
Abstract
Infectious hepatitis is a systemic infection predominantly affecting the liver. Most cases resolve spontaneously, but some progress to chronic hepatitis. Infectious hepatitis has a number of causes but this article will focus on hepatitis A, B and C. Diagnosis is made using liver function tests and serological tests to identify the virus. Depending on the specific virus, treatment and vaccination can be offered to patients and close contacts.
The GP curriculum and infectious hepatitis
A GP should
Be able to appropriately assess patients who present with jaundice and arrange investigations. Liver function tests (LFTs) form a key part of this process and hence knowledge of their interpretation is required (
Have knowledge of hepatitis B tests and their interpretation (
Have knowledge regarding immunization of patients at high risk of hepatitis B as well as immunization of children whose mothers are affected by hepatitis B (
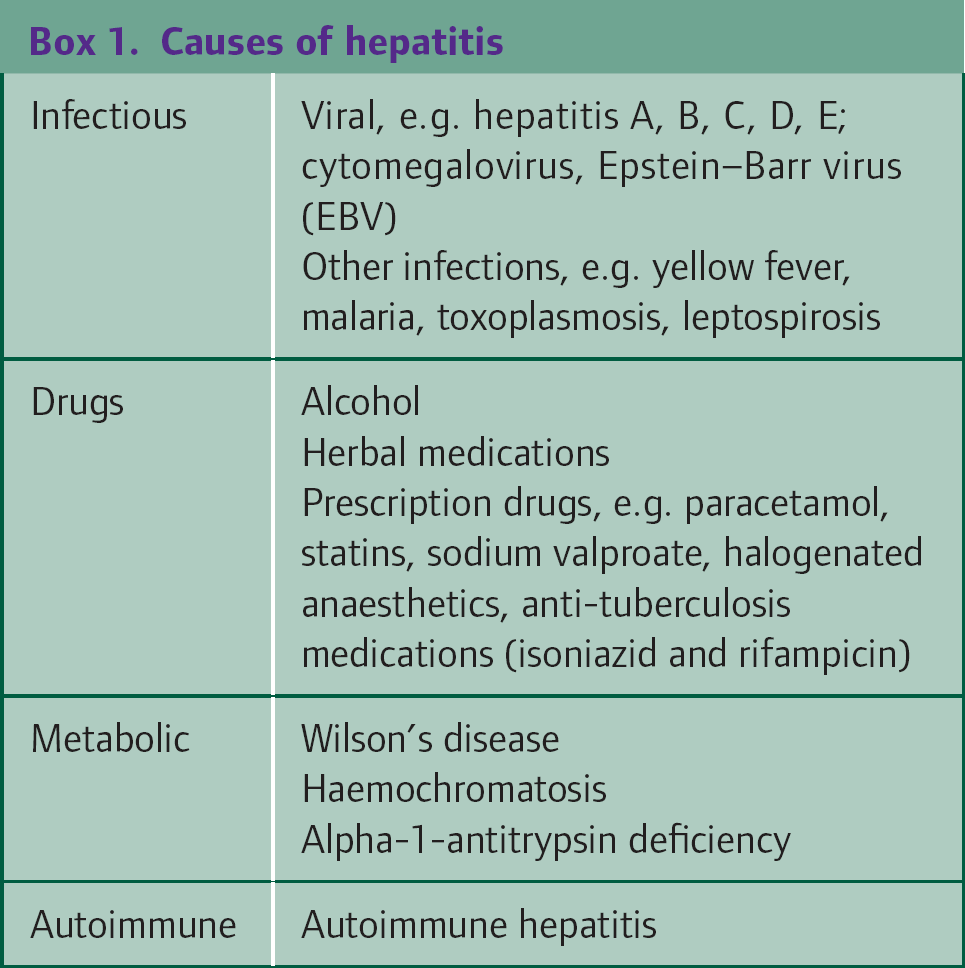
Inflammation of the liver, or hepatitis, may be caused by infection, drugs, alcohol, autoimmunity and genetic factors (Box 1). Patients with infectious hepatitis may present with acute hepatitis, chronic hepatitis, chronic liver disease or occasionally acute liver failure. A significant majority of those with chronic hepatitis are asymptomatic, and therefore it is important to have a higher index of suspicion in high-risk patient groups. These high-risk groups include
intravenous drug users sex workers patients who have had blood transfusions pre-1990 haemophiliacs men who have sex with men patients on haemodialysis tattoo recipients human immunodeficiency virus (HIV)-positive patients
Presentation
Acute hepatitis
Patients with acute hepatitis often present with non-specific symptoms of fever, fatigue, abdominal pain, loss of appetite, nausea, arthralgia and occasionally diarrhoea. Examination findings can include jaundice, painful hepatosplenomegaly and lymphadenopathy. Rarely patients may present with, or develop, sudden onset of severe illness indicating acute liver failure, sometimes accompanied by encephalopathy.
