
Abstract
The incidence of hip and knee replacement surgery is increasing rapidly as a consequence of our ageing and increasingly obese society. In the UK, 50 000 hip replacements are being performed each year, and this is expected to treble by 2030. The aim of this article is to discuss the principles behind hip and knee arthroplasty, the types of prostheses, the surgeon's aims and the potential complications that may be encountered.
The GP curriculum and hip and knee arthroplasty
Hip arthroplasty
There are multiple indications for hip arthroplasty. Hip arthroplasty, as other types of arthroplasty, can be categorized as total, replacing all joint components, or partial, when some aspects of the anatomical joint remain.
Total hip arthroplasty
The most common indications for total hip arthroplasty (THR) are pain, deformity and decreased range of movement secondary to osteoarthritis. Other indications include:
Trauma Infection Avascular necrosis Slipped upper femoral epiphysis Failed reconstruction Malignancy Congenital disorders.
The aim of THR is to provide a pain-free joint, which allows patients to perform functions expected of them in their day-to-day living. This demand will change depending on patient age, medical co-morbidity and mental status.
The surgical goal is to replicate the normal anatomical position of the hip joint and provide a stable joint with optimum range of movement by replacing both femoral and acetabular components of the joint. The femoral component replaces the femoral neck and head and aims to be positioned in such a way as to restore the centre of rotation of the femoral head at its most anatomically accurate position to allow optimum movement and ambulation. Failure to optimize the anatomical position will result in a hip that has an abnormal leg length and muscle balance, which is liable to impinge or remain unstable; both of which will restrict movement, increase discomfort, accelerate wear and promote dislocation.
Femoral stems are manufactured from cobalt-chrome or titanium alloys. They are either cemented or non-cemented (Fig. 1). Cemented stems are smooth and rely on a cement made from a polymer (polymethylmethacrylate) that acts as a grout between the femoral medullary canal and the prosthesis. Non-cemented stems have a partial or fully coated surface that allows bone to grow into or onto the surface of the prosthesis. Both have excellent long-term survival (cemented stems 91.5% at 31 years) and, as yet, there is no clear evidence to favour one type over the other. Theory suggests that non-cemented stems may be beneficial in younger patients as bone ingrowth provides a stronger fixation although there is no definitive evidence for this.

Cemented (left) and uncemented (right) femoral components.
Intraoperatively, the acetabulum is reamed using an instrument to remove a periphery of bone to prepare it for the acetabular prosthesis. As with the femoral component position is paramount to outcome. The acetabular prosthesis generally consists of a metal ‘outer’, which is either cemented or non-cemented (Fig. 2). As with the stem, non-cemented cups have excellent survival rates, documented to be up to 96% at 20 years. Choice, as with femoral stems, is often determined by surgeon choice, patient cohort and cost-benefit analysis. Occasionally, screws are required to provide enhanced fixation although the cups have excellent hold provided by both osseous ingrowth and the elastic nature of the bony acetabulum gripping the prosthesis. A hybrid THR refers to one, which incorporates a cemented component (usually femoral) with an uncemented one (usually acetabular) (Fig. 3a).

An example of an uncemented acetabular component with ceramic liner and head.

(a) A cemented femoral stem with non-cemented acetabular component. (b) An example of a right hip resurfacing.
Hip resurfacing
Hip resurfacing involves a surgical approach similar to that for THR. The acetabulum is replaced in a similar manner. However, rather than excision of the femoral head, the surface is reamed to allow fit of a metal ‘resurfacing’ that articulates with the metallic acetabular prosthesis (Fig. 3b). This surgery is aimed at a younger patient group who are more likely to outlive the survival of a traditional prosthesis. The aim is to restore anatomy to as near as normal, thus offering improved load transference through the prosthesis to the femur compared with a THR.
This is a relatively new procedure that demonstrates excellent short-term results having a 5-year prosthesis survival of between 93 and 96%. There appears to be little difference in outcomes comparing resurfacing and THR but the dislocation rate is lower in the former and conversion to THR is technically straightforward as a consequence of preserved bone stock. Fracture of the neck of femur following resurfacing is a risk that increases with age and decreasing bone density, so generally resurfacings are not done in those over 65 years of age.
Bearings
The bearing refers to the articulating surfaces of the prosthetic joint. The most common materials are
highly cross-linked polyethylene metal (cobalt-chrome/titanium) or ceramic.
