
Abstract
Diarrhoea is a common clinical problem seen in UK general practice. The perception of diarrhoea varies widely among patients as well as clinicians. Although there is no uniformly accepted definition, diarrhoea is generally agreed to be the abnormal passage of more than three loose or liquid stools per day. Diarrhoea may be termed acute or, if it lasts for more than 4 weeks, chronic. Chronic diarrhoea affects 4–5% of the adult population in the UK.
The GP curriculum and chronic diarrhoea
GP
Demonstrate an understanding of national guidelines that influence health care provision for digestive problems Manage primary contact with patients who have a digestive problem Recognize that some patients may find digestive problems embarrassing to discuss openly. Therefore, adopt a non-judgemental, caring and professional approach towards patients with digestive problems. Understand the principles of treatment for common conditions managed largely in primary care, such as diarrhoea Recognize the effects psychological stress can have on the gastrointestinal (GI) tract, especially with functional disorders Provide advice on dietary and lifestyle interventions (smoking cessation and alcohol reduction) Recognize and respond urgently to ‘red flag’ symptoms Explain the indications for urgent referral to specialist services for patients with suspected GI malignancy Be aware of secondary care management of digestive problems, including surgical options
Pathophysiology and classification of chronic diarrhoea
Box 1 lists important causes of chronic diarrhoea in adults. Chronic diarrhoea can be classified according to the mechanism involved.
Osmotic Secretory Inflammatory (exudative) Altered motility
Osmotic diarrhoea
The gut mucosa acts as semipermeable membrane and fluid shift occurs if there are large amounts of non-absorbable hypertonic solutes present within the lumen. Common causes of osmotic diarrhoea include lactulose therapy, antacids and malabsorption.
Secretory diarrhoea
Secretory diarrhoea results from two processes: increased secretion of fluid together with reduced absorption. Examples of secretory diarrhoea include diarrhoea caused by drugs such as antibiotics or antidepressants, diarrhoea caused by bacterial enterotoxins (for example, Campylobacter or Clostridium diarrhoea) and diarrhoea caused by excess hormone secretion (for example, that caused by insulinoma).
Inflammatory diarrhoea
Inflammation and ulceration of the colon lead to impaired absorption and result in loss of mucus, pus or blood in the bowel lumen and thus diarrhoea (see Figs. 1 and 2). Examples of inflammatory diarrhoea include diarrhoea associated with inflammatory bowel disease and that associated with bacterial or parasitic colonic infections.

Normal colon as seen at colonoscopy.

Ulcerative colitis seen at colonoscopy: severe inflammation, oedema and ulceration of the colonic mucosa.
Altered motility
Altered motility of the bowel prevents normal transit of bowel contents and thus limits absorption. Common examples for this type of diarrhoea include diarrhoea associated with diabetes (secondary to autonomic neuropathy), diarrhoea caused by certain drugs (for example, erythromycin), diarrhoea that occurs post-gastrectomy and diarrhoea associated with irritable bowel syndrome (IBS).
Assessment of chronic diarrhoea in primary care
The British Society of Gastroenterology recommends that initial assessment of adults with chronic diarrhoea should be carried out in the primary care setting. However, it can be a difficult task to distinguish between functional and organic causes based on symptom reporting alone. As IBS may affect up to 15% of the population, there is clearly the potential for inappropriate investigations of patients reporting diarrhoeal symptoms. Therefore, a detailed history and careful examination are essential in the initial assessment of any patient with chronic diarrhoea.
Causes of chronic diarrhoea
Infection
Giardiasis Amoebiasis
Clostridium difficile
Cryptosporidium — particularly if immunocompromised
Inflammation
Crohn's disease Ulcerative colitis Non-specific inflammatory colitis
Neoplasia
Colon cancer Intestinal lymphoma Carcinoid
Malabsorption
Bacterial overgrowth Chronic pancreatitis Coeliac disease Bile salt malabsorption
Endocrine
Diabetes mellitus Thyrotoxicosis Addison's disease Insulinoma
Drugs
Antibiotics Proton pump inhibitors Colchicine Metformin
Functional
Irritable bowel syndrome (IBS)
Others
Alcohol Bowel resection Constipation with overflow diarrhoea Diverticular disease
History
The history remains the most important tool for GPs in the assessment of adult patients with chronic diarrhoea. Points to cover in the history are summarized in Box 2. Start with open questions and then focus your enquiry to:
Establish that the symptoms are organic as opposed to functional Assess for any specific cause of the diarrhoea Distinguish malabsorption from infective or inflammatory forms of diarrhoea Identify high-risk features for suspected cancer
Symptoms suggestive of organic disease include a history of diarrhoea of less than 3 months duration, nocturnal or continuous diarrhoea and significant weight loss. Inflammatory or secretory forms of diarrhoea typically present with loose stools sometimes mixed with blood or mucous. They can also be associated with abdominal pain. Malabsorption is often accompanied by bulky light-coloured stools that are difficult to flush and have an offensive odour.
