
Abstract

Assessment of risk is crucial to patient safety during times of crisis. As a GP registrar, I often find these situations quite daunting. I asked Dr Matt Rowett, ST4 in Psychiatry, for some advice.
Suicidal intent
How do we assess a patient who is suicidal in the community?
There are rating scales for the assessment of suicidal intent; however, these often focus on assessment following a suicide attempt. Formal rating scales also have the drawback of being awkward to use in a clinical encounter. We can, however, use our knowledge of the items on these scales to inform our enquiry into a patient's thoughts about suicide.
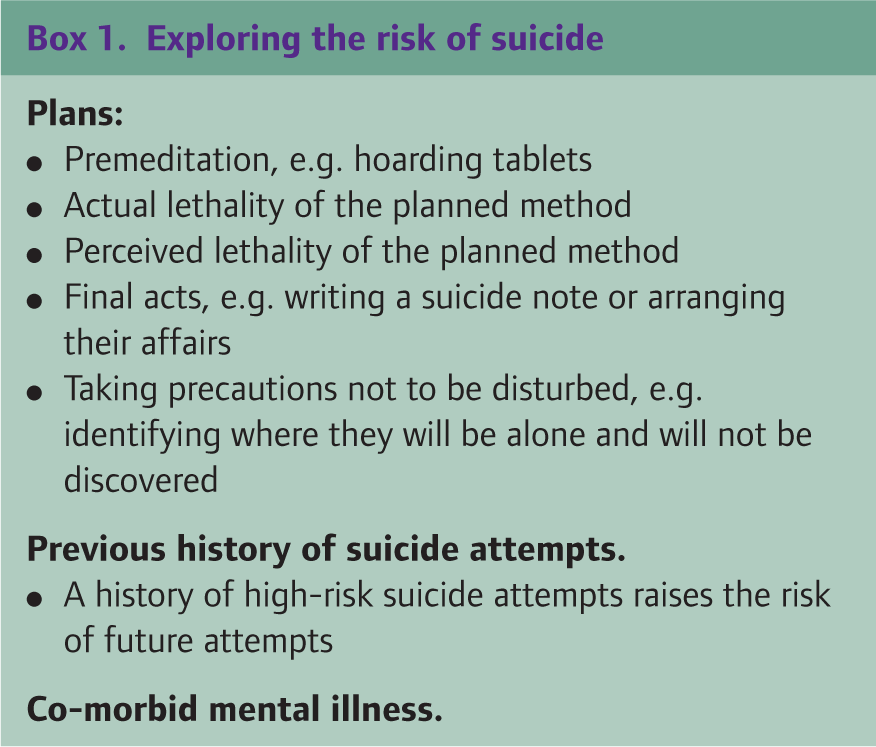
The most important question to ask if suicidal intent is suspected is whether the patient has thoughts of ending their life. It is surprising how often this simple question is omitted. If the answer to this question is ‘yes’ it does not necessarily mean there is a significant risk of suicide so more information is necessary. This can be broken down into the following areas as shown in Box 1.
Exploring the risk of suicide
Premeditation, e.g. hoarding tablets
Actual lethality of the planned method
Perceived lethality of the planned method
Final acts, e.g. writing a suicide note or arranging their affairs
Taking precautions not to be disturbed, e.g. identifying where they will be alone and will not be discovered
A history of high-risk suicide attempts raises the risk of future attempts
Personality difficulties
Patients with personality difficulties pose many challenges. They may inappropriately use services and can cause time management problems within consultations. How do you set boundaries and communicate the management plan?
Unfortunately, there is no simple answer to this question. Personality traits of impulsivity, unpredictability, tendency to outbursts of emotion and quarrelsome behaviour can lead to the doctor experiencing feelings of frustration in response to unreasonable behaviour.
It can help to understand some of the processes behind the patient's behaviour. Patients with emotionally unstable personality disorder often have a fear of abandonment and will go to excessive lengths to avoid being abandoned. This can include increasing the frequency or severity of problem behaviours to draw someone closer if they feel abandoned, e.g. if that person goes on holiday or cancels an appointment. They can idealize some people while demonising others. This leads to an unsustainable situation, as no matter how hard the idealized person tries they will eventually abandon the patient by doing something ‘wrong’, e.g. being unable to offer an appointment or intervention.
They can identify the doctor as taking the same role as someone from their past. For example, if the person was abused by someone in a position of authority, they may see all people they feel have authority over them as a threat. This can lead them to take a defensive and hostile approach before the doctor has even said a word.
Knowledge of the processes involved can allow us to understand our responses more and to maintain our boundaries as we are not drawn into taking the roles or meeting the expectations that are put upon us.
Communicating the management plan to a patient when you know your assessment differs from theirs can be difficult. It is important to listen to their point of view and empathize with their problems. Find a common ground by focusing on what you both agree on and use this to form a partnership. This might be as simple as acknowledging their distress and agreeing to respect each other's opinions. A practical tip for setting boundaries is highlighted in Box 2.
Practical tips
Writing down ‘contracts’ should be done with caution as it is hard to enforce consequences if they are broken, but you may be expected to adhere to the contract rigidly. Agreeing regular appointments at set times can cut down on repeated attendance and contain the anxieties of a chaotic patient; however, ‘extra measures’, such as appointments after hours, should be avoided as they are a sign that boundaries are moveable. All suggestions will come with a caveat but the overriding principle is to balance the anxiety and caring impulse some patients can evoke with consistent practice and boundaries
It is interesting to note that a diagnosis of personality disorder is associated with increased attendance at primary care. However, agreement between GP rating of personality disorder and that of standardized assessment has been shown to be poor. GPs reported personality disorder more frequently in patients who were perceived to be less compliant, less likeable and more stressful to deal with. Patients who were diagnosed with a personality disorder on a standardized rating scale did not attract these perceptions!
Footnotes
Acknowledgements
Danielle Peet is a GP trainee currently doing a hospital placement in a mental health unit in rural Northumberland. ‘I find dealing with emotionally unstable patients challenging and often exhausting. I try and look after myself by discussing tricky things with my trainer or with friends.’