
Abstract
Urinary incontinence (UI) is a common and important problem, which impacts on the physical, psychological and social well-being of sufferers as well as their families and carers. Most patients with UI can be assessed and managed by GPs without the need for referral to secondary care.
The GP curriculum and urinary incontinence
Manage primary contact with older patients—this includes knowledge of the epidemiology of older people's problems presenting in primary care, and an understanding of the management of the conditions and problems commonly associated with old age [such as urinary incontinence (UI)] Cover the full range of health conditions affecting the elderly—this requires skills in history taking, physical examination and use of ancillary tests to diagnose conditions presented by patients in primary care and skills in therapeutics, including drug and non-drug approaches to treatment of these conditions Coordinate care with other professionals in primary care and with other specialists Understand and implement the key national guidelines that influence health care provision for older people
Demonstrate knowledge of women's health problems, conditions and diseases Demonstrate a reasoned approach to the diagnosis of women's symptoms in a manner that is comfortable for both the patient and the GP using history, examination and incremental investigations and refer appropriately Demonstrate an understanding of the importance of risk factors in the diagnosis and management of women's problems Describe and implement the key national guidelines that influence healthcare provision for women's problems
Prevalence
It is difficult to assess accurately the prevalence of UI as results of studies vary widely. This is a consequence of varying definitions of incontinence, the frequency of incontinence considered to be significant in the studies and the reluctance of patients to admit to incontinence. Women are more at risk of incontinence, with the prevalence increasing with age. The Incontinence Foundation found that one in four women and one in nine men will be affected by a degree of UI at some point during their lives. Other studies have shown that in young adults approximately 20–30% of women are affected; in middle age, this rises to 30–40%, while in elderly women the prevalence is 30–50%.
Risk factors
Female sex is the most important risk factor for developing UI. Other risk factors are listed in Box 1.
In men, UI can follow (or be relieved by) prostate surgery. In both sexes the following are risk factors: drugs (e.g. diuretics), diabetes mellitus, increasing age, cognitive impairment, urinary tract infection and neurological disorders.
Risk factors for UI in women
Pregnancy Vaginal delivery Pelvic surgery Pelvic organ prolapse Conditions that raise intra-abdominal pressure such as chronic constipation, lung disease and occupational and recreational activities Obesity Menopause
Aetiology of incontinence
The main function of the bladder is storage of urine, which is achieved by passive relaxation. Continence requires normal neurological function, a stable detrusor muscle with adequate compliance and a functioning sphincter mechanism. If any of these fail, then incontinence may result.
Incontinence may therefore be caused by the following (Box 2):
Neurological dysfunction Abnormalities of detrusor function Abnormalities of the sphincter apparatus (including surrounding pelvic floor muscles and tissue) Anatomical abnormalities that allow urine to bypass the normal anatomical pathway
Classification of incontinence
Incontinence may be categorized into three main types based on history and examination findings:
Stress incontinence
Stress incontinence occurs when the mechanisms that normally prevent urine from leaking from the bladder are abnormal and can be due to a problem with the sphincter apparatus or secondary to a neurological problem. The patient gives a history of involuntary leakage of urine caused by effort or exertion or on sneezing or coughing. It may be confirmed by asking the patient to cough several times while examining for urinary leakage. When there is an increase in intra-abdominal pressure, this causes the pressure in the bladder to rise until it exceeds the sphincteric closure pressure at the bladder outlet and consequently urine leaks.
Urge incontinence
Overactivity of the detrusor muscle may cause spontaneous contraction of the bladder leading to an uncontrollable leakage of urine preceded by or accompanied by a sudden urge to void. Although the mechanisms that prevent urine from leaking are normal, they are not able to maintain continence in the face of abnormally high bladder pressures.
Mixed incontinence
Mixed incontinence is the common complaint of uncontrollable leakage of urine preceded or accompanied by urgency with additional features of stress incontinence. Careful history taking may determine the predominant factor.
Other types of incontinence
Additionally there are other types of incontinence that do not fit into the categories described above.
Causes of incontinence
Initial assessment
UI is associated with social stigma and patients may find it difficult to discuss issues of continence. It is important to make them feel at ease and be sensitive to their concerns. They may become socially isolated by their condition, preferring to remain at home rather than risking an episode of incontinence while out of the house. Patients may also not appreciate what a common problem incontinence is.
The key to management is careful history taking to define which type of incontinence they are suffering from. A focused history should elicit typical triggers for stress incontinence such as coughing, sneezing, exercise, lifting or rising from sitting (although incontinence caused by an unstable bladder can also occur following rising from sitting). Questions concerning urge incontinence should focus on whether UI is triggered by running taps and cold weather, and patients should be asked if they regularly fail to reach the toilet in time. The degree of UI should also be quantified (i.e. number of pads required per day) and the impact on the patient's life and wish for treatment considered.
