
Abstract
Blisters are fluid-filled eruptions on the skin or mucous membranes. They are commonly seen in general practice in patients with herpes infection, insect bites, burns and friction trauma. Primary blistering disorders, for example bullous pemphigoid (BP) and pemphigus vulgaris (PV) are rare in comparison. These are immune or inherited disorders of proteins that bind the skin together. Blistering conditions may present alone or in association with other diseases, for example dermatitis herpetiformis and gluten-sensitive enteropathy. Blistering may be trivial or life threatening and therefore requires a logical approach to assessment, management and referral in the primary care setting.
The GP curriculum and blistering skin conditions
GP
Have a reasoned approach to the diagnosis of skin diseases using history, examination and investigations
Work in close collaboration with specialist dermatological services
Intervene early when the patient presents with an emergency skin problem
Know about drugs that may cause skin conditions and describe the side effects of drugs used to treat skin disease
Understand how cosmetic skin changes may affect the patient
Autoimmune bullous disease
The most widely known immunobullous diseases are BP and PV. The Latin bulla and Greek pemphix both mean ‘bubble’. The term pemphix was originally used to describe all blistering disease. BP and PV were separated as disease entities by Lever in 1953 and later characterized by the technique of immunofluorescence (IF) in 1967.
In both conditions, the body produces autoantibodies against desmosomal proteins important in stabilizing the skin epidermis. These diseases are typically seen in the elderly (Fig. 1). Other autoimmune diseases such as dermatitis herpetiformis and linear immunoglobulin (Ig) A disease are generally found in younger patients.
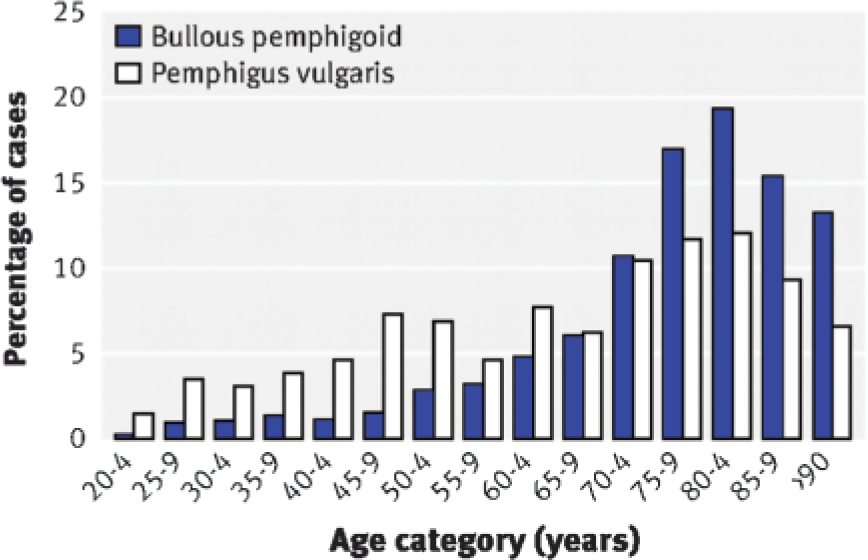
Age at diagnosis in patients with bullous pemphigoid and pemphigus vulgaris.
