and mental health in the elderly that are important for health practitioners to be aware of. Hormonal changes such as hypercortisolaemia occur in chronic medical illness, and this leads to stimulation of the amygdala and thus depression. However, there are also social implications of medical illness that are important; for example, a fall in the elderly can lead to fear of falling, thus reduced physical activity, increased isolation and depressive symptoms.
There are also certain conditions that put patients at particular risk. There is a high rate of depression in people with cerebrovascular disease, with 20–25% of patients having a major depressive disorder. This probably results from increased vulnerability secondary to structural brain damage as discussed above and also the potential loss of physical function, dependence on carers and loss of social activity. Other specific conditions associated with increased prevalence of depression are
PD
Alzheimer's disease
Cardiovascular disease
Hypo- and hyperthyroidism
Diabetes
Finally, certain medications have also been linked to an increased risk of depression
beta blockers
central nervous system medications
calcium channel blockers
digoxin
corticosteroids
anti-Parkinsonian medications
benzodiazepines
Insomnia
There is an important relationship between insomnia and depression, and this becomes even more relevant in this age group, with a high prevalence of insomnia and other sleep disorders in the elderly. It is well known that sleep disturbance is a common symptom of depression; however, it has also been shown that insomnia often precedes the onset of the mood disorder. Furthermore, the presence of insomnia in depression is a poor prognostic factor, and the continuing presence of insomnia in remission is a risk factor for earlier relapse.
Personality
Several personality traits have been associated with an increased risk of depression, and these are similar across age groups
Neuroticism (predictive for developing first onset late-life depression)
Anxiety
Pessimism (predictive of suicidal thoughts)
Rumination
Avoidance
Narcissistic personality traits (associated with increased suicide risk)
Apathy
Conversely, personality traits such as resilience are protective against the risk of depression in the presence of stressful life events.
Genetic
It is possible that there may be a genetic preponderance to developing late-life depression, although a family history of mood disorder is more common in patients developing depression at a younger age, and no definite genetic markers have yet been identified. Genetic preponderance that predisposes to conditions mentioned above, such as vascular disease and Alzheimer's disease, is more likely to be significant.
Previous history
Recurrence of depressive episodes is common, and thus a previous episode of depression earlier in life is a strong risk factor when elderly. Furthermore, some research has shown that childhood trauma remains a risk factor for depression in later life.
Clinical features
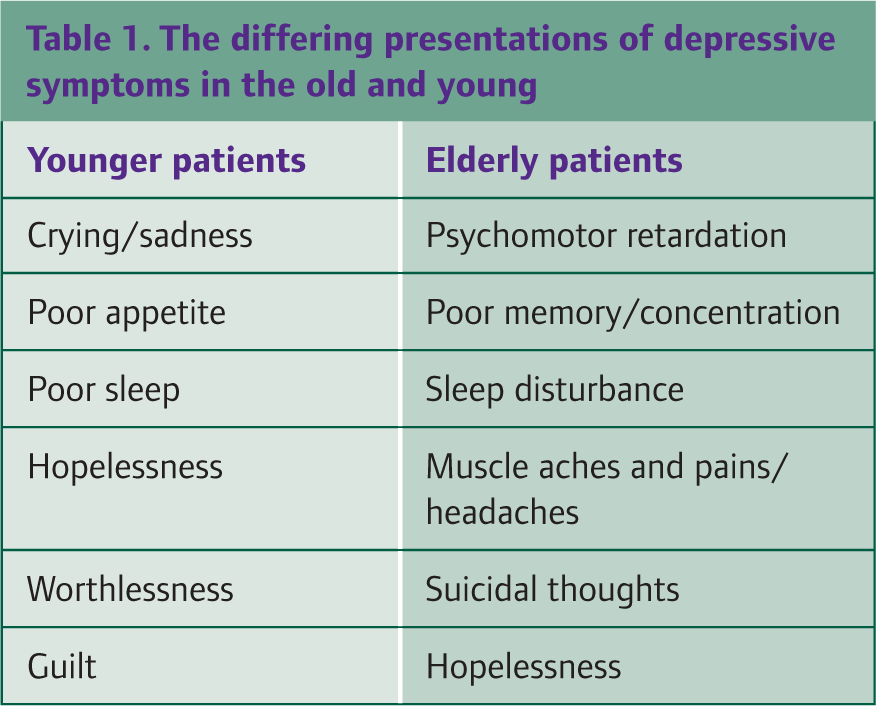
The symptoms of depression and criteria for diagnosis as defined by ICD-10 can be seen in Box 1. Detection of depression in the elderly can be difficult for various reasons. Older patients are more likely to underreport symptoms, and therefore, collateral history from family members and carers is particularly important. Late-life depression also tends to present with symptoms more suggestive of cognitive impairment and somatic symptoms than affective changes (Table 1).