Causes of hepatitis
Chronic hepatitis
The majority of patients with chronic hepatitis are asymptomatic, but some may exhibit signs of chronic liver disease (Fig. 1). Occasionally, patients may present with decompensation of chronic liver disease and encephalopathy.
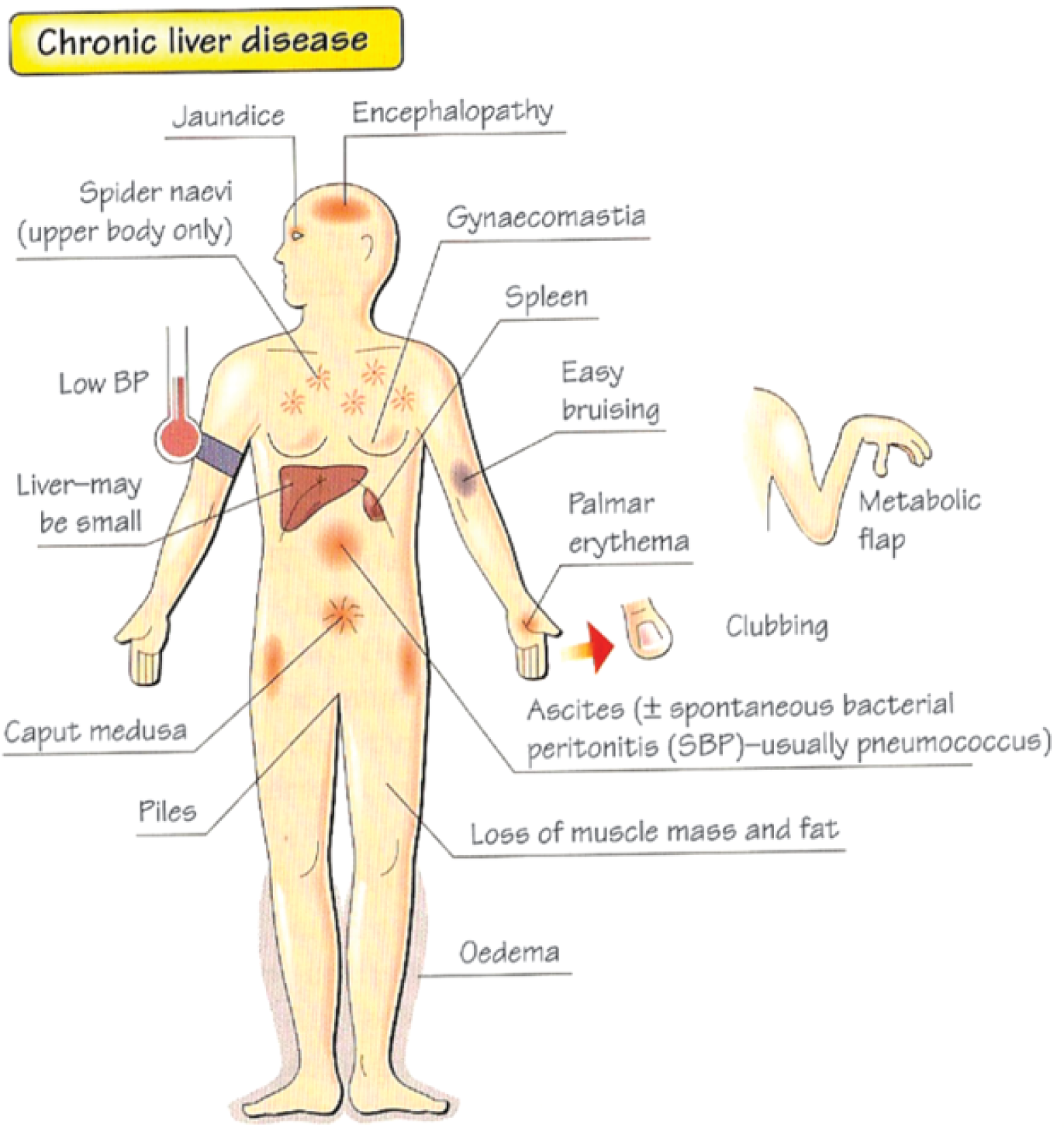
Signs of chronic liver disease
Asymptomatic patients with chronic hepatitis are diagnosed through screening of high-risk individuals, or coincidentally when mildly deranged LFTs are detected on routine blood tests and require further investigation. In any patient with deranged LFTs, consider the full differential diagnosis (Box 1). A thorough history (Box 2) and examination are often helpful in revealing the cause.
Important points to elicit in the history of a patient with deranged LFTs
Hepatitis A—foreign travel and jaundiced contacts Hepatitis B and C—sexual activity, intravenous drug use, blood transfusions, tattoos, body piercings and jaundiced contacts Drugs—paracetamol, herbal medications, antibiotics, oral contraceptives, other prescribed medications—previous and current Alcohol Family history—autoimmune hepatitis, Wilson's disease, haemochromatosis, alpha 1-antitrypsin deficiency
Investigation and referral
If a patient has symptoms or signs of infective hepatitis, is in a high-risk group and/or has a history of contact with a patient with hepatitis A, B or C, ask for viral hepatitis serology (along with LFTs) on symptomatic presentation or as soon as abnormal liver function is noticed. A previous InnovAiT article (Pritchett, 2009) provides a useful strategy for the investigation and management of abnormal LFTs in primary care. In summary:
Patients with acute or decompensated chronic liver failure with or without encephalopathy require immediate admission for inpatient treatment If a patient has very markedly raised or rapidly rising LFTs, urgent referral to secondary care may be appropriate without any further primary care investigations For patients with more minor elevations in LFTs, particularly if asymptomatic, it may be more appropriate to repeat the tests and investigate further in primary care
Patients with infective hepatitis have raised serum alanine transaminase (ALT) and aspartate transaminase (AST) compared to alkaline phosphatase. Bilirubin levels may be normal or elevated.
Further investigation in primary care
When assessing an asymptomatic patient with raised serum transaminases in primary care, consider other causes as well as infective hepatitis including:
Alcohol Non-alcoholic fatty liver disease Neoplastic disease Drugs
If a patient is clinically well but has transaminase levels in excess of three times the upper limit of normal, recheck LFTs in a week to ensure no rapid rises requiring secondary care referral. If the patient is clinically well and transaminase levels are less than three times the upper limit of normal, recheck them in 1–3 months. If the transaminases remain elevated, arrange for a liver ultrasound and perform a ‘hepatitis screen’, including the tests listed in Box 3.