Points to cover in the history
Presenting complaint
Duration of the diarrhoea—termed ‘chronic’ if persists more than 4 weeks Nature of the diarrhoea—colour, consistency and presence of blood/mucus Contact with anyone else with similar symptoms? Travel history Other associated symptoms, e.g. fever, abdominal pain, vomiting and weight loss
Surgery—especially ileal resection that can cause ‘short bowel syndrome’ and cholecystectomy (up to 10% develop chronic diarrhoea) Pancreatic disease Systemic disease, e.g. diabetes mellitus, thyrotoxicosis, adrenal disease, systemic sclerosis and amyloidosis
Regular medications cause up to 4% of chronic diarrhoea—examples of drugs causing diarrhoea include magnesium-containing products, non-steroidal anti-inflammatory drugs, antiarhythmics, proton pump inhibitors and chemotherapy Recent antibiotics
Inflammatory bowel or coeliac disease Bowel cancer
Alcohol consumption—high intake is associated with diarrhoea
How does the patient see the problem? What does he/she think is wrong? What does the patient want you to do about it?
High-risk or red flag features for colorectal malignancy include:
Age over 60 years Persistent rectal bleeding without anal symptoms Persistent change in bowel habit (more than 6 weeks duration, especially to looser stools) Weight loss Unexplained iron-deficiency anaemia Significant family history
In the absence of such symptoms in patients who first present under the age of 40 years, a functional cause or IBS should be considered, particularly if physical examination and baseline investigations are normal and the Rome criteria are met (see Box 3).
Examination
Start by assessing baseline observations (temperature, pulse and blood pressure), hydration and nutritional status. This helps to establish whether the patient is unwell with diarrhoea.
Rome II criteria for diagnosis of IBS
Symptoms of abdominal discomfort or pain, for at least 3 days a month in the past 3 months, associated with two or more of the following features:
Pain is relieved with defecation Onset is associated with change in stool frequency Onset is associated with change in stool form
When examining the abdomen, look for scars that might indicate previous surgery. Feel for tenderness, organomegaly or palpable masses. The National Institute for Health and Clinical Excellence (NICE) (2005) recommends that a digital rectal examination should always be performed in patients with unexplained symptoms related to the lower GI tract, provided that it is acceptable to the patient. This may reveal tumour mass or faecal impaction.
Investigations
The British Society of Gastroenterology (2003) recommends the following baseline investigations for patients with chronic diarrhoea presenting to primary care:
Stool microscopy and culture if an infectious aetiology is suspected Blood for full blood count, erythrocyte sedimentation rate (ESR) and/or C-reactive protein, urea and electrolytes, liver function tests, serum calcium, haematinics (B12, folate and ferritin) and thyroid function and serological tests for coeliac disease (and IgA level)
Do not delay referral for patients who need acute admission or meet 2 week wait criteria to perform investigations in primary care. Further investigations will depend on the likely cause of the diarrhoea.
Management of chronic diarrhoea in primary care
The management of patients presenting with chronic diarrhoea to primary care is summarized in Fig. 3.

Management of patients presenting with chronic diarrhoea to primary care.
Patients requiring acute admission
Admit as an acute medical emergency if the patient has:
Severe abdominal pain (especially if associated with tenderness) Severe diarrhoea (more than eight stools a day) with or without rectal bleeding Significant rectal bleeding Dramatic weight loss Dehydration and the patient is unable to tolerate sufficient oral fluids Fever in excess of 37.5°C, tachycardia of more than 90 beats per minute, hypotension or other signs of systemic disease (such as a raised ESR or raised white cell count)
Patients not requiring acute admission
If there is an obvious identifiable cause of the patient's diarrhoea, for example, GI infection, overflow diarrhoea secondary to constipation or diarrhoea resulting from drug side effects, then treat the patient and review after treatment. Refer to gastroenterology if treatment does not relieve the symptoms.
If the patient has symptoms suggestive of functional bowel disease and is under 40 years of age with normal investigations, IBS is likely. Reassure, offer advice and review as necessary. Refer to gastroenterology if atypical symptoms appear or the patient is unhappy with the diagnosis.
