
Abstract

This competence is about maintaining the performance and effective continuing professional development of oneself and others.
The fourth and final competence progression in this performance area takes us into a developing area, i.e. that of doctor as teacher. The behaviours are described in Fig. 1. Looking at each of the word pictures in turn:
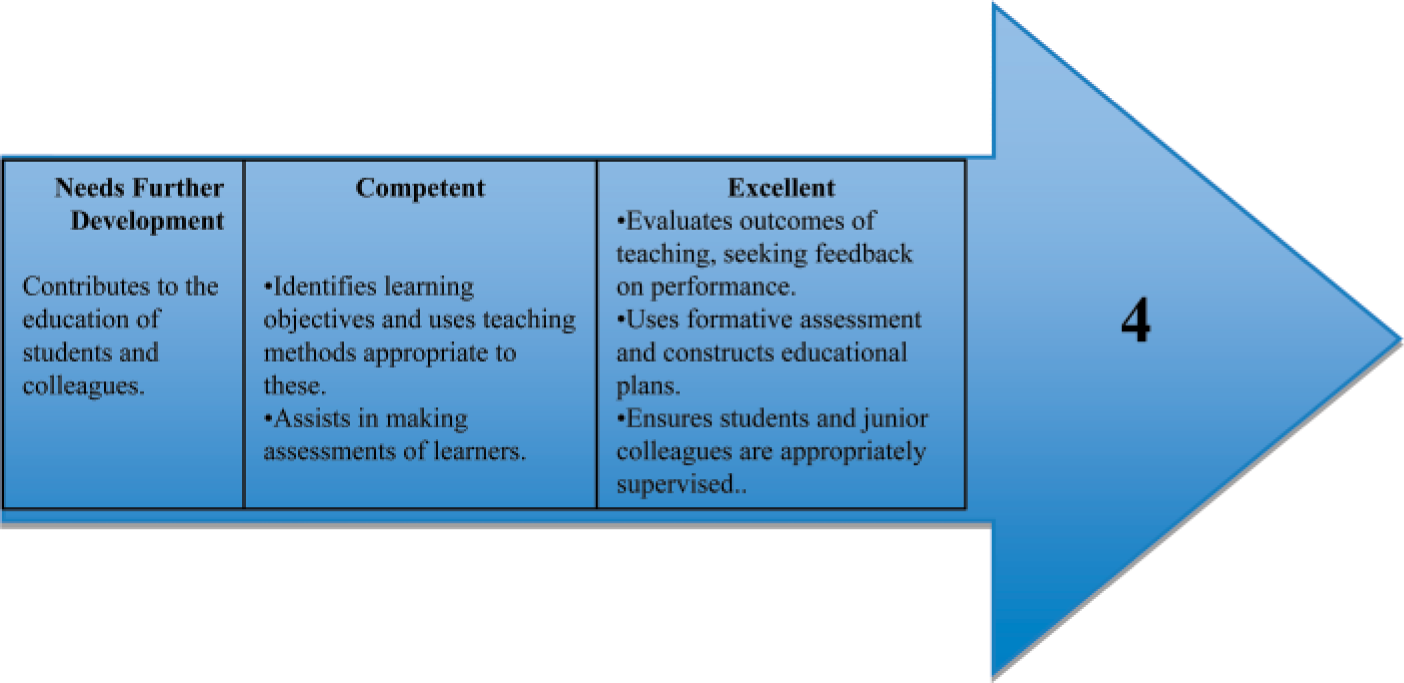
The fourth competence progression of maintaining performance, learning and teaching.
The first competence is at a basic level and requires us to engage with the education that goes on around us. ‘Good medical practice’ encourages doctors to regard teaching as being part of routine medical practice. For a non-specialist teacher, this can simply involve playing a role in the educational programmes that go on in the practice, for example, by allowing students to sit in and observe the consultation, by answering queries of those in training or by becoming more involved in debriefing and case discussion.
The curriculum has a statement devoted to this area, in which it suggests that we should be able to:
Understand how adults learn Demonstrate an awareness of the differing learning styles of individuals Demonstrate a learner-centred approach to teaching Demonstrate the ability to facilitate the learning of a small group Deliver a presentation clearly and effectively, contribute positively to a culture of teaching and learning within the practice organization Understand the benefits of inter-professional and multi-professional learning Demonstrate the ability to give effective feedback to a colleague
We will consider some of these issues below:
The learners that we come across in general practice are adults, rather than children, and ‘adult learning’ has some particular characteristics. Being mature and independent individuals, adults particularly value their autonomy and usually they learn better if allowed to be self-directed. This is not an absolute. For example, it does not mean that learners should be allowed to sink by virtue of having no direction at all. If they are in situations that are entirely new to them, it would be appropriate for the GP to direct their learning rather than leave them to flounder and become dispirited.
Learning through experience is particularly valuable, especially if new experiences are embedded or purposefully connected with previous experiences and insights. In this way, learners can put new knowledge, skills and attitudes into a context that they already understand. Connecting new experiences with old ones is also a mechanism that allows new learning to gain a sense of proportion. We have a role in creating these important connections, for example, by asking ‘how does this differ from what you already know’ and ‘what would you now do differently?’
The discomfort that learners experience when exposed to situations that they find difficult is a powerful motivator for learning. Teachers can hopefully ‘sensitize’ learners so that they learn to recognize their own areas of discomfort and act upon them rather than ignoring them.
In summary, adult learning is most effective when it is clearly relevant to the reality of working life, relates theory to solving practical problems and encourages reflection. All these components need to be considered in preparing for teaching.
Learning in primary care is a team exercise. Therefore, learning with other doctors (inter-professional learning) and with other members of the team (multi-professional learning) can be invaluable provided that it addresses shared needs. For example, revising the family planning protocol is better if the doctors and the nurses who run the clinic do so in collaboration.
Teaching is not entirely for the learner's benefit. Indeed, preparation for teaching is an excellent form of continuing professional development because it influences attitudes and behaviour in the consulting room and thereby improves patient care. Educational skill and insight encourage doctors to see patients as both learners and teachers, improving shared understanding and therefore the quality of patient management.
To be ‘competent’, doctors should demonstrate that they are able to help learners convert broad areas of educational need into manageable tasks or ‘objectives’. Objectives should be written in such a way that the task is clear. Good objectives are said to be SMART, meaning that they are
The teaching methods should address these, but again they need not be complicated. For example, if a learner lacks a skill such as soft tissue injection, s/he may learn better by going to a clinical skills laboratory or being taught through practical demonstration than by being given a talk or shown a video.
The second of the ‘competent’ descriptors refers to our willingness to engage in making formative assessments that assist the learner's development. These assessments need be no more complicated than giving constructive feedback. Many doctors are asked to do this as part of multi-source feedback. Where there is opportunity for the feedback to be more detailed, the principles of doing this effectively should be observed. For example, feedback should be specific, based on evidence such as the observation of behaviour, actionable (i.e. something can be done in relation to it), balanced and feasible.
There are other guidelines about how best to deliver feedback, such as Pendleton's rules, that are worth knowing about.
These ‘excellent’ competences require doctors to show more advanced educational expertise. At present, these abilities may be witnessed in many training practices but doctors who are not involved in education are unlikely to have the need or the opportunity to demonstrate these skills.
In the future, involvement in the teaching of doctors and other primary health care professionals will become a more routine part of every GP's core functions at which time these skills will no longer be the sole concern of specialist educators.