
Abstract
Hip pain can affect patients of all ages with vastly differing presentations. Presentation may be acute or insidious, and the patient may present with limp, immobility or no functional disturbance. Pain in the hip can also be misleading due to referred pain from the lumbar spine, abdomen, pelvis or knee.
The GP curriculum and hip pain
Manage primary contact with patients who have hip pain Explain the aetiology and natural history of common and important conditions of the hip Describe the indications for referral within a suitable time frame Describe the epidemiology of disorders of the hip at all ages and apply this when developing a differential diagnosis Assess the mechanism of injury when considering diagnosis Distinguish inflammatory from non-inflammatory conditions Describe when blood tests and imaging methods are required for diagnosis of musculoskeletal problems Facilitate self-help strategies to empower the patient Avoid investigations or treatments that are unlikely to alter outcomes Describe the key national guidelines that influence health care provision for hip disorders
Understanding the anatomy of the hip and its pathology will aid the clinician in forming succinct differential diagnoses. The majority of hip pathology is related to age, due to changes in developing anatomy and environmental and physical demands (see Table 1). With a focused history and examination it is possible to accurately diagnose hip pathology and guide investigation and management appropriately. This article aims to look at the common causes of hip pain in the adult population, although some pathologies may display a degree of overlap.
Common pathology of the hip causing pain, related to age

Trauma
Trauma to the hip can be due to single episodes, resulting in injury from simple contusions to fractures of the proximal femur, neck of femur, acetabula or pubic rami. Equally, it can be cumulative with patients presenting with pain from sprains and tendonitis to stress fractures. Diagnosis of trauma-related hip pain can usually be gained through a thorough history, with examination confirming suspicions, revealing localized areas of tenderness or pain on stretching the sprained inflamed tendon.
However, in an ageing population, a high index of suspicion should be used when approaching the patient with increased confusion or recent unexplained deterioration in mobility. If there is any clinical suspicion, then investigation should be sought with two plane radiographs to rule out fracture as minor trauma (a fall from less than the height of a chair) to the hip can easily result in fragility fractures in the elderly as a result of to osteoporosis. With a reported 30% of over 65s having a fall each year, it is also advisable to take a full falls history and manage appropriately to reduce the risk of further falls and therefore fragility fractures.
Osteoporosis and hip fracture
The National Institutes for Health define osteoporosis as ‘a systemic skeletal disease characterized by low bone mass and micro-architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture’. The World Health Organization classifies osteoporosis into four groups according to bone mineral density: normal, osteopenia, osteoporosis and severe osteoporosis. It is estimated that there are 180 000 osteoporosis-related fractures in the UK each year and 70 000 of these are to the hip. Diagnosis of osteoporosis is confirmed with dual-energy X-ray absorptiometry (DEXA) scanning. However, osteoporosis can be assumed in any woman sustaining a fragility fracture, such as a fractured neck of femur, who is over the age of 75. A previous InnovAiT article summarizes the secondary prevention of osteoporosis (Davies, 2008).
Transient osteoporosis (also referred to as transient bone marrow oedema) of the hip is an uncommon condition of unknown aetiology and must be considered a diagnosis of exclusion. Most commonly affecting middle-aged men and women in the third trimester of pregnancy, it presents with sudden onset of hip, groin and/or thigh pain. Even if a patient has minimal pain, walking may still be problematic. The reason for this is unclear but it may result from alterations in the femoral head sphericity. Transient osteoporosis is usually unilateral although can affect other joints in up to 40% of cases. Plain radiographs show the early subtle signs of osteoporosis; however, there is a 1–2 month lag behind clinical symptoms. Magnetic resonance imaging (MRI) is usually necessary to confirm diagnosis. The natural history is for resolution within 6–12 months and treatment is therefore supportive, offloading the joint through the use of mobility aids. Referral for a specialist opinion should be sought if this condition is suspected and other causes of hip pain have been ruled out.
Avascular necrosis
Avascular necrosis (AVN) of the femoral head is most commonly secondary to trauma and fracture of the femoral neck. In a small population, however, AVN can be non-traumatic in origin with aetiologies including inter-osseous hypertension, fat embolism, steroid therapy, alcohol excess, immune suppression and haemoglobinopathies (such as sickle-cell anaemia).