The most usual combination is a polyethylene acetabular bearing paired with a metal femoral head, ceramic liner and head or metal head and liner. Each material has pros and cons. Ceramic is strong but can be more brittle than other materials, whereas polyethylene is relatively soft in comparison to metal and ceramic. Polyethylene is prone to wear but rates are generally slow being about 0.01–0.02 mm/year. However, because of this, polyethylene has been noted to cause some problems as a consequence of wear, with the debris particles accelerating further wear and prosthesis loosening. As the liner becomes increasingly worn and the head less of a concentric fit, the risks of increasing discomfort and dislocation escalate.
Metal-on-metal bearings release cobalt and chromium ions into the blood stream. Tissue inflammatory reactions occur and are commonly termed ‘pseudotumours’, but there is no evidence that this effect is linked with malignancy. Inflammation and pseudotumours may cause pain and soft tissue destruction. Most cases are noted in patients who have undergone hip resurfacing rather than THR. Incidence of revision surgery as a result of this phenomenon is 1–2% but increased with time and higher in women, especially those under 40 years. It is feasible that the undiagnosed incidence of pseudotumours and associated soft tissue reactions is much higher but, if asymptomatic, there is no cause for concern. The effects of trans-placental passage of metal ions are unknown, but as a precautionary measure, metal-on-metal bearings are avoided in women of child-bearing age should arthroplasty be required.
Complications of hip arthroplasty
Every operation has inherent associated risks. The timing of arthroplasty surgery ideally occurs at the point at which the benefits of undertaking surgery outweigh the potential risks.
Bleeding
Bleeding can occur after hip arthroplasty, occasionally requiring transfusion. British Orthopaedic Association guidelines (BOA, 2005) advise that patients should not be transfused with haemoglobin of greater than 10 g/dl. Haemoglobin of less than 5 g/dl is essential to transfuse and between 8 and 10 g/dl is safe even with coexisting cardiorespiratory disease. There is no evidence for the use of ferrous sulphate to hasten recovery.
Infection
Prior to the use of perioperative prophylactic antibiotics, this rate exceeded 25%, but now the infection rate following hip arthroplasty is less than 1%. Diabetes, immunosuppression and obesity have been identified as independent risk factors for prosthetic infection. After the wound has healed, risk of infection decreases and continues to do so with time.
Infection is usually characterized by pain, present at rest and on movement. Wound changes may be absent, but when present include persistent discharge or tenderness and redness. Systemic symptoms may or may not be present. Unfortunately, C-reactive protein (CRP) and plasma viscosity levels are not specific and can remain elevated for 6 months or longer post-operatively; however, they should not be increasing. Never aspirate any prosthetic joint in primary care, even if infection is suspected.
Contact the operating surgeon if infection is suspected. Deep infection is a real problem. Once present, it is extremely difficult to eradicate. Antibiotic delivery is difficult as is organism eradication from the prosthesis. Treatment may be with prolonged antibiotic administration although far more frequently surgery is required in addition to this. Occasionally, salvage of the prosthesis is possible when accompanied by extensive lavage and debridement, but revision surgery is often necessary.
A Girdlestone procedure is removal of the prosthesis and excision of the proximal femur. It is performed as a salvage procedure to relieve pain or possibly as a consequence of infection. Surprisingly, patients are usually pain free and remain ambulant to a degree following this procedure.
Stitch abscesses are not unusual. They generally resolve with removal of the offending suture with or without a short course of antibiotics.
Venous thrombosis
The deep vein thrombosis (DVT) rate following hip arthroplasty is just under 50% and the pulmonary embolus (PE) rate is 3% if the patient is not treated with prophylactic agents. The DVT rate decreases to 2–5% once treated prophylactically.
Thromboprophylactic therapy consists of post-operative low-molecular weight heparin (LMWH) or other similar anticoagulant therapy, which is now advised to continue for 28–35 days. Therefore, home therapy after discharge is now common. A potential complication of thromboprophylactic therapy is the promotion of bleeding, which in turn may impair wound healing and result in infection or the need for further surgery. The National Institute for Health and Clinical Excellence (NICE, 2010) recommends that the relative risk reduction in thromboembolic events outweighs these risks and is cost-effective; however, many orthopaedic surgeons disagree and this remains a point of contention. Thromboembolic stockings and pneumatic foot pumps are a useful adjunct perioperatively. Incidence of fatal PE is less than 0.01% but thromboprophylaxis has no influence on this.