Other risk factors should also be inquired about, such as constipation, chronic cough and fluid intake. Patients must be encouraged to drink enough to have a normal urine output of 1000–2000 ml/day and should not restrict their intake below this. They should, however, avoid caffeinated drinks. If a patient has a body mass index (BMI) of greater than 30, they should be encouraged to lose weight as there is emerging evidence that a 5% reduction of BMI can reduce urinary symptoms by up to 50%.
Examination should include a pelvic examination in women to look for evidence of incontinence and associated genital pathology (e.g. pelvic organ prolapse). It also provides the opportunity to assess pelvic floor strength. Abdominal examination is necessary to determine if there is a palpable bladder, and rectal examination will allow palpation of the prostate in men and assessment of anal tone. It will also aid in the diagnosis of constipation. Finally, a neurological screen should be carried out particularly if there is abnormal anal tone or pelvic floor strength.
Management of incontinence affecting women
National Institute for Health and Clinical Excellence (NICE) Guidelines have been produced concerning the management of UI in women. These are summarized in Fig. 1.
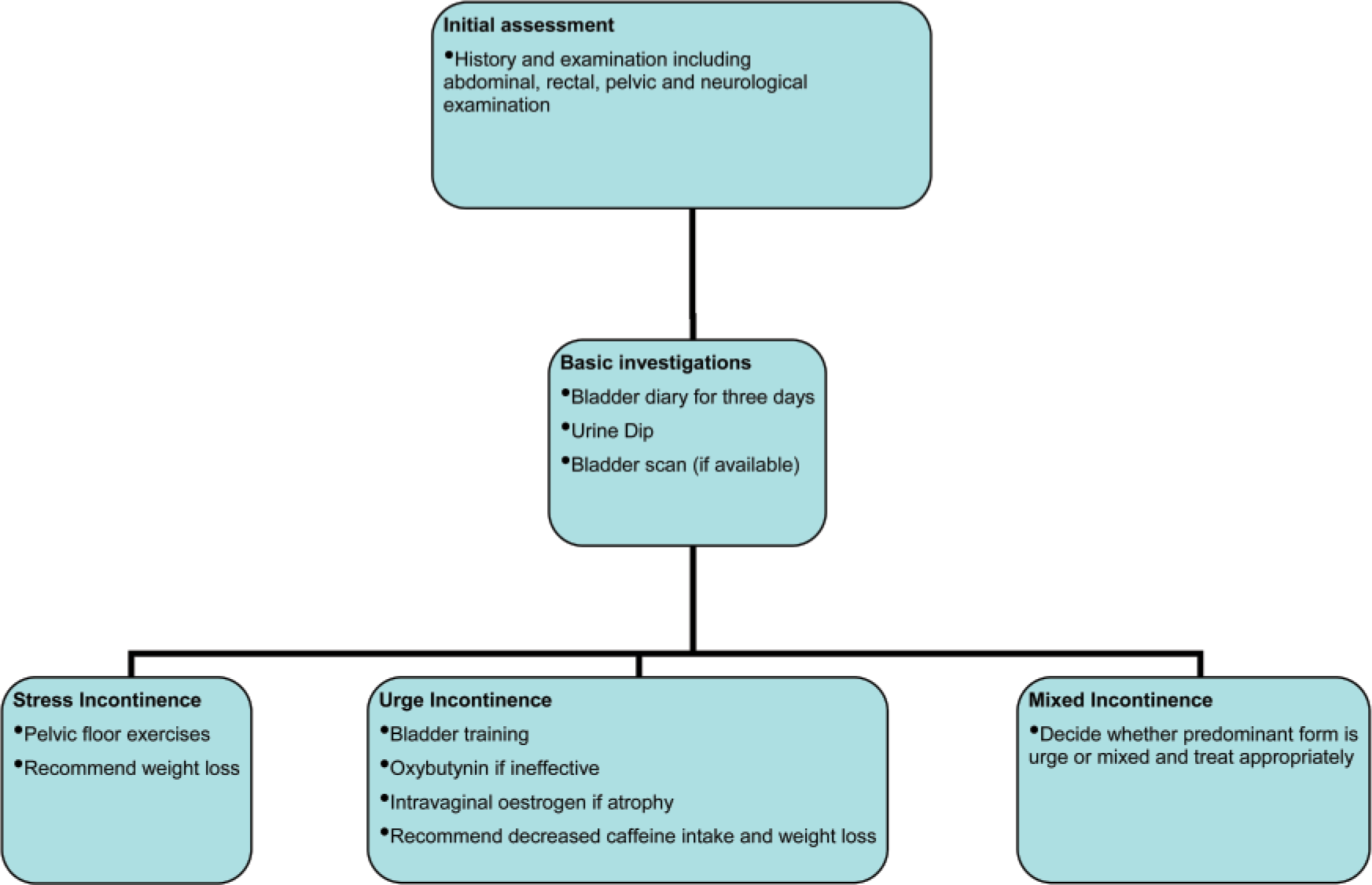
Summary of primary care management of UI in women.