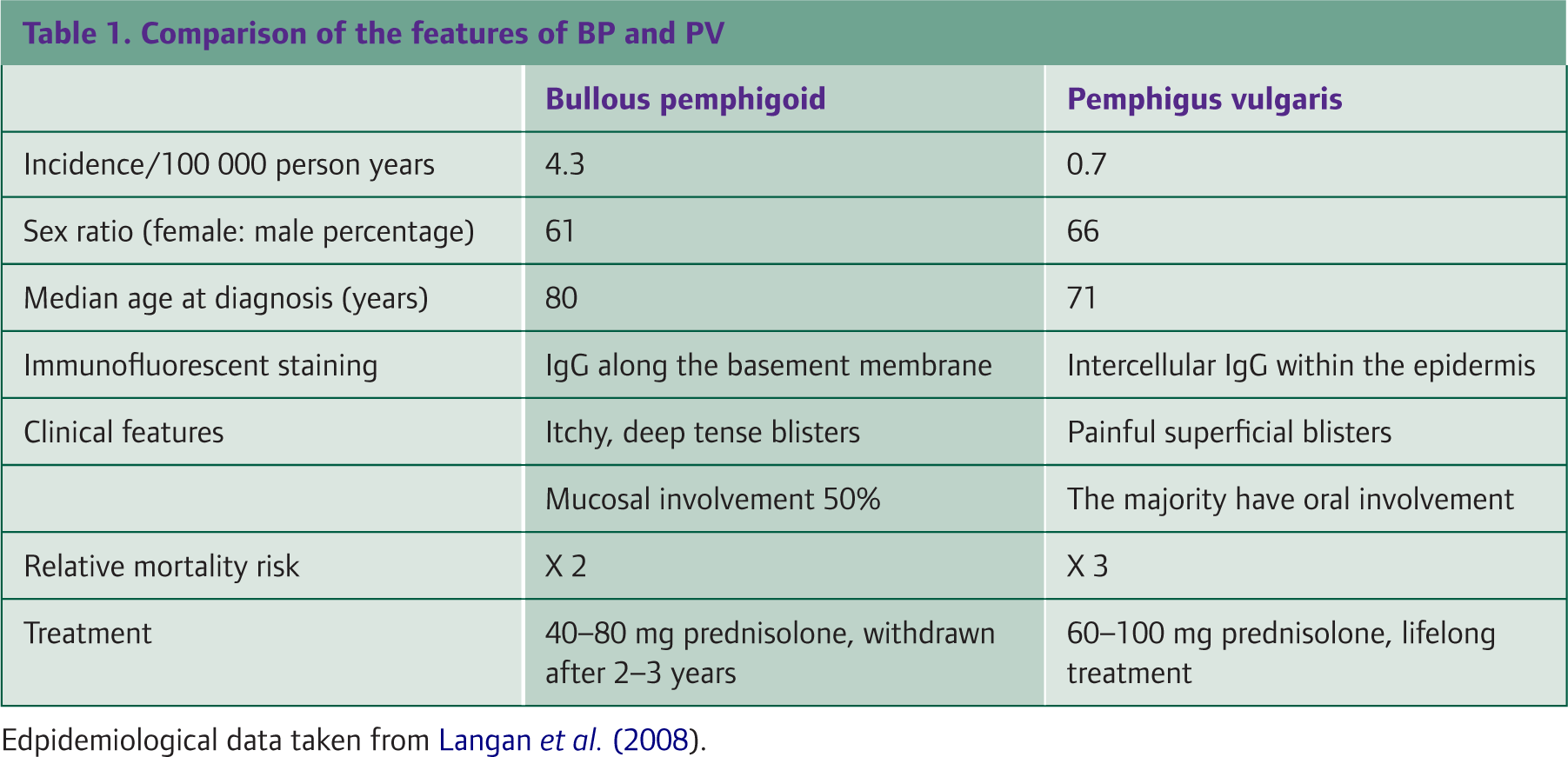
A recent UK-based primary care cohort study showed that the incidence of BP and PV is rising (Langan et al. 2008). The reason for this is unclear. In the same study, mortality from these conditions was also shown to be greater than previously estimated. The risk of death in BP and PV is 2-and 3-fold that of matched controls, respectively. Patients, especially the elderly, are at risk not only from the disease but also from complications of immune suppressing treatments. However, the steroid treatment risks must be balanced against the success of steroid therapy in controlling disease, for example in PV steroid treatment reduces mortality from 75% to 30%.
The severity of disease varies greatly depending on the condition that the patient has. Blisters may range from being localized and a nuisance to causing systemic illness and disfigurement. If you suspect autoimmune disease, refer to a dermatologist to confirm diagnosis and guide management.
In severe disease, investigations should wait until treatment is initiated. Diagnosis is made clinically, using histology (on perilesional biopsy) and IF. IF demonstrates the presence of antibodies bound either in the skin (direct IF) or in the serum (indirect IF) of the patient by showing specific green fluorescence under the microscope. In Fig. 2, this technique is demonstrated for linear IgA disease. Indirect IF requires incubation of the patient's serum with another substrate, for example monkey oesophagus.

Linear band of IgA at the dermoepidermal junction.
The goal of treatment is to make the disease tolerable to an individual patient. This includes reduction in blister formation, itch and sores. Steroids are the mainstay of treatment and work by reducing inflammation and, at high doses, by suppressing autoantibody production. They can be given orally, intravenously or topically as creams, nasal sprays and mouthwashes. If the response to steroid is inadequate or the side effects are unacceptable, steroid-sparing agents such as azathioprine are used.
Other medications, for example tetracycline (an antibiotic with antiinflammatory properties) and nicotinamide, may be considered first line for the treatment of mild to moderate disease. Dapsone and sulphonamides can be useful but have hazardous side effects in the elderly. In general, patients must be monitored until remission and maintained on the lowest does of medication necessary. Importantly, the appearance of occasional blisters does not signify inadequate treatment.