Soft tissue collections
Early on, haematomas can occur. Generally, these resolve without intervention but they can provide a focus for infection. The surgeon should be informed if concerned. Soft tissue collections, including pseudotumours, may cause pain on specific movement and on palpation and are best diagnosed by magnetic resonance imaging (MRI).
Leg length discrepancy
Following hip arthroplasty, leg length discrepancy can be a problem but surgeons try to avoid this. It is advisable not to aim to alter this with devices such as shoe raises too soon following surgery but to let things settle for a few months. This is one of the things the patient will often mention in follow-up clinics and will be addressed by the orthopaedic team if necessary.
Gait abnormalities can occur after THR for a variety of reasons. These are generally picked up on and managed during follow-up appointments although, should concern arise, a referral to the operating surgeon is appropriate.
Dislocation
The dislocation rate following hip arthroplasty is 2.5–5%. Patients present with a history of sudden onset of pain that may be accompanied by shortening and rotational deformity of the leg. This requires urgent referral to the emergency department. Following dislocation, the re-dislocation rate is about 30%. Certain positions such as hip flexion and crossing of the legs predispose to dislocation, thus patients are given advice regarding avoidance of these manoeuvres. Incidence of dislocation is higher in THR following fractured neck of femur.
Loosening
Loosening is usually characterized by pain on activity, often (but not always) relieved by rest. Loosening can result from surgical technique, expected component wear, fracture, osteolysis (reabsorption of bone material) or infection. It can be detected on serial radiographs and other modalities such as bone scan and MRI. If suspected, referral back to an orthopaedic surgeon is required as wear and loosening are common indications for revision surgery.
Trochanteric bursitis and abductor tendonitis
Trochanteric bursitis and abductor tendinitis are characterized by pain localized to the area of the greater trochanter, often very specifically. There is pain on palpation and on movements that stress the area such as active abduction and straight leg raising. Overlying skin changes are unlikely.
Both conditions can be appropriately managed with injection of steroid and local anaesthetic (e.g. 40 mg depomedrone and 5–10 ml 1% lidocaine), which is safe in the community. Relief may be transient or permanent. If symptoms persist or recur despite injection, referral is appropriate for further imaging, injection or occasionally surgical intervention.
Sciatic nerve injury
Sciatic nerve injury is a rare complication following hip arthroplasty with rates quoted of 1–3%. The prognosis is determined by degree of injury. Physiotherapy and occupational therapy aids may be necessary.
Noise
Patients will often complain of the hip replacement making noises such as squeaks, clunks and clicks. This is more common with ceramic bearings and is reported by up to one in three patients. Generally, noises are harmless, but if persistent or consistently clunking, refer for an orthopaedic opinion in case the noise heralds an unstable fit between components or a subluxing hip threatening to dislocate.
Pain
Pain following hip arthroplasty surgery is common with 5% complaining of persistent pain. The diagnostic challenge arises in determining the origin of symptoms and how to proceed. The causes of pain associated with the prosthesis are legion and are not covered exhaustively above.
It is important to remember referred causes of hip pain. Commonly, symptoms can be felt in the hip arising from lumbar spine pathology. Similarly, vascular insufficiency and claudication can present as hip and thigh pain, as can hernias, soft tissue and bony masses such as neoplastic deposits.
Knee arthroplasty
The surgical aims of knee arthroplasty are to restore mechanical alignment, preserve or restore the joint line and ensure adequate soft tissue balancing thus providing a pain-free stable joint with the maximum range of movement possible. Great care is taken during the operation to ensure precise alignment of the components as failure to do so can lead to uneven wear, loosening of components and early failure, as with hip arthroplasty.
As with the hip, pain and deformity secondary to osteoarthritis are the most common indications for knee arthroplasty surgery. In contrast, in a trauma setting, primary knee replacement is not undertaken but rather an attempt to restore normal joint anatomy through a combination of internal and external fixation is utilized.
Other disorders that may require knee replacement surgery include:
Avascular necrosis Metabolic bone disease Post-infective Post-trauma Malignancy Congenital deformity.
Types of knee replacement
The decision as to what type of knee arthroplasty surgery is most appropriate is based on several factors:
Patient age Bone and soft tissue anatomy Health Patient expectations and Pattern of arthritic wear.
The knee joint can be divided into three compartments, medial, lateral and patello-femoral. These can be affected by osteoarthritis in isolation or together resulting in uni-, bi- or tri-compartmental arthritis.