Hepatitis screen tests
Serology for hepatitis A, B, C, EBV and cytomegalovirus Liver autoantibodies Iron studies/transferring saturation—for haemochromatosis Copper/caeruloplasmin—for Wilson's disease Alpha 1-antitrypsin level Alpha-fetoprotein—for hepatocellular carcinoma Fasting lipids, glucose and HbA1c
Refer for specialist assessment and management if
The diagnosis remains unclear and the LFTs remain elevated A diagnosis of hepatitis B or C is made If any other serious underlying cause of deranged liver function is found
Other infective viral hepatitides can usually be managed in primary care as they are self-limiting.
General measures
In patients with hepatitis or impaired liver function, all medications including contraception should be reviewed. Discontinue those drugs likely to adversely affect liver function until the patient has fully recovered, or if essential prescribe them in reduced dosage. Advise patients to refrain from drinking alcohol.
Hepatitis A
Hepatitis A is caused by the hepatitis A virus (HAV) that is transmitted faeco-orally through jaundiced contacts or travel to an endemic area. It has an incubation period of 2–6 weeks and is usually a self-limiting illness. Around 1000 cases of hepatitis A are notified per year in England and Wales but infection rates are probably much higher than this figure implies as patients may be asymptomatic (particularly children) or have mild symptoms only. The risk of acute liver failure is very low (less than 0.1%) although this increases with age and in those with pre-existing liver disease. There is no chronic infection state and recovery from an acute infection induces lifelong immunity.
Diagnosis of hepatitis A
The diagnosis of acute hepatitis A infection can be made in general practice by testing blood for anti-HAV immunoglobulin M (IgM). The presence of anti-HAV IgG indicates a previous infection and is detectable lifelong.
Management of hepatitis A
Hepatitis A is a notifiable disease and all cases should be notified to the local public health department so that contact tracing can occur. Payment is made to GPs for doing this.
Except in severe cases when a patient develops acute liver failure, the management of hepatitis A is supportive with rest and hydration. Patients with a higher risk of complications (those with concurrent hepatitis B or C, chronic liver disease or who are immunocompromised or aged over 50 years) may benefit from human immunoglobulin treatment under specialist supervision in secondary care. Seek specialist advice.
In all patients with hepatitis A, discontinue alcohol and medications such as oral contraception and hormone replacement therapy until the patient recovers from the acute illness. Advise patients to avoid food handling and sexual contact until they are non-infectious.
Follow up in general practice with repeat LFTs to ensure reducing transaminase and bilirubin levels, until they are normal (1–3 months). If at any point the patient develops signs of acute liver failure or has rapidly rising LFTs, admit for inpatient treatment.
Prevention of hepatitis A
The hepatitis A vaccine may be offered to close contacts of patients with hepatitis A such as sexual partners and household contacts. The vaccine may be given up to 14 days after exposure, providing that this exposure was within the infectious period of the source case (i.e. the prodromal period and first week of jaundice).
Hepatitis A vaccination should also be offered to susceptible individuals and patients at high risk of complications:
Travellers to endemic areas (Indian subcontinent, Far East and Eastern Europe) Individuals at occupational risk Haemophiliacs Patients with hepatitis B, hepatitis C or liver cirrhosis of any cause Injecting drug users
Hepatitis A vaccine is available as a monovalent vaccine, combined with hepatitis B vaccine or combined with typhoid vaccine. For patients travelling to endemic areas, good hand hygiene is particularly important in preventing hepatitis A.
Hepatitis B
Hepatitis B is caused by the hepatitis B virus (HBV) that is found in most bodily fluids of affected individuals. It is transmitted through sexual contact, parenterally (sharing needles by intravenous drug users or non-sterile instruments) or vertically (mother-to-baby at birth). The incubation period of HBV is 28–160 days. Most individuals who contract hepatitis B fully recover (95%). However, 2–5% develop chronic hepatitis with a smaller number developing acute liver failure or an inactive carrier state.
Some patients with hepatitis B develop symptoms and signs of acute hepatitis, but the majority present to primary care with chronic hepatitis. They are usually asymptomatic but may have symptoms and signs of chronic liver disease.