Further assessment
Patients should be asked to complete a bladder diary for 3 days as this gives information about how many incontinence episodes the patient gets and helps quantify urinary frequency. Bladder diaries (Fig. 2) are also useful to provide a baseline to assess how well the patient is responding to treatment. The patient should be asked to measure the volume of urine that they produce and the number of incontinence episodes per day. It is also useful to know their fluid intake. It is normal to pass urine four to eight times per day with a volume of roughly 300–600 ml per void. If the patient voids frequently and does not pass very large volumes, it suggests that they have a poorly compliant or sensitive bladder. There are multiple causes for reduced functional bladder capacity, including overactive bladder (secondary to detrusor overactivity), hypersensitivity related to bladder stones or infection, chronic inflammatory changes and cancer. It is also possible to have reduced functional bladder capacity if the patient is afraid of being incontinent as they may void more frequently.

Example of a bladder diary.
The urine should be dipped in all patients suffering from UI. If there are symptoms of urinary infection, and the urine dip is positive, the patient should be empirically treated with antibiotics until the culture result is back. If there are no symptoms and the urine dip is positive, it is recommended to await the culture result before commencing antibiotics.
If possible, a measurement of the post-void residual with a bladder scanner gives valuable information. A volume of greater than 100 ml is considered significant. If this is not available, then a bladder with more than 300 ml in it is normally palpable in a slender individual. Once it is decided what type of incontinence the patient appears to be suffering from, the following treatments are recommended.
Primary care management of stress incontinence
Pelvic floor exercises have been shown to be useful in stress incontinence, and a referral to physiotherapy services is recommended for a 3 month trial of supervised pelvic floor exercises.
Primary care management of urge incontinence
The recommended first-line treatment for urge incontinence is bladder training for a 6 week period. This helps the patient to regain control of their bladder musculature. Initially, the patient is instructed to void every hour. This interval is then increased by 20 minutes/week so that by 6 weeks, an interval of 2–3 hours is achieved. By the end of the training, the ultimate aim is to void less than eight times per day.
If bladder training is ineffective, then anticholinergic drugs may be useful. These work by inhibiting bladder contractions and also increase bladder capacity. Oxybutynin is the first-line agent, and second-line drugs include darifenacin, solifenacin, tolterodine or trospium chloride. When prescribing these drugs it is important to remember to warn about antimuscarinic side effects, and ensure that there are no contraindications to their use such as closed angle glaucoma. In postmenopausal women with evidence of vaginal atrophy, intravaginal oestrogen may be useful.
Primary care management of mixed incontinence
If possible, try to decide whether the predominant form is stress or urge incontinence and treat the predominant form as suggested above. There is good evidence that pelvic floor exercises and bladder training exercises are useful for mixed incontinence, and antimuscarinics should be offered to women if bladder training has been ineffective.
Referral to secondary care
NICE recommends referral for specialist assessment if any of the criteria in Box 3 are met. In addition, if initial primary care treatment is unsuccessful, or if the diagnosis is in doubt, then consider referral to local urological or urogynaecological services for further investigation and management.
Management in secondary care involves a multidisciplinary team approach. In addition to assessment by a medical practitioner, patients have the opportunity to see a specialist pelvic floor physiotherapist. They should also be offered the opportunity to speak to a continence advisor, a specialist nurse who can offer further advice and counselling for patients with incontinence.
Investigations in secondary care
Investigations may include flow rates and residuals or urodynamics. Urodynamics involves the measurement of bladder pressure during the filling and voiding cycle. It helps to differentiate between detrusor overactivity and stress incontinence and defines the dominant form in mixed incontinence. The test is performed as an outpatient and involves the insertion of two fine catheters into the bladder for filling and pressure measurement and a pressure probe into the rectum to measure intra-abdominal pressure. The bladder is filled until the patient feels comfortably full, then the patient is asked to pass water into a flowmeter.