The differing presentations of depressive symptoms in the old and young
Assessment and diagnosis
When elderly patients present with possible symptoms of depression, it is important that other medical causes for their symptoms are excluded through a thorough history, examination and appropriate investigations (Box 2). This should include exclusion of
Endocrine abnormalities, e.g. thyroid abnormalities and diabetes
Drug toxicity
Substance misuse, e.g. alcohol
Nutritional deficiencies, e.g. vitamin B12 deficiency and anaemia
Sleep disorders, e.g. insomnia
Infectious disorders, e.g. encephalitis or human immunodeficiency virus infection
Neoplastic disease
Neurological disorders, e.g. cardiovascular disease or dementia
Investigations to consider in an elderly person with depressive symptoms
Full blood count
Urea and electrolytes
Calcium and albumin level
Thyroid function tests
Fasting glucose
B12/folate
Urinalysis
Electrocardiogram (ECG)
Computed tomography (CT) scan of the brain (in many areas only available via secondary care)
Diagnosis can be aided by the use of verified scoring systems, such as the Patient Health Questionnaire (PHQ-9; Box 3). This is a screening tool that can be used within a GP consultation to gauge the presence and severity of depression. It can also be used to monitor the success of treatment.
A mental state examination should be done to assess, for example, the presence of psychotic symptoms or thoughts of self-harm or suicide. In the elderly, this should include a mini-mental state examination (MMSE) to screen for cognitive disorders.
Questions of the nine-point PHQ-9
Over the last 2 weeks, how often have you been bothered by any of the following problems?
Little interest or pleasure in doing things?
Feeling down, depressed or hopeless?
Trouble falling or staying asleep or sleeping too much?
Feeling tired or having little energy?
Poor appetite or overeating?
Feeling bad about yourself—or that you are a failure or have let yourself or your family down?
Trouble concentrating on things, such as reading the newspaper or watching television?
Moving or speaking so slowly that other people could have noticed? Or the opposite—being so fidgety or restless that you have been moving around a lot more than usual?
Thoughts that you would be better off dead or of hurting yourself in some way?
0 = not at all
1 = several days
2 = more than half the days
3 = nearly every day
0–4 = no depression
5–9 = mild depression
10–14 = moderate depression
14–19 = moderately severe depression
20–27 = severe depression.
PHQ © 1999 Pfizer Inc. All rights reserved
Consequences of depression in later life
Depression has wide ranging consequences for the individual and society. Older people with depression have higher morbidity rates than non-depressed counterparts and a mortality rate two to three times higher than expected. They are also more likely to be dependent on carers, and there is a higher rate of nursing or residential home placement. This in turn has wider implications for the family of the patient and economic implications for health and social services.
Suicide risk
Suicidality is an important issue in the elderly. Compared with younger adults, they are more likely to die as a result of a suicide attempt. It has been estimated that 7% of elderly primary care patients suffer with suicidal thoughts and prevalence increases with age. Suicide is much more common in men. The greatest risk factor for suicidal ideation is depression, and thus, careful assessment and intervention for patients with depression is vital.
Management
The National Service Framework for Older People (Department of Health, 2001) identifies three important aspects to the management of depression in the elderly
Promoting good mental health
Early recognition and management of mental health problems
Access to specialist care
Promoting good mental health
The promotion of good mental health is an important role for the GP as GPs are well placed to screen for social and physical risk factors and act to modify them. The holistic treatment of chronic medical illnesses and the modification of risk factors for vascular disease are also important. Moreover, services that seek to reduce social isolation and bereavement services are particularly useful in this age group.
