
Abstract

This competence is about the management of the health and social care of the practice population and local community.
In the previous article on community orientation, we discussed the first competence progression about understanding the people who make up the local community. In this article we look at the second progression, shown in Fig. 1, which concerns the resources that are available to the local patient population.
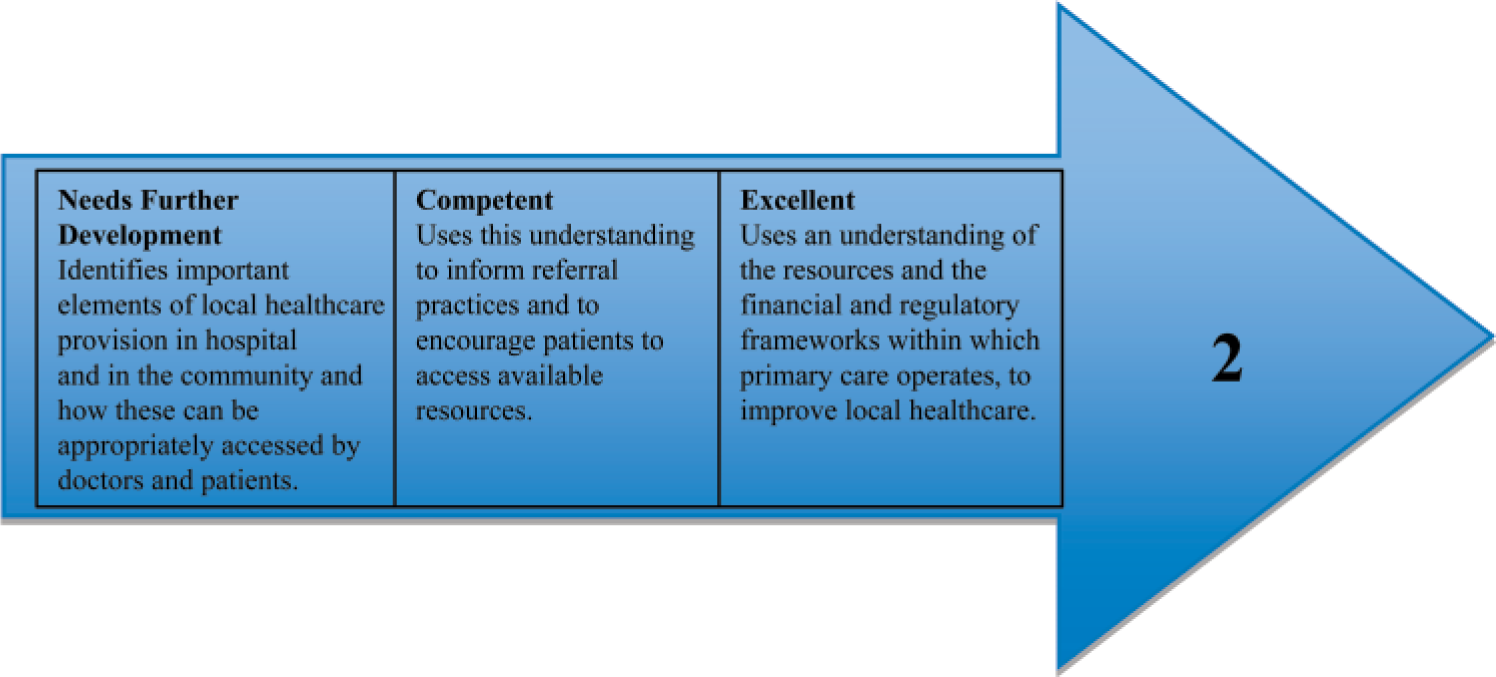
The second competence progression of community orientation.
Let us discuss the word pictures in turn.
This basic level is mainly about information gathering and there are two stages involved. Firstly, we need to find out what hospital and community services are available. There may be specialist hospitals such as oncology and children's hospitals as well as district general or teaching hospitals. In the community, there will be health visitors, district nurses, midwives and community mental health workers. Less commonly, there may be chiropodists and community physiotherapists. It is worth being aware of the roles and availability of paid carers, respite care and the services offered by local voluntary and statutory agencies.
In between community care and hospital care, there may be specialist outreach nurses such as diabetic and epilepsy liaison nurses, who can give specialist advice and support and can usually be contacted directly by sufferers.
Tip: knowing what is available
In order to do your job effectively, you will probably need to keep a diary or address book in which the important contact details are logged. You may also wish to add information on whether or not the patient can self-refer to these resources.
This list of contacts is good evidence of having achieved the first level.
You should already know the opening hours of your practice, including any extended hours that it offers. You will also need to find out how out-of-hours care is provided and how patients can access GPs and other providers of emergency care such as casualty departments, National Health Service (NHS) direct and walk-in centres.
Secondly, you need to find out for whom these services are available and how they can be accessed by doctors and possibly directly by the patient.
Assessors will look particularly closely at referral practices. Good referral practice partly means that the problem has been appropriately defined and that we have appropriately decided that it is beyond our sole management. However, it also means that the inquiry has been appropriately directed. ‘Encouraging patients to access available resources’ may mean advising them about a range of people and resources that are available.
Also, because GP care is holistic, we should think about the needs of the patient's family and carers as well as the patient. When it comes to resources, carers are frequently overlooked. Many self-help groups for patients with significant/chronic conditions are good sources of support for carers and can often signpost other useful resources that you may not be aware of.
When you have offered such help, which might include advising about websites or giving a patient information leaflet, it is worth recording this in the medical record. This will help others involved in the patient's care to see that wider forms of help have been offered and will also provide evidence of your competence in this area.
This descriptor of excellence shows how we apply knowledge of the healthcare system rather than just our biomedical knowledge to improve the health of a whole community. This depends upon knowing where the faults lie in the current service, the characteristics of the local population and what they need, what they expect (which may not be what they clinically need), what is feasible, allowable and what is cost-effective. As you can see, this is a complex calculation!
Tip: service redesign
Even if you are not yet able to demonstrate the ‘excellent’ competence, you can learn a great deal by joining in any service initiatives that your practice is part of. Ask the GPs and practice manager about the practice development plan/business plan. Identify an area of service improvement and speak to the lead clinician or manager in the practice. If you can, try to observe how the process is carried out, perhaps by sitting in at one of the relevant meetings.