Bullous pemphigoid
BP is more common that PV. In the UK primary care cohort study (Langan et al. 2008), the incidence of BP and PV was shown to be 4.3 and 0.7 per 100 000 person years, respectively. BP tends to affect older patients with a median age of 80 years. It is characterized by itchy, tense, deep blisters commonly found on the limb flexures, hands and feet, spreading to the trunk (Fig. 3). Mucous membranes are involved in approximately 50% of cases. The disease may be generalized or localized to one site.

Bullous pemphigoid.
A variant of BP is found during pregnancy known as pemphigoid gestationis. Itchy blisters begin around the umbilicus and spread symmetrically over the abdomen to the torso and limbs (Fig. 4).

Pemphigoid gestationis.
Blisters are tense because autoantibodies affect proteins lower in the epidermis at the basement membrane. IF shows linear staining of IgG along the basement membrane. The antibodies bind to components of the hemidesmosome adhesion complex, the BP230 and BP180 antigens. In cicatrical pemphigoid, a variant of BP in which the blisters form scars, C3 complement and IgG are found in the lamina lucida of the basement membrane.
BP is treated with prednisolone 40–80 mg per day depending on disease severity. The treatment period is usually 2–3 years with most disease remitting before 5 years. Steroid doses should be reduced after 1–2 months depending on clinical symptoms. In localized disease, potent topical steroids may be sufficient.
Pemphigus vulgaris
PV is characterized by a more superficial intraepidermal splitting of the skin (acantholysis). IF shows intercellular staining of IgG within the epidermis. As a consequence, blisters break more easily than in BP causing erosions that are painful and weeping rather than itchy (Fig. 5). Nikolsky's sign, named after the Russian dermatologist Pyotr Nikolsky, can be demonstrated by the slipping away of the outermost skin layer with gentle rubbing. The blisters are commonly widespread and located primarily on the trunk. In contrast to BP, the oral mucosa is the first site of involvement in the majority of cases. Patients may also have erosions of the conjunctiva and nasal and genital mucosa.

Pemphigus vulgaris.
In hospital studies, PV presents across a wide age range with peaks between the third and sixth decades. Results of the primary care cohort study (Langan et al. 2008) show a median age at diagnosis of 70 years, 10 years younger than BP. Mild disease is treated initially with 40–60 mg prednisolone per day but higher doses of 60–100 mg are necessary in more severe cases. Clinical improvement may be seen within days of starting treatment. If no response is seen within 1 week, the steroid dose may be increased in 50–100% increments. If doses above 100 mg are required, pulsed intravenous methylprednisolone should be considered. The aim is to control disease quickly to reduce the need for long-term maintenance doses. Once symptoms are controlled, tapering of the dose by 50% every 2 weeks is suggested. Treatment is usually lifelong (Table 1). For resistant disease, intravenous immunoglobulins and plasmophoresis may be utilized.
Dermatitis herpetiformis
Dermatitis herpetiformis (DH) is a rare autoimmune blistering disorder of young adult life and has no association with herpes viral infection. It commonly begins between 15–40 years of age and has a slight male preponderance. It is associated with gluten-sensitive enteropathy including coeliac disease, which is often mild. Skin biopsy shows subepidermal blistering with neutrophil microabscesses in the dermal papillae. IF highlights IgA in the dermal papillae and along the basement membrane. Like coeliac disease, autoantibody testing of the blood and small bowel can aid diagnosis. However, if the dermatitis is associated with mild enteropathy, the blood test may be negative.
Intensely itchy blisters may form in small groups on the elbow, extensor forearms, scalp, buttocks and knees. For successful management, a diet free of gluten is vital although this may only have a slow impact on resolution of the rash. Drugs such as sulphonamides and dapsone are therefore important in controlling symptoms but are not curative. The disease has lifelong effects. Dapsone can be used at doses of 50–200 mg per day. The lowest effective dose is used to prevent side effects such as haemolytic anaemia, liver damage and polyneuropathy. The patient should be advised how to recognize a blood problem and must have regular monitoring of both full blood count and liver function.
Linear IgA disease
Linear IgA disease is known as a chronic bullous dermatosis of childhood but may also affect adults. It is a subepidermal disease with IgA present against basement membrane proteins. Similar to dermatitis herpetiformis, it can be managed with dapsone or sulphonamides. Spontaneous resolution usually occurs in 3–6 years.