Early recognition and management of mental health problems
National Institute for Health and Clinical Excellence NICE (CG90, 2009), recommends a ‘stepped-care’ approach to management of depression (Fig. 2). It highlights the important role that the GP has in the recognition of depression in patients, being active in screening ‘at-risk’ groups such as the bereaved or those with a chronic illness. NICE recommends the use of screening questions:
During the last month, have you often been bothered by feeling down, depressed or hopeless?
During the last month, have you often been bothered by having little interest or pleasure in doing things?

Stepwise management of depression.
A positive response to either of these questions should prompt further assessment, for example, with an assessment tool, such as the PHQ-9. Once a depressive illness has been identified, the GP should involve other members of the multidisciplinary team, such as primary mental health care workers and specialist care as appropriate, and initiate treatment.
Expert consensus guidelines have been published in the UK by Baldwin et al. (2003) and in the USA by Alexopoulos et al. (2001), which can aid in the decision of initiating treatment for different types of depressive illness, specifically in elderly patients. Table 2 summarizes their guidance. This is similar to the NICE guidance for all age groups (Fig. 2), but specifies that a patient with a more prolonged mild depression or dysthymia should be considered for antidepressant medication.
A summary of the expert consensus guidelines for the treatment of late-life depression

Antidepressant medication
The pharmacological options for treating depression in the elderly involve the four classes of antidepressant medication: the SSRIs, the tricyclic antidepressants (TCAs), the monoamine oxidase inhibitors (MAOIs) and the newer noradrenaline and serotonin reuptake inhibitors (Table 3).
A summary of the antidepressant medications available

The commonly used classes of medications in primary care are the SSRIs and TCAs. Evidence-based practice is difficult in the elderly, especially the above 75 age group, as they are often excluded from randomized controlled trials. However, a recent Cochrane review ‘Antidepressants for the elderly’ (2006) found no significant differences in efficacy between SSRIs and TCAs, and thus, the choice of treatment must be based on the individual patient's circumstances, taking into account the following factors:
Response to previous treatment
Co-morbidities
Other medications and interactions
Side-effect profile
Risk of suicide
Desirability of other effects of drug, e.g. sedation
Patient choice
For example, if there is a risk of suicide, SSRIs are a safer choice of treatment as they are generally not toxic in overdose. In the presence of sleep disorder, a sedative antidepressant such as a TCA may be appropriate.
All the classes of antidepressants can have significant side effects (Table 4), although the Cochrane review found SSRIs are generally safer and better tolerated, and for this reason are generally the first-line treatment in the elderly. The NICE guidance (CG23, 2007) recommends close observation of patients on antidepressants for side effects.
The common side effects of antidepressants

SSRIs most commonly cause gastro-intestinal side effects, with other side effects being agitation, gastro-intestinal bleeding and hyponatraemia. There is an increased risk of hyponatraemia in the elderly, women, those concomitantly taking diuretics and those with lower body weights. Hyponatraemia can lead to increased confusion and fatigue. It is therefore important that serum sodium concentrations are monitored regularly.
As well as urinary retention, dry mouth and blurred vision, TCAs can cause confusion and delirium in the elderly, and are more sedating than SSRIs. They can also cause cardiovascular side effects and arrhythmias and should be avoided if possible in those with ischaemic heart disease.
The MAOIs are generally used in secondary care since they have significant drug and food interactions and are most effective in atypical depression. Newer drugs (such as venlafaxine or mirtazapine) have not been shown to be more effective than the SSRIs but may be a useful second-line option when other medications are not tolerated or there is an insufficient clinical response to SSRIs or TCAs.
In the elderly, the dose should be started low and slowly increased to a therapeutic dose. Treatment should be for at least 6 weeks at therapeutic level before assessment for response. If there is no improvement in mood by then, the drug is unlikely to have any effect. It is important that primary care practitioners understand that treatment in the elderly may take longer to become effective, and elderly people may need longer courses of antidepressants or ‘prophylaxis’ when well. A consensus guideline (Baldwin et al., 2003) recommends continuing treatment for at least 12 months after achieving remission of symptoms, while NICE guidance (CG90, 2009) recommends continuing antidepressants when well in older patients who have experienced multiple depressive episodes in order to prevent relapse.
Psychological therapies
There are three psychological therapies that have been recommended in the National Service Framework for Older People
Cognitive behavioural therapy (CBT) is of use in the depressed elderly. This is a technique that can help patients understand and modify how their thoughts affect their feelings and then behaviour and can particularly help with feelings of hopelessness, suicidality, low self-esteem and poor problem solving.