Typical presentation is in the young to middle-aged patient, often with increasing bilateral pain on weight bearing, standing or walking and persisting pain at rest. Investigation with plain radiographs shows early subtle signs that are often missed, including loss of joint space and flattening of the femoral head prior to sclerotic changes, subchondral fracture and ultimately collapse of the femoral head. These changes may lag behind the clinical picture. If diagnosis is prompt, then revascularization techniques can be trialled (e.g. drilling of the cortex); however, ultimately if progression is severe, then arthroplasty is the only surgical option.
Trochanteric bursitis
Trochanteric bursitis is the most common cause of soft tissue hip pain and deserves individual mention. The trochanteric bursa lies between the greater trochanter and the gluteal muscles and iliotibial tract (see Fig. 1). Inflammation can be due to either a single direct trauma or a repetitive trauma from exercise. Patients classically complain of lateral hip pain, commonly radiating down the thigh that is worse on exercise or when lying on the affected side, disturbing sleep. Bursitis can result in a sensation of decreased power due to pain inhibition and therefore decreased levels of activity. Examination will reveal point tenderness over the bursa with normal ranges of hip movement.
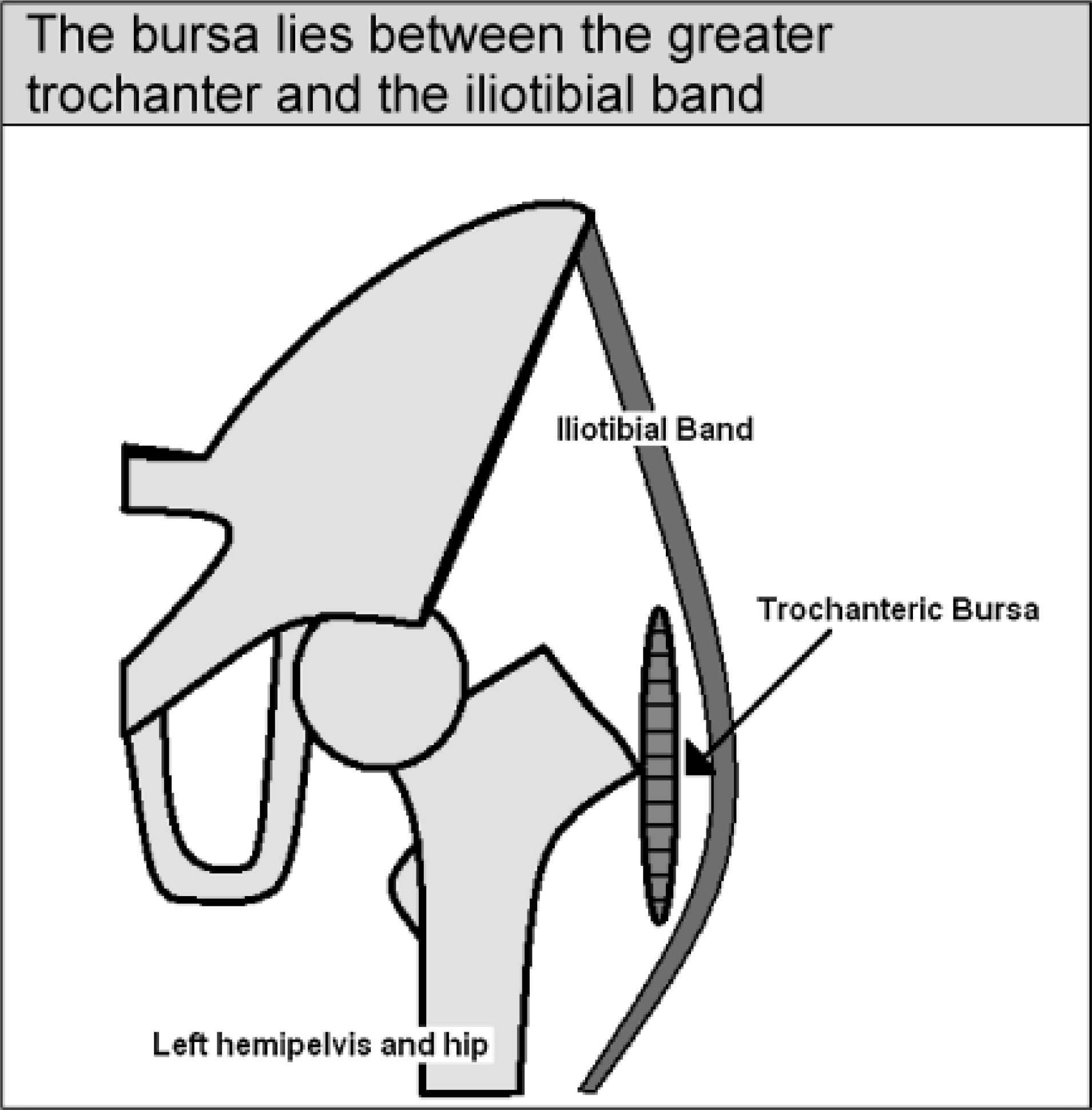
Trochanteric bursa. The bursa lies between the greater trochanter and the iliotibial band.