Diagnosis of hepatitis B
The diagnosis of hepatitis B is made by blood tests for the antigens and antibodies summarized in Box 4. The simplest initial screening test is anti-hepatitis B core (anti-HBc) antibody with the addition of other tests as necessary (Fig. 2).
Interpretation of hepatitis B serological tests
Appears at the onset of symptoms in acute hepatitis B and persists for life. The presence of anti-HBc indicates previous or ongoing infection with HBV.
A protein on the surface of HBV; it can be detected in high levels in serum during acute or chronic HBV infection. The presence of HBsAg indicates that the person is infectious. The body normally produces antibodies to HBsAg as part of the normal immune response to infection.
The presence of anti-HBs is generally interpreted as indicating recovery and immunity from HBV infection. Anti-HBs also develops in a person who has been successfully vaccinated against hepatitis B.
Positivity indicates recent acute infection with HBV (less than 6 months)

Flow chart for hepatitis B serology
Management of hepatitis B
Refer all HBsAg-positive patients with acute or chronic hepatitis to a hepatologist for further management. Hepatitis B is a notifiable disease and all confirmed cases should be notified to the local public health department so that contact tracing can take place.
On diagnosis, advise patients to avoid unprotected sexual contact until they become non-infectious and their partners have been vaccinated. Give patients a detailed explanation of their condition with particular emphasis on the long-term implications and routes of transmission. It is also important to screen for other sexually transmitted infections, including hepatitis C and HIV.
An acute infection of hepatitis B usually resolves within 1–3 months and most patients (95%) develop long-term immunity to the virus. At 6 months following the acute infection, serology is repeated by the hepatologist to assess for chronic hepatitis, even if LFTs appear normal.
Patients with chronic hepatitis are at risk of developing liver cirrhosis and hepatocellular cancer. They should be regularly reviewed by a hepatologist and undergo active surveillance with liver ultrasonography on an ongoing basis. Antiviral treatment such as lamivudine, tenofovir or pegylated interferon may result in reduced long-term liver damage and decreased risk of liver cancer in patients who respond to treatment. All patients with chronic hepatitis B infection should also be offered vaccination against HAV due to the increased risk of complications with concurrent infections. They are also advised to decrease alcohol intake to reduce the rate of liver cirrhosis.
Prevention of hepatitis B
Advise all patients who are sexually active (or likely to become sexually active soon) about ‘safe sex’. Immunize people in high-risk groups for hepatitis B:
Injecting drug users Those with many sexual partners (including sex workers) Adopted children from high or intermediate risk countries Foster parents Close family contacts of a case or carrier Those receiving regular blood or blood products and their carers Those with chronic renal or liver disease Prison inmates Those at risk due to occupation, e.g. health care workers Staff and residents of residential accommodation for individuals with learning disability or cognitive impairment Those travelling to high- or intermediate risk areas Babies born to mothers who are chronic carriers of hepatitis B or have had acute hepatitis B in pregnancy (vaccinated at birth)
Immediate post-exposure vaccination is effective in preventing hepatitis B. Ideally vaccinate within 48 hours of exposure to the virus, but vaccination is effective in prevention of transmission for up to a week. In addition, give passive immunization with human immunoglobulin at the same time as hepatitis B vaccination to non-immune high-risk contacts of infected patients.
Immunization is not necessary for those who have markers for current (HBsAg) or past infection (anti-HB) but do not delay vaccination to obtain these results. Consider using a rapid vaccination regime, with immunization at 0, 7 and 21 days, and a booster after 12 months, for those who have been exposed to hepatitis B (including newborn babies of mothers with hepatitis B) and injecting drug misusers.
Regimes used for pre-exposure prophylaxis include vaccination at 0, 1 and 2 months, with a fourth dose at 12 months for those at continued risk, or vaccination at 0, 1 and 6 months. In total, 10–15% of adults vaccinated will not become immune even after three doses.