In all other cases, refer to gastroenterology for assessment. Speed of referral depends on the patient's age and severity of symptoms.
Refer immediately for secondary care outpatient assessment if the patient is having an exacerbation of known inflammatory bowel disease. Often, these patients have direct access arrangements with the specialist GI team that looks after them on an ongoing basis.
Refer under the 2 week wait rule for outpatient assessment by a team specializing in the treatment of lower GI malignancy if NICE referral criteria are met (Box 4). Red flag symptoms suggestive of bowel cancer include unintentional and unexpected weight loss, persistent change in bowel habit for 6 weeks or more in anyone aged over 60 years, iron-deficiency anaemia not related to menstrual loss or rectal bleeding that does not clearly originate from haemorrhoids or an anal fissure. In addition, consider immediate referral if the patient has a family history of bowel or ovarian cancer.
NICE referral guidelines for suspected lower GI cancer
Refer urgently to be seen within 2 weeks by a team specializing in lower GI malignancy if:
right lower abdominal mass consistent with involvement of large bowel a palpable rectal mass (intraluminal, not pelvic; a pelvic mass outside the bowel would warrant an urgent referral to a urologist) unexplained iron-deficiency anaemia (haemoglobin of 110 g/dl or less for men or 100 g/dl or less for non-menstruating women)
rectal bleeding persisting for 6 weeks or longer without a change in bowel habit and without anal symptoms change in bowel habit to looser stools and/or more frequent stools persisting for 6 weeks or longer without rectal bleeding
Secondary care investigations
Secondary care investigations depend on the underlying pathology suspected. Typical investigations include:
Small bowel lesions/malabsorption—endoscopy, distal duodenal biopsies, barium follow through and hydrogen breath testing for bacterial overgrowth Pancreatic lesions—computed tomography scan of the pancreas, faecal elastase, endoscopic retrograde cholangio pancreatography (ERCP) and magnetic resonance cholangio-pancreatography (MRCP) Terminal ileal disease—barium follow through, 99mTc-labelled white cell scanning (terminal ileal Crohn's disease) Colonic pathology—flexible sigmoidoscopy if aged under 45 years. If aged over 45 years, colonoscopy is the preferred investigation (see Fig. 4).
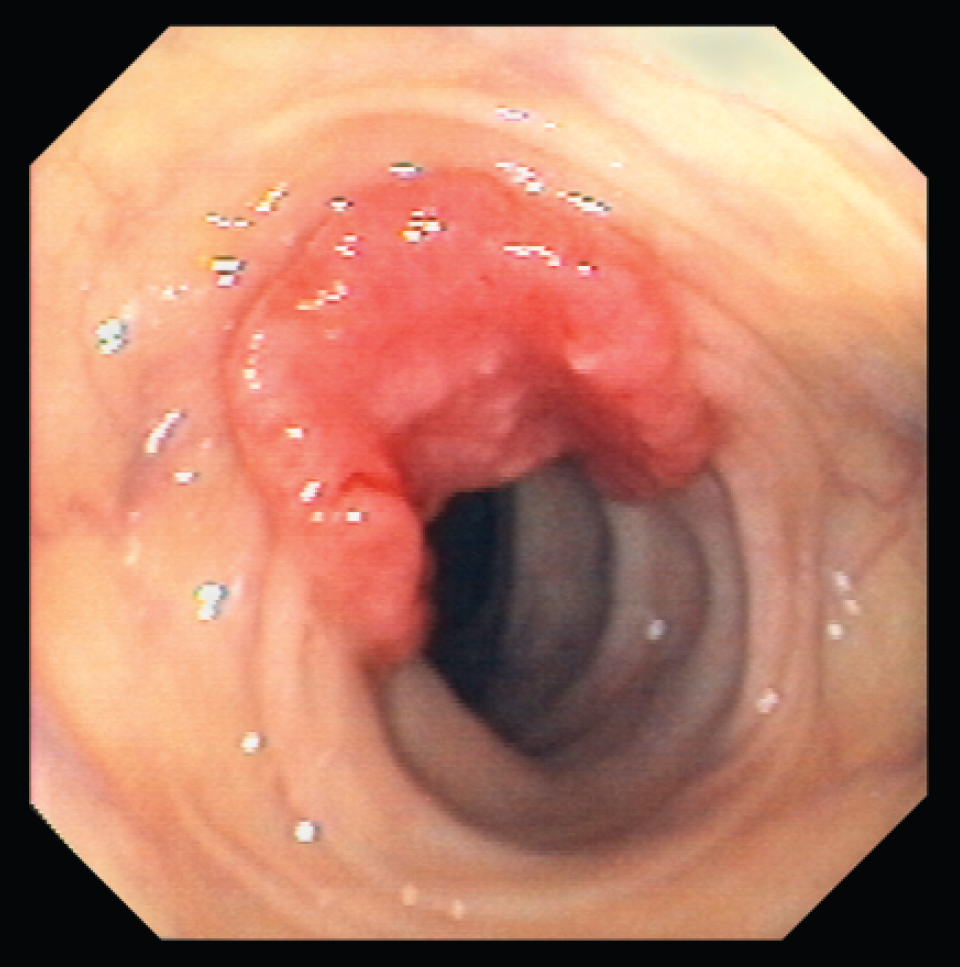
Carcinoma of the colon seen at colonoscopy.