Management is with advice and reassurance, avoidance of aggravating activity and stretching of the iliotibial tract. This can be achieved either in the standing position by leaning side on to a wall with the feet crossed and the affected hip closest to the wall and stretching the affected hip towards the wall or supine with the affected hip flexed and adducted with subsequent use of the upper limbs to encourage adduction and increase the stretch.
The natural prognosis is for complete resolution; however, symptomatic therapies including non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroid injection can be of benefit both symptomatically, providing a 60–66% improvement at 1 year and therapeutically giving a 2.7-fold increase in resolution at 5 years. Referral to an orthopaedic surgeon is rarely indicated if pain is refractory to primary care management.
Impingement
Femero-acetabular impingement, unlike other hip pathologies, does not result from a change in the weight-bearing surface of the hip but abnormal contact between the femoral neck and the acetabulum at the extremes of movement. Two mechanical pathologies have been identified as demonstrated below (see Fig. 2), resulting in significant chondral injury. It is even suggested that up to 90% of previously diagnosed primary hip osteoarthritis (OA) can be attributed to an underlying mechanical abnormality.

Impingement syndromes. With movement of the hip and a pincer deformity, the acetabulum will impinge before a full range of movement is achieved, whereas in a cam deformity excess bone on the femur results in impingement on the acetabulum prior to achieving full range of movement. In practice, the two impinging pathologies often coexist.
These syndromes are most likely to present insidiously in young athletes or patients subjecting the hip to supra-physiological ranges of motion. Patients may describe symptoms of locking, giving-way, clicking and snapping. Limited hip movement may be a complaint; however, pain increasing with hip flexion and prolonged sitting is typical, limiting sporting activity. Impingement testing is usually positive, with groin pain on hip flexion, adduction and internal rotation.
Suspected impingement requires referral for specialist investigation as delay in diagnosis and treatment will result in significant chondral injury and expedite the need for future arthroplasty to alleviate secondary OA. Conservative treatment requires the use of analgesics and exercise modification to limit impinging ranges of movement, with physiotherapy and stretching exercises often exacerbating symptoms. Surgical intervention is usually indicated to restore normal mechanics, reduce symptoms and prevent further injury.
Arthritis
Arthritis of the hip can be divided by cause into degenerative, inflammatory and infective types. These can primarily be distinguished by their history of presentation.
Osteoarthritis
OA is a degenerative disease caused by the inability of the chondral cartilage to repair itself with the subsequent wear and tear leading to degenerative changes within the joint. It is most commonly age related (primary OA) or secondary to previous disease or injury (secondary OA). OA classically presents with a consistently progressive groin and thigh pain that escalates with physical activity and eases with rest, together with stiffness reducing the ability to ‘tie shoe laces’ or ‘cut toenails’. Examination reveals reduced ranges of all movement and often fixed flexion, adduction and external rotation deformities. Radiographs show typical loss of joint space, subchondral sclerosis and cysts and the formation of osteophytes (see Fig. 3).