Arthroscopic knee washout is occasionally of some benefit to delay definitive surgery or in patients in whom arthroplasty is contraindicated, for example, very frail patients for whom the long operation and recovery period would be harmful. However, debridement of arthritic tissues is no longer thought to be of any benefit. Arthroscopy may be used to assess the knee for suitability for unicompartmental arthroplasty prior to operation.
Unicompartmental knee replacement
Unicompartmental knee replacement (UKR) is less common because it is more usual to have widespread degeneration requiring total knee replacement (TKR). However, the medial compartment of the knee is more commonly affected by osteoarthritis than the lateral compartment because of the increased vulnerability of the medial meniscus to injury and therefore alteration of the mechanical forces applied to this part of the knee. The benefits of UKR are that the patient has a smaller incision, shorter hospital stay (about 2–3 days after operation), faster return to unaided walking and the preservation of more normal tissues, namely the cruciate ligaments and other unaffected compartments (Fig. 4a).
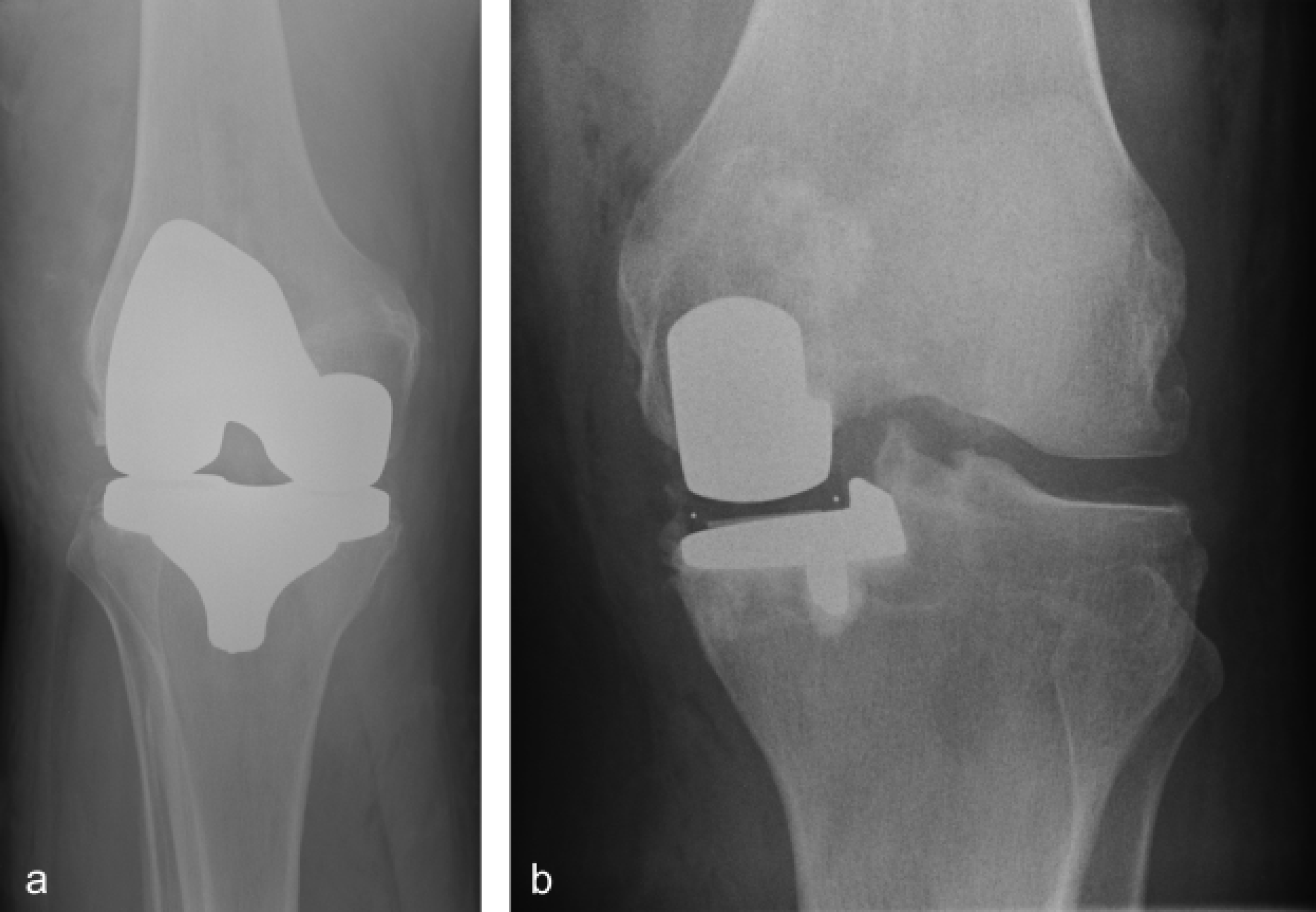
(a) A radiograph illustrating a cemented total knee replacement. (b) A radiograph illustrating a unicondylar knee replacement.