Interpersonal therapy (IPT) looks at improving interpersonal skills and roles, understanding that these factors are important in psychological well being. This therapy looks at areas such as grief and role transition (where patients are giving up old roles and taking up new ones) and helping them work through difficult emotions and acquiring social skills and support in their situation.
Cognitive analytical therapy is a brief focused therapy that looks at changing maladaptive coping procedures to problems experienced in life.
Problem-solving therapy is also commonly used for elderly patients. This is a focused therapy that looks to teach problem-solving skills to help patients overcome stressful events and problems within the context of their social setting.
Focal brain stimulation
In the past, this area of treatment has been limited to electroconvulsive therapy (ECT), a very effective therapy in treatment-resistant depression but one with cardiovascular and cognitive side effects. More recently, newer techniques have been introduced such as deep brain stimulation and transcranial magnetic stimulation to areas of the prefrontal cortex and subgenual cingulate (see Fig. 1) and have had encouraging results in patients with treatment-resistant depression.
Indications for referral to specialist care
Indications for referral to specialist care include
Uncertain diagnosis
Insufficient response to treatment
Suicide risk
Complex patients with multiple co-morbidities
Psychotic depression
Specific groups
Depression and cognitive impairment
It can be difficult to differentiate between depression and cognitive impairment as they can both coexist with each other and mimic each other. Ageing-related processes, such as cerebral atrophy and vascular disease, that disrupt structures and pathways can affect both mood and executive function, and this may explain some of the relationship between these presentations.
Some patients with depression will present with symptoms of cognitive impairment (‘pseudodementia’). This can improve with treatment of the mood disorder, although, in most, it will not completely resolve. Conversely, patients can appear depressed and withdrawn when in fact they are displaying apathy, a feature of dementia. Here, patients will not initiate activity but will join in when activity is introduced by another and their mood will be reactive to this stimulus.
There is also some debate as to whether depression is a risk factor for developing dementia or even a prodromal phase of the disease. Depression symptoms are highly prevalent in dementia, with 17% of patients having criteria for a major depressive disorder. However, it can be hard to diagnose depression in patients with dementia as patients find it difficult to communicate their symptoms. Tools, such as the PHQ-9 or the Geriatric Depression Scale, can be used reliably for patients with an MMSE of greater than 15, but below 15 the specificity for diagnosing depression becomes unacceptable. There are tools that have been validated in diagnosing depression in this situation, with The Cornell scale for depression in dementia (CSDD) being the most commonly used (Fig. 3).