OA accounts for 15% of all musculoskeletal consultations in the over 45 age group rising to 25% in the over 75s. The prevalence of radiological osteoarthritic changes in the hip in the adult population is 11%; however, only 5% will be symptomatic. Clinical diagnosis based on the presence of all the following clinical features precludes the need for immediate radiological investigation:
Persistent joint pain increasing with use Age greater than 45 years Morning stiffness lasting no more than half an hour
Management of OA hip requires a conservative, medical and surgical approach. Conservative treatment aims to modify environmental and lifestyle risk factors including obesity, muscle weakness and occupational or recreational joint stress, along with offering patient education. The core treatment is controlled exercise to encourage weight loss and increase local muscle strength and general aerobic fitness. Non-pharmacological treatments include transcutaneous electrical nerve stimulation (TENS) and the use of walking aids.
Pharmacological management includes the use of the analgesic ladder starting with simple paracetamol at a dose of 1 g four times daily taken regularly. If this is not controlling pain, consider adding an oral NSAID, if not contraindicated, with proton pump inhibitor cover. If combination treatment is not effective or NSAIDs are contraindicated, consider adding an opioid such as codeine 30–60 mg four times daily.
Referral for surgery should be considered in patients who are symptomatic, with a significant impact on their activities of daily life and who have been shown to be refractory to non-surgical interventions. Referral should be made prior to establishment of functional limitation. The Oxford Hip Score (Dawson et al., 1996) is now widely used for the assessment of patients with hip arthritis and may provide guidance on when to refer for a specialist orthopaedic assessment (Fig. 4 or online at www.orthopaedicscore.com/scorepages/oxford_hip_score.html).

Bilateral severe hip arthritis.

Oxford hip score. (As a guide, a score of 0–19 is suggestive of severe arthritis and necessitates referral for specialist opinion, 20–29 is suggestive of moderate to severe arthritis, non-medical management should be optimized and a surgical referral considered, 30–39 is suggestive of mild to moderate hip arthritis with no immediate need for surgical review and a score greater than 40 suggests no significant joint derangement.) Oxford Hip Score © Isis Innovation Limited, 1996. All rights reserved.
Rheumatoid arthritis
Rheumatoid arthritis (RA) is an inflammatory process. It results in a destructive arthropathy that rarely affects the hip. However, when the hip is affected, the outcome is usually severe with intense pain and limitation of movement. Examination reveals a fixed flexion deformity often with an adduction deformity and wasting of the gluteal and thigh muscles. Radiographs show a typical diffuse destruction of the articular cartilage with joint narrowing, inward protrusion of the soft medial wall of the acetabulum and medialization of the femoral head, together with subsequent secondary OA.
Affecting an estimated 1.1% of the population, RA is a systemic disease affecting multiple joints and body systems. Initial investigation should include blood tests for rheumatoid factor and C-reactive protein.
As with OA, physiotherapy plays a vital role in improving general fitness, enhancing joint flexibility, improving muscle strength and overcoming functional impairments. Non-pharmacological treatment includes the use of TENS. Pharmacological treatment can be classified as either symptomatic or disease modifying. Disease-modifying treatments should always be consultant led and include corticosteroids, sulfasalazine, methotrexate and anti-tumour necrosis factor (anti-TNF).
Referral for specialist opinion should be made for any patient with suspected RA affecting the hands or feet, more than one joint, or where there has been a delay to presentation of more than 3 months. Referral for surgical intervention in RA of the hip should be made when the patient has failed to respond to maximal non-surgical management and presents with persistent pain, progressive deterioration in function and worsening joint deformity. The aim of surgery is to reduce pain and prevent further deterioration.
Septic arthritis
Septic arthritis of the hip is most common in childhood and rarely seen in adults unless through direct inoculation (e.g. after hip arthroplasty) or in the immunocompromised. It was first described by Smith in 1874, prior to the advent of antibiotics, and had a reported mortality rate of 60%. Potential sequelae of missed diagnosis include chondrolysis, limb deformity (secondary to AVN, pseudoarthrosis, premature physeal closure and/or dislocation), osteoporosis, overgrowth of the greater trochanter and secondary metastatic infection.