Nonautoimmune bullous disease
Mechanobullous disease
Epidermolysis bullosa is a rare inherited disorder involving a mutation in the gene for keratin. It results in extremely fragile skin and recurrent blister formation. The severity of disease varies and may be noticed at or shortly after birth. It can be diagnosed antenatally by amniocentesis and management must be in a specialist centre.
Infective disease
Herpes vesicles are a common cutaneous sign in general practice. Chickenpox affects the majority of people before the age of 10 years and 90% of over eighteens have immunity for varicella zoster virus. It is thought that chickenpox is named after the likeness of the vesicles to ‘chick’ peas. The rash usually presents with a fever and forms 2- to 4-mm red papules that develop into clear vesicles. After 8–12 hours, the vesicles turn cloudy and break leaving a crust. The fluid is highly contagious, however, most viral particles are spread from the respiratory tract. Adults and immunocompromised individuals may get severe primary varicella infections.
Herpes zoster or shingles is the name given to the painful blistering eruption following chickenpox. The virus persists asymptomatically in the ganglia of sensory cranial nerves and spinal dorsal root ganglia. As immunity to the virus decreases, the virus reactivates and travels along the nerve often causing a prodrome of pain. This commonly occurs in old age as immunity wanes but is also seen in children. The rash appears in a ‘belt’-like distribution within a dermatome and does not cross the midline. It typically involves the trunk but can affect the face and eye. Postherpetic neuralgia describes dermatomal pain that persists after the rash has disappeared and can be treated with drugs used for neuropathic pain relief (generally amitriptyline or anticonvulsants such as gabapentin or pregabalin).
Another virus commonly found in children is the coxsackie virus. This causes a self-limiting blistering disease known as hand, foot and mouth disease. Small vesicles appear in the mouth followed by the hands, feet and buttocks.
Bacterial infections such as bullous impetigo can also cause blistering. This is a highly contagious disease that primarily affects infants and children younger than 2 years. The blisters are painless and usually form on the trunk, arms and legs. They may scab over with a yellow crust. The most common causative organism is Staphylococcus aureus. Toxigenic forms of this bacterium can also cause a red blistering skin condition known as scalded skin syndrome. Toxins bind to a molecule within the desmosome called desmoglein 1 and disrupt the skin structure giving the appearance of a burn or scald.
Adverse drug reactions
Blistering can be caused by many prescription and over-the-counter medications. Blisters may be localized or widespread and can be severe. A fixed reaction always occurs at the same site of exposure to the drug. The rash may appear 1–2 weeks following first exposure. In subsequent exposures, lesions present within 24 hours. Antibiotics are the most common cause, especially sulphonamides and tetracyclines. Other drugs that commonly cause blistering include nonsteroidal antiinflammatories (NSAIDs) and terbinafine. Approximately 10% of cases of PV cases are drug induced, of which gold, penicillamine and captopril are examples.
Rarely, medications such as tamiflu, NSAIDS and anticonvulsants can rarely cause Stevens-Johnson syndrome in which cell death causes the epidermis to separate from the dermis. Toxic epidermal necrolysis can be considered a severe form of Stevens-Johnson. In this condition, necrosis of keratinocytes usually occurs in the mucous membranes.
Physical causes
Blistering is commonly caused by physical insults to the skin. Extremes of temperature including first- and second-degree burns and frostbite may give rise to blisters. Sun damage can cause blistering and this may be accentuated by phototoxic medications, for example NSAIDS or tetracyclines. Blistering can also be a sign in contact dermatitis. Common aggravating factors are chemical agents such as cosmetics, detergents and solvents, as well as insect bites and stings. Friction or rubbing the skin may also cause blisters especially if the skin is moist. The hands and feet are particularly susceptible because of repetitive motions, such as running in a new pair of trainers.
Eczema
The hands and feet may also blister in a form of eczema known as pompholyx. This is a recurrent dermatosis of the fingers, palms, and soles, characterized by a sudden onset of deep-seated, itchy vesicles. These may later form scaling and areas of lichenification. Treatment is with moisturiser and potent topical steroid.
Key points
Many causes of blistering are self limiting and do not require specific treatment
Primary blistering disorders are rare but carry significant morbidity and mortality. Prompt recognition allows appropriate referral and treatment.
Important aspects in the history of blistering conditions are the age of the patient, prescribed and over-the-counter medication, previous adverse drug reactions, the timing and distribution of the blisters, prodromal or systemic features and the presence of itch or pain
On examination, determine the distribution and depth of the blisters — Nikolsky's sign is a simple way to differentiate the level of skin affected
Biopsy and IF are useful tools in the classification and diagnosis of primary blistering disorders
Ensure follow-up and vigilance for those patients taking immune-suppressing therapies