Patients with chronic hepatitis B infection should not donate semen, blood, milk or organs. It is also important to educate them about taking care not to infect others through contact with their bodily fluids, for example through use of needle exchange schemes for intravenous drug users or safe sexual practices.
Hepatitis C
Hepatitis C is caused by the hepatitis C virus (HCV). It is a blood-borne infection that has an incubation period of 14–60 days. Unlike other forms of viral hepatitis, HCV is more likely to become chronic, with approximately 75% of infected individuals developing chronic infection.
Most acute and chronic infections are asymptomatic, and given the high risk of chronic disease, it is important that GPs have a high index of suspicion. Consider screening asymptomatic individuals who are at increased risk of HCV infection including:
Intravenous drug users Haemophiliacs Patients on haemodialysis Patients who had blood transfusions pre-1990 People at risk due to their occupation e.g. health care workers Men who have sex with men Sex workers Tattoo recipients HIV-positive patients Those with chronic hepatitis B infection
The transmission of HCV occurs mainly via blood and therefore can also potentially occur through sexual contact. Perinatal transmission rate is around 5%, which is much lower than HBV and HIV rates. In the UK, the two major routes of transmission of HCV have been through the sharing of needles by injecting drug users and transfusion of infected blood products. Since 1991, blood has been screened for hepatitis C, largely eliminating blood products as a source of HCV infection.
Diagnosis of hepatitis C
The diagnosis of HCV infection is made using a blood test looking for antibodies to the virus (anti-HCV antibodies). Pretest counselling is important (Fig. 3). Anti-HCV antibodies indicate current or previous infection. It is important to check when the individual was exposed to the virus because it can take up to 3 months for antibodies to be produced. If the antibody test is negative and the last exposure risk occurred in the preceding 3 months, a repeat anti-HCV antibody test should be performed after an appropriate interval.

Flow chart for the diagnosis of hepatitis C infection.
Any positive test should be confirmed with a second sample and a test for HCV ribonucleic acid (HCV-RNA). HCV-RNA assesses whether there is current infection. If the HCV-RNA test is positive, this indicates ongoing infection, and the patient should be referred to a hepatologist for consideration of treatment. A positive antibody test but negative HCV-RNA test indicates a previously resolved infection but not immunity to further infection. Confirm the negative HCV-RNA result with a repeat test after 4–6 weeks. In all cases, discuss the results of the tests with the patient and explain their meaning and implications both to the patient and to the patient's family.
Management of hepatitis C
Hepatitis C is a notifiable disease and the local public health department should be informed of any patient who tests positive for hepatitis C. All patients with confirmed hepatitis C infection should be referred for specialist follow-up by a hepatologist.
Under specialist supervision, patients with acute infection receive monitoring for the initial 3 months following diagnosis as they often have a self-limiting illness. Risk of acute liver failure in acute HCV infection is less than 1%.
If the infection does not resolve spontaneously, treatment with interferon begins 3–6 months after the diagnosis of acute hepatitis C. This reduces the risk of progression to chronic infection. Unfortunately, most acute infections are asymptomatic so the opportunity to treat is rare, unless known exposure to an infected contact has occurred.
Patients with chronic hepatitis C infection should be reviewed regularly by a hepatologist on an ongoing basis. They are at increased risk of developing cirrhosis and hepatocellular cancer and active surveillance with liver ultrasonography is carried out by the hepatology team. Education about the condition, its long-term prognosis and lifestyle implications is important. All patients with hepatitis C should be advised to reduce alcohol and tobacco intake to decrease the rate of progression of liver disease. Offer hepatitis A vaccination and screen (with consent and appropriate counselling) for other sexually transmitted infections, including HBV and HIV. Close contacts and family members should also be offered screening for HCV infection.