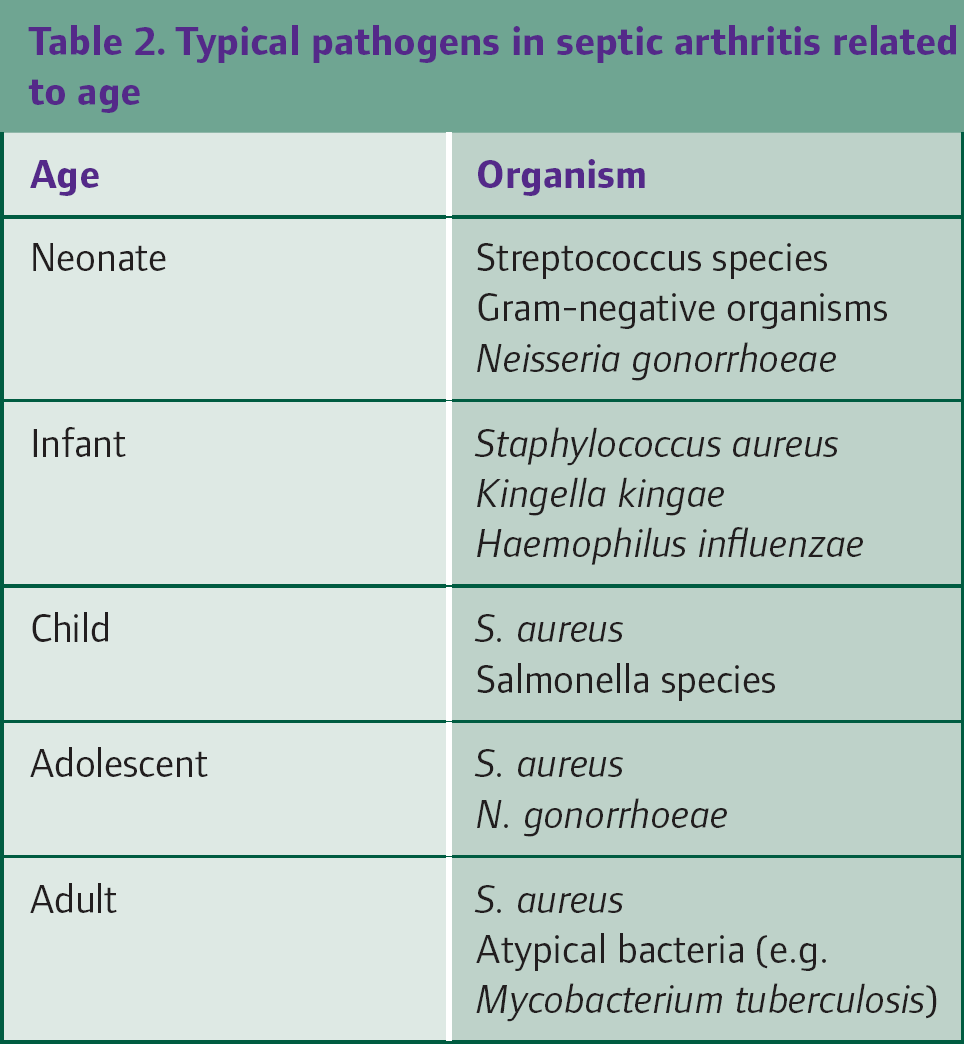
Inoculation of the joint can occur as a result of direct inoculation, haematogenous or adjacent osteomyelitic spread. Causative organisms are listed in Table 2. The most commonly isolated bacterium in septic arthritis is Staphylococcus aureus; however, a causative organism is only isolated in 60% of patients. Historically, Haemophilus influenzae was the most pathognomic organism; however, this has been principally eradicated; thanks to childhood vaccination programmes in the UK.
Typical pathogens in septic arthritis related to age
The patient will tend to present with increasing pain and decreasing range of movement, often with the hip held flexed, abducted and externally rotated to relax the capsule. Following direct inoculation, there may be symptoms of general malaise and lethargy, an acute or more commonly insidious onset of pain, which in the presence of a prosthesis may be related to septic/infective loosening. Clinical signs may include sinus formation and discharge, inflammatory skin changes, reduced range of movement and tenderness.
Septic arthritis is an orthopaedic emergency and necessitates immediate secondary care referral. Imaging in secondary care includes anteroposterior and lateral radiographs, ultrasound scan and MRI. Antibiotics should be withheld until microbiological samples can be taken including blood cultures and joint aspirates with or without synovial samples. Empirical antibiotic treatment is then started according to local guidelines but typically includes intravenous gentamicin and cefotaxime.