Patello-femoral arthritis in isolation often presents with a description of pain when going upstairs or when standing from a seated position, and commonly an unremitting pain seated at rest, localized behind the kneecap. This can be treated by resurfacing of the patella and underlying femoral trochlea.
Total knee replacement
By far, the most common form of arthroplasty in the knee is a total replacement (TKR). There are usually four components to the prosthesis: femoral and tibial metal-cemented elements; a polyethylene spacer attached to the tibial component and, in the majority of cases, a polyethylene bearing on the patella (Figs. 4b and 5). As with hip arthroplasty, the metal components are generally cobalt-chrome or titanium alloys. The majority of TKR components are cemented although uncemented components also exist. The polyethylene spacer is generally firmly attached to the tibial component. Mobile polyethylene bearings have been designed with a view to reducing wear and prolonging the life of the replacement joint, but the long-term outcome data for these are, as yet, unavailable.

An example of a total knee replacement demonstrating the individual components.
A larger incision is required for TKR compared with UKR. Approximately, 1 in 20 TKRs are undertaken as minimally invasive surgery (MIS), resulting in a scar of about half the length. Image-guided surgery is another technique currently being used, using computer navigation equipment to plot the precise positions of components to ensure optimum alignment. This is not a widely used technique and trials are awaited to assess whether it will improve clinical outcomes and be cost-effective.
The time of life at which knee arthroplasty is recommended is decided on a balance of activity, disease progress and other co-morbidities. As a rule of thumb, a rate of failure of replacements can be expected to be approximately 1% per year; therefore, patients with osteoarthritis, aged 65 years, have an 85% likelihood of outliving their prostheses. The factors that are considered to decrease this likelihood are as follows:
Weight—as much as obesity can cause osteoarthritis it is also a contributing factor towards early wear of polyethylene spacers, mainly if not aligned correctly If the arthroplasty has been undertaken for progressive disease such as ankylosing spondylitis, the continuing progress of disease can alter the biomechanics of the prosthesis and lead to loosening The mechanical strain on components is increased by frequency of use and forces involved. More active patients have greater wear and earlier failure.
Complications of knee arthroplasty
Inherent risks of knee arthroplasty surgery are similar to those of the hip arthroplasty. The assessment of the painful knee or problematic wound post arthroplasty requires the same logic and approach as with the replaced hip.
Bleeding
As with hip surgery, bleeding can be a problem both during and after knee surgery. Many centres will use re-transfusion drains with TKR, thus allowing autologous blood transfusion.
Infection
There is less than 2% risk of deep infection with TKR when perioperative prophylactic antibiotics are used. As with hip arthroplasty, post-operative wound management and assessment of painful or swollen lower limbs are key elements to avoiding complications in the midterm.
Any persistent erythema, increasing pain or discharge from recent knee arthroplasty warrants urgent assessment by the operating surgeon to exclude a deep infection. It is important to remember that the artificial components of joint replacements mean that joint infections do not present with the normal feature of inability to move the joint and that some features, such as pain, erythema and swelling, are part of the normal healing process of an arthroplasty.
Again early action is the key to preventing the failure of the operation. If infection is suspected, contact the operating surgeon and arrange for review as soon as possible and certainly within a week. As with THR, infection is problematic and will require similar management.
Thromboembolus
Historically, risk of DVT associated with TKR was as high as 50%. However, LMWH and other measures such as use of thromboemboloic stockings and pneumatic foot and calf pumps have decreased this incidence to 2–5%. Incidental research has suggested there may be a much higher incidence of subclinical below knee DVT. NICE guidelines (NICE, 2010) advise continuing LMWH for 14 days post-operatively.