Specific causes of diarrhoea
The following conditions causing diarrhoea can be managed in primary care without the need for specialist GI referral.
Overflow diarrhoea
Among elderly patients admitted to hospital with non-malignant disease, constipation with faecal impaction and overflow of watery stool accounts for over half of all cases of diarrhoea. Other patients prone to overflow diarrhoea include patients with terminal illness and those on opioid medication for other reasons.
For these patients, treatment with antidiarrhoeal agents makes matters worse. Treatment is as for constipation with rectal laxatives (such as glycerol or bisacodyl suppositories and/or enemas) together with stool softeners. Stimulant laxatives such as senna may cause colic.
Irritable bowel syndrome
Twenty percent of people develop symptoms of IBS in their lifetime. Loose stools and/or urgency of defecation are common symptoms of IBS, and these are often associated with symptoms such as abdominal pain or bloating.
IBS is a diagnosis of exclusion. How far to investigate is a clinical judgement weighing risks of investigation against possibility of serious disease. Factors to take into consideration include the age of the patient, family history, length of history and symptom cluster.
Education and reassurance form the basis of management of symptoms in these patients. Lifestyle and dietary measures must be tried before trying pharmacotherapy. Information leaflets are helpful. Encourage effective use of leisure time and regular physical exercise.
For patients with diarrhoea-predominant IBS, dietary advice should include:
Eat regularly and take time to eat—avoid long gaps between eating or missing meals Drink at least eight cups of fluid daily—but restrict tea and coffee to three cups per day and reduce intake of fizzy drinks and alcohol Reduce intake of high-fibre foods such as brown rice, wholemeal bread and cereals high in bran Reduce intake of ‘resistant starch’ found in processed or re-cooked foods Limit fresh fruit to three portions per day (a portion is about 80 g) Avoid sorbitol, an artificial sweetener, as this can make diarrhoea worse Try a 4 week trial of probiotics Up to 50% of patients with diarrhoea-predominant disease are helped by exclusion of certain foods—food diaries may help identify foods that provoke symptoms. Common candidates are dairy products, citrus fruits, caffeine, alcohol, tomatoes, gluten and eggs. Consider referral to a dietician for an exclusion diet. For wind and bloating consider increasing intake of oats (e.g. oat-based breakfast cereal or porridge) and linseeds (maximum one tablespoon daily)
Antidiarrhoeal preparations taken as required (for example, loperamide) may be helpful in controlling symptoms of diarrhoea-predominant disease. Avoid codeine phosphate as this may cause dependence. Use pre-emptive doses to cover difficult situations such as air travel.
Other treatments that may help patients with IBS include antispasmodics (such as mebeverine or peppermint oil taken as needed) and antidepressants (in particular, low-dose amitriptyline). If a patient fails to respond to treatment, consider another diagnosis. Review the history and examination and consider referral for further investigation.
Factitious diarrhoea
Factitious diarrhoea is responsible for 4% of referrals to gastroenterology departments and 20% of tertiary referrals. It is caused by laxative abuse or the adding of water or urine to stool samples. It can be difficult to spot: have a high index of suspicion especially in patients with history of eating disorder or somatization.
Key points
Digestive problems are common presentation to general practice, and the GP has a central role in their diagnosis and management Some patients may find digestive problems embarrassing to discuss openly and so it is important to adopt a non-judgemental, caring and professional approach History taking remains the most important tool for GPs in the assessment of patients with chronic diarrhoea Patients with chronic diarrhoea with an obvious underlying cause that can be treated in the community or those under the age of 40 years with symptoms suggestive of IBS can be managed in primary care All other patients with chronic diarrhoea should be referred for specialist assessment—the presence of ‘red flag’ symptoms or signs should trigger urgent referral For patients initially managed in primary care, atypical symptoms or failure of symptoms to respond as expected to primary care treatment warrant referral for specialist assessment.