In patients with chronic infection, interferon and ribavirin are the only two available treatments. Under specialist supervision a decision on treatment is made based on HCV-RNA levels, HCV genotype and, in certain situations, a liver biopsy. When effective, treatment with antivirals reduces the risk of progression to cirrhosis and also the chance of hepatocellular cancer.
Prevention of hepatitis C
There is no vaccine available against hepatitis C. Therefore, prevention focuses on education. Inform patients with hepatitis C infection about routes of transmission and advise them to avoid activities that might expose others to their infected blood—for example, they should not share toothbrushes or razors. Patients with hepatitis C infection should not donate semen, blood, milk or organs.
Other viral hepatitides
Hepatitis D virus (HDV) is an incomplete RNA virus that requires the HBV outer coat for transmission and is therefore only found in patients with concurrent hepatitis B infection. The mode of transmission of HDV is the same as HBV, i.e. parenterally and through sexual contact. It is largely an infection affecting intravenous drug users and their sexual partners. It is associated with a high rate of chronic liver failure and progression of cirrhosis. If suspected, these patients should be referred to a hepatologist for specialist input.
Hepatitis E (HEV) is an RNA virus that is transmitted faeco-orally. It is a self-limiting illness and therefore treatment is supportive. Pregnant women are a high-risk category with a 15% risk of acute liver failure, and therefore require inpatient investigations and treatment if suspected.
The Epstein-Barr virus causes an acute febrile illness known as infectious mononucleosis (glandular fever), which occurs worldwide in adolescents and young adults. It is transmitted in saliva and by aerosol droplets. The predominant symptoms are fever, headache, malaise and sore throat. On examination, posterior cervical lymphadenopathy and splenomegaly are characteristic. It commonly causes mild hepatitis and treatment is supportive. The diagnosis can be confirmed by a monospot test. Both toxoplasmosis and cytomegalovirus cause clinically similar illnesses and can be diagnosed by serology.
Approximately 10–15% of acute viral hepatitides cannot be typed. Therefore, depending on the clinical presentation, a ‘watch and wait’ approach while monitoring LFTs may be appropriate because the majority of these infections are self-limiting. However, if the patient has signs of acute liver failure or has rapidly rising LFTs, then urgent referral to secondary care is appropriate.
Pregnancy and breastfeeding
A small number of pregnant women have abnormal LFTs and jaundice in pregnancy. While this is relatively rare, it can have potentially serious consequences for maternal and foetal health. The important causes not including viral hepatitis are pre-eclampsia, acute fatty liver of pregnancy, hyperemesis gravidarum and intrahepatic cholestasis of pregnancy. Hence jaundice in pregnancy requires prompt referral to an obstetrician for further investigations and management.
Hepatitis A infection in pregnant women increases the risk of premature labour and miscarriage and requires specialist input. HAV-infected mothers can continue to breastfeed and most children will have mild or asymptomatic infection.
All pregnant women are currently offered screening for hepatitis B infection as part of routine antenatal care. Infants born to HBV-infected mothers are at high risk of vertical transmission and are therefore vaccinated at birth. HBV-infected mothers can continue to breastfeed as there is no additional risk of transmission.
At the present time, there is no known way of reducing vertical transmission in HCV-infected mothers. Women should be informed of the potential risk of transmission in pregnancy. There is no firm evidence of additional risk of transmission in breastfeeding women except perhaps those who are symptomatic with a high viral load.
Occupational exposure of primary care staff
Prevention of exposure to contaminated blood is an important part of health and safety policy in every GP practice. General measures include
Washing hands before and after contact with each patient Wearing gloves where contact with blood can be anticipated and changing gloves between patients Covering existing wounds, skin lesions and all breaks in exposed skin with waterproof dressings When using sharps taking particular care with handling and disposal—it is the responsibility of people using sharps to make sure that they are disposed of appropriately' Avoiding open footwear where sharp instruments or needles are handled or blood or other bodily fluids may be spilt Clearing up any spillage of bodily fluids promptly and disinfecting surfaces
Ensure that the practice has a policy in place for use in the event of exposure to potentially contaminated bodily fluids. Staff need to know how to report these incidents and a policy must be in place, including access to emergency occupational health advice, for management of all such incidents.