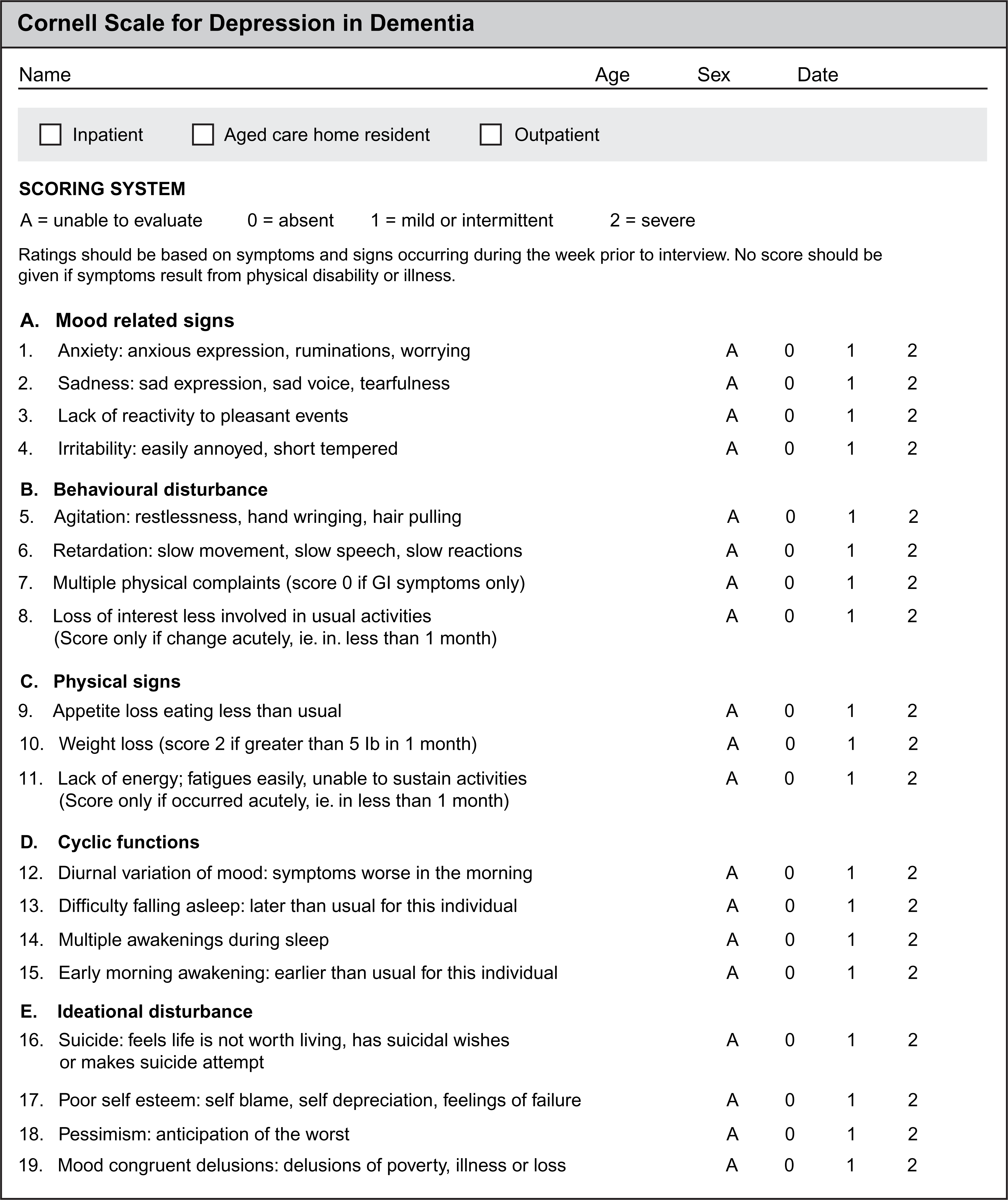
The Cornell scale for depression in dementia. Scores are determined by a combination of prior observation and two interviews: 20 minutes with the carer and 10 minutes with the patient. Depressive symptoms are suggested by a total score of eight or more.
If a patient has mild depressive symptoms in the presence of dementia, the guidance is to have a period of watchful waiting with simple psychosocial measures and caregiver support for a few weeks as there is a high rate of resolution of symptoms within 4 weeks. Examples of such support would be the introduction of pleasant activities and routine and education for the caregiver on depression, dementia and problem-solving skills. For more persistent or severe symptoms, treatment with SSRIs, TCAs and moclobemide (an MAOI) have all been shown to be effective. The SSRIs sertraline or citalopram are generally the first-line agents. TCAs have been found to have more anticholinergic side effects in patients with dementia.
Post-stroke depression
As discussed previously, depression is extremely common post-stroke and can present after days to months after the cerebrovascular accident, with a peak at 3–6 months. This has important consequences not only on quality of life but also on physical recovery post-stroke. It is so common that prophylactic prescription of antidepressants or the introduction of a psychological intervention such as problem-solving therapy has been recommended for these patients.
Depression in PD
It is estimated that one in three patients with PD will have some type of depressive disorder during their illness. Again, it is thought that damage to limbic system pathways in the PD process can predispose to depression. Diagnosis can be difficult as patients with PD tend to be emotionally labile and melancholic, but features that suggest depression in these patients are dysphoria, pessimism, irritability, sadness and suicidal ideation. Depression in PD is amenable to treatment with dopamine but also responds to SSRIs, TCAs and noradrenaline and serotonin reuptake inhibitors. TCAs may help with motor symptoms given their anticholingeric properties but tend to worsen cognitive impairment.
Key points
Depression is very common in the elderly and often underdiagnosed and undertreated
The aetiology is complex and made up of biological, psychological and social factors
Prevention and screening (e.g. using PHQ-9) in high-risk groups should be an important target
Treatment should include psychological and pharmacological interventions
There is no proven increased benefit of any class of antidepressant, but SSRIs are generally thought to be first line as they are the safest and best tolerated