Neoplasia and metastasis
Primary neoplasms of the proximal femur have an extensive differential diagnosis beyond the scope of this article. Patients may present with unexplained or persistent bone pain or tenderness, particularly at rest, non-tender bony masses, limp, pathological fractures or systemic symptoms unrelated to the proximal femur. Radiographs may show lytic, blastic or mixed lesions requiring further specialist investigation and management.
Metastasis to the skeleton is common, with the proximal femur second only to the axial spine as a site for bony metastasis. The most common neoplasms to metastasize to the bone include breast, lung, kidney, prostate and thyroid cancers. With the prolonged survival of cancer patients, the incidence of metastatic bone disease is increasing. Patients may be asymptomatic with metastases being an incidental finding or may present with pain, loss of function and/or pathological fracture.
Any patient with a history of cancer or red flags in their history (e.g. change in bowel habit, weight loss, fatigue, cough, hoarseness, dysphagia or chronic pain) should have further investigation. The National Institute for Health and Clinical Excellence (NICE) recommends that this should include immediate radiographs of the hip and pelvis (NICE, 2005) and referral to be seen by an appropriate specialist (usually an oncologist or orthopaedic surgeon) within 2 weeks.
Surgical treatment can be offered for intractable pain, impending or actual fracture, or to improve quality of life. Radiotherapy for pain control may be an alternative for patients without fracture who are too frail for surgery. Metastatic pain from prostate cancer may respond to hormonal therapy.
Referred pain
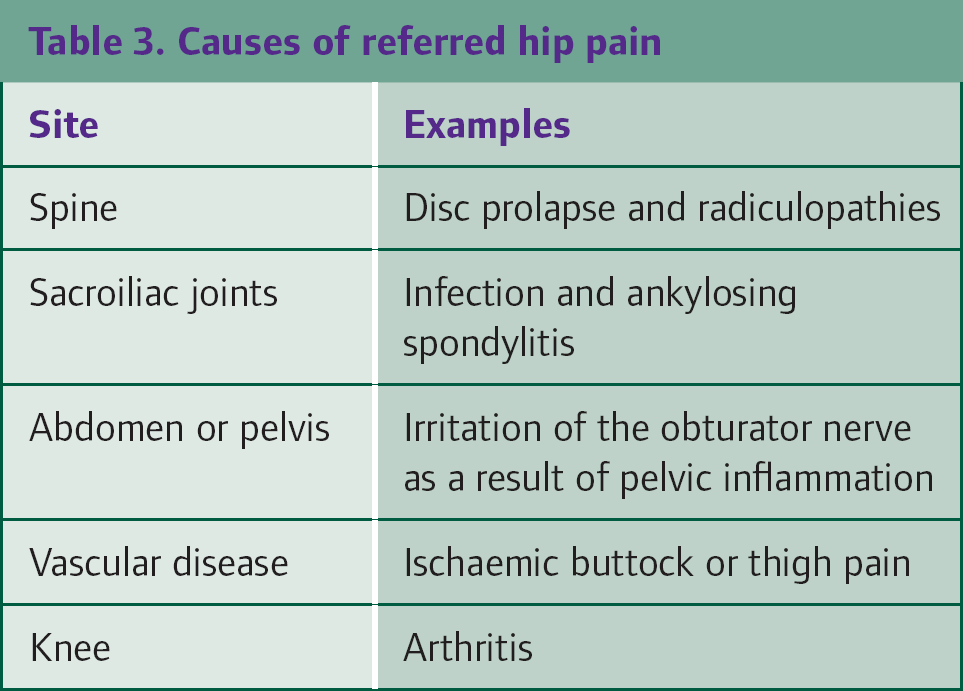
Referred pain is pain felt at a site distant from the cause of the pain. Always remember that patients presenting with hip pain may be experiencing referred pain from elsewhere. Table 3 lists common causes of pain referred to the hip area.
Causes of referred hip pain
Key points
Knowledge of the anatomy of the hip and the anatomy being tested when examining the hip is crucial Most hip pathologies have a clear and differentiating history Septic arthritis is an orthopaedic emergency and requires immediate specialist consultation History of malignancy, or red flags in the history, should prompt immediate investigation