NICE recommendations for referral

Secondary care management of stress incontinence
The most common surgical interventions include mid-urethral tapes such as tension-free vaginal tapes (TVT) or transobturator tapes (TOT). These act to physically elevate the urethra and bladder neck behind the pubis to prevent urine leakage. Colposuspension is rarely used now. Urethral bulking agents such as collagen injected to bulk up the urethral sphincter may give some success. Further options include artificial urinary sphincters or urinary diversion with an ileal conduit.
Secondary care management of urge incontinence
Options include intravesical botulinum toxin (Botox) injections or insertion of a sacral nerve stimulator. If these more conservative measures are not successful, then augmentation of the bladder or urinary diversion can be considered.
Management of incontinence affecting men
The causes of incontinence in men are similar to those in women, and the initial investigation in males should be carried out as for assessment in women. There are some types of incontinence that are specific to male patients, namely post-micturition dribble and post-prostatectomy incontinence. The European Association of Urology has produced guidelines for the management of UI in men that are summarized in Fig. 3.

Summary of primary care management of UI in men.
Post-micturition dribble
Post-micturition dribble is common and occurs in 17% of healthy males. It is not a feature of prostatic disease by itself and can be safely managed in primary care. A urethral milking technique can be helpful whereby the patient places their fingers behind the scrotum and gently massages the bulbar urethra (that part of the urethra found in the perineum) in a forwards and upwards direction in order to ‘milk’ the remaining urine from the urethra. If this is not successful then pelvic floor exercises are also helpful.
Post-prostatectomy incontinence
Post-prostatectomy incontinence occurs in less than 1% of men after transurethral resection of prostate (TURP) and 0.5% after open prostatectomy for benign disease, although this rises to approximately 10–15% if surgery is performed for cancer. It may be due to damage to the external sphincter mechanism or be due to urge incontinence that was already present prior to surgery. This type of incontinence is treated initially with pelvic floor exercises. If these are unsuccessful, then secondary care referral and surgical options may be considered including: urethral bulking agents, artificial urethral sphincters or urethral slings or tape.
Stress incontinence, urge incontinence and mixed incontinence
Stress incontinence, urge incontinence and mixed incontinence in men are treated in a similar fashion to these problems in women. However, pelvic floor training and bladder training are recommended for all three types of incontinence. Antimuscarinic agents may be useful in men with urge incontinence. Surgical options for men with stress incontinence include artificial urinary sphincter, male urethral slings and bulking agents.
Specialist options for treatment of urge incontinence depend on whether the patient has bladder outflow obstruction or not. If this is present, then alpha-blockers (e.g. alfuzosin) and/or 5α-reductase inhibitors (e.g. finasteride) can be helpful. 5α-Reductase is the enzyme involved in the conversion of testosterone to dihydrotestosterone that is important in the development of benign prostatic hyperplasia (BPH). 5α-Reductase inhibitors therefore slow the progression of BPH. Alpha adrenergic antagonists work by mediating relaxation of smooth muscle within the bladder neck, aiding non-obstructive voiding. If this is unsuccessful, or not acceptable to the patient, then a prostatectomy can be offered. When these more simple measures fail, then patients with urge incontinence can be considered for neuromodulation, bladder augmentation or urinary division.
Indications for referral
The indications for referral for men with UI are shown in Box 4.
Indications for referral in men
Recurrent incontinence Incontinence associated with:
Pain Haematuria Recurrent infections Voiding symptoms Prostate irradiation Previous radical pelvic surgery Any other significant abnormality picked up at initial assessment, e.g. significant post-void residual
Management of incontinence affecting frail older persons
Incontinence becomes increasingly common with age, particularly in patients who are institutionalized. In this group, there are specific and often multifactorial reversible causes to consider. These are summarized in the European Association of Urology Guidelines under the pneumonic ‘DIAPPERS’ (Box 5).
The initial approach to and management of these patients should be the same as that for younger patients where at all possible. The patient's environment can be optimized either with simple measures such as providing a commode or bottle to be kept near the bed or by providing safe and convenient access to the bathroom perhaps by installing handles and mobility aids or setting up single-floor living.
Reversible causes of UI in older people
If active management is not possible due to frailty or cognitive impairment, then conservative measures can be applied such as pessaries for vaginal prolapse, a Conveen or absorbent pads. Indwelling urethral or suprapubic catheters should be used as a last resort as they can be associated with significant complications.
Key points
UI is a common problem especially in women and in the elderly History and examination is the key to deciding what type of incontinence the patient is suffering from (urge, stress, mixed or other) Many patients can be managed successfully in primary care without the need for specialist investigations UI has a significant impact on patients' physical, psychological and social well-being