Immediate actions post-exposure
Immediately following any exposure, the site of exposure, for example the needle puncture wound or area of non-intact skin, should be washed liberally with soap and water but without scrubbing. Exposed mucous membranes, including eyes, should be irrigated copiously with water (removing contact lenses first if worn). If there has been a puncture wound, gently encourage free bleeding.
Obtain as much information as possible about the person who was the source of the exposure, including risk factors for blood-borne infection, results of previous tests for HIV or hepatitis and medical history suggestive of such infection. Then contact the responsible medical officer, the nearest public health laboratory, the local health protection unit or virologist on-call for advice on further management.
In primary care, depending on local arrangements, take a baseline sample of serum from the person exposed, and ask the source patient for permission to take a blood sample for testing for blood-borne infections, including HIV, HBV and HCV. Consent for testing should be obtained and appropriate pretesting counselling given.
Post-exposure prophylaxis
If the source patient is known to have hepatitis B infection, and the exposed individual has not been immunized, or if the person exposed is a known non-responder to hepatitis B vaccination and it is not known if the source patient has hepatitis B infection, refer for administration of hepatitis B immunoglobulin (usually to occupational health or accident and emergency depending on local arrangements). This is most effective within 48 hours of exposure and is of no use after 7 days.
In all cases, consider providing a course or a booster dose of hepatitis B vaccination. Choice depends on whether vaccination has been given previously and known antibody response to previous vaccination. Up to date recommendations are available from the Department of Health in the Green Book (www.dh.gov.uk/greenbook). Vaccination given within 7 days of exposure (and preferably within 48 hours) is an effective preventative measure. For those receiving immunoglobulin, vaccination can be given at the same time but at a different site.
At the present moment there is no post-exposure prophylaxis available for hepatitis C. If a member of practice staff is contaminated with blood from a known HCV source, closely monitor for acute hepatitis C infection requiring referral to secondary care. If the individual develops acute hepatitis, this can be treated with antivirals under specialist supervision but there is the potential to develop chronic infection. Health care workers who know that they are HCV-RNA positive should not perform exposure-prone procedures.
Follow-up
Exposed individuals will require follow-up serological testing to ensure that they have not been infected with hepatitis B or C or HIV. This is best done through an occupational health department. While testing earlier might be appropriate in some cases, testing 6 months after the exposure will usually exclude the possibility of transmission of these infections.
Exposure of a member of staff to possible blood-borne infection is a significant event. All such events should be formally discussed so that measures can be put in place to avoid further incidents.
RIDDOR (Reporting of Injuries, Diseases and Dangerous Occurrences Regulations) should be notified about any staff member contracting hepatitis B or C (www.hse.gov.uk/riddor). Industrial Injuries Disablement Benefit can be paid where an employed person contracts viral hepatitis, as long as the person has worked in an environment where exposure to human blood or blood products could occur. In addition, the NHS Injury Benefits Scheme provides temporary or permanent benefits for all NHS employees (including those employed in primary care) who lose remuneration because of an injury or disease attributable to their NHS employment.
Key points
Infectious hepatitis can present acutely with symptoms but can also affect individuals asymptomatically Hepatitis A is generally a self-limiting illness. Vaccination against HAV is important in susceptible individuals and patients at high risk of complications. Hepatitis B resolves in 95% of individuals with a small percentage going on to develop chronic infection. Vaccination of high-risk groups such as health care workers is important. All pregnant women are offered HBV screening. Hepatitis C is most likely to present asymptomatically with chronic infection. Screening of patients at high risk of contracting hepatitis C is important. Hepatitis A, B and C are notifiable diseases