Pain
Pain can be an ongoing problem following knee replacement. Roughly, 5% of patients following have ongoing discomfort, for which it is not possible to diagnose a cause. Undiagnosed pain is not a reason for revision as the pain is rarely relieved by this.
Arthrofibrosis
Knee stiffness can be a problem. A possible predictor may be failure to obtain early range of motion prior to discharge home. Referral for manipulation under anaesthetic may be required if symptoms are severe.
Perioperative soft tissue injury
Both the medial collateral ligament and extensor mechanism are at risk during knee arthroplasty. Both can be repaired intraoperatively if damaged although the patient will require an altered rehabilitation regimen post-operatively if this is done.
Late patella fracture may occur mainly as a consequence of altered biomechanics or over-reaming of the patella. This can be treated conservatively or surgically depending on the injury and patient characteristics.
Nerve damage
The main nerve structures at risk at the time of knee arthroplasty are the common peroneal nerve and tibial nerve. Damage results in distal sensory deficit with or without associated motor deficit and a drop foot. Consequences and longevity of symptoms are determined by the extent of the injury.
Blood vessel damage
The popliteal artery and vein lie immediately behind the knee capsule and are consequently at risk during knee arthroplasty. Should they be injured, surgical repair is necessary.
Leg length discrepancy
Leg length discrepancy is unusual following TKR, but can occur. However, more often, this is an apparent phenomenon following deformity correction and the symptom soon settles.
Dislocation
Dislocation of a TKR is very unusual. The polyethylene bearing of a unicompartmental replacement is able to dislocate independently as it is mobile. As this is radiolucent, it will not show up on radiographs. This is very uncommon.
Need for revision
Revision knee arthroplasty is becoming increasingly common as patients are outliving their metalwork. It is an operation that carries a significantly increased risk both intra- and post-operatively. The primary difficulty is the need for further bone removal to allow adequate attachment of the necessarily larger prosthesis. This increases the risk of amputation in the event of failure.
Post-operative management
The normal follow-up process following hip and knee arthroplasty surgery is individual for every surgeon. Usually, it comprises a pre-discharge review during the average 4 day post-operative stay and then a 6 week follow-up. Further follow-up varies according to individual preferences and local policies although it is not unusual for patients to be followed up routinely for many years.
Prior to discharge, a post-operative X-ray is taken to ensure prosthesis position is good and that there are no signs of peri-prosthetic fractures. Physiotherapy ensures adequate mobility and educates the patient about gait rehabilitation and muscle strengthening before the patient goes home (or where there are early discharge schemes, in the days after discharge). For knees, physiotherapy should aim to achieve flexion of at least 90 degrees. Surgical wounds need careful monitoring.
At 6 weeks, the key element is mobility and flexibility. If this is inadequate, a manipulation under anaesthesia (MUA) is sometimes considered. This involves having a general anaesthetic and a forced flexion, to break down any restricting scar tissue. Further appointments monitor any residual problems and aim to ensure early awareness of potential complications.
What can the patient expect?
Following surgery, patients should aim to start walking outside, with aids, after approximately 3 weeks. They should expect that it will take at least 6 weeks until they are able to resume normal activities, such as driving. It is not unusual for patients to continue to require analgesia for this time but an ongoing need after that should trigger consideration of complications or other causes of pain (i.e. concomitant hip arthritis).
Patients should not be too quick to discard walking aids over this period as the consequences of a fall during this time are potentially serious and the use of an aid is unlikely to delay their return to normal function.
There are certain precautions that should be taken, more so in the initial stages, to avoid damage to the prosthesis, for example, avoidance of sitting with crossed legs. Following hip replacement surgery, it is advisable not to sleep on the side of the operation as this may promote dislocation. After knee arthroplasty, it is important that patients do not sleep with a pillow under their knee—this may be more comfortable but it can lead to a fixed-flexion deformity.
Airport metal detectors and arthroplasty
Studies in the past have been inconclusive about whether joint replacement sets off airport alarms; however, over recent years, the sensitivity of walk through metal detectors of the type used at airports has been enhanced as technology and perceived threat has increased. A recent study (Ramirez et al., 2007) has concluded that all THRs tested were detected and 90% of TKRs. Of the metal subtypes, those made of cobalt-chromium were most easily detected as compared with those made of titanium or steel. Previous studies have suggested that hemiarthroplasties (such as those used for hip trauma) are also commonly detected.
The BOA has established an information card known as the Orthocard. This is a card that all those who have orthopaedic metallic implants can apply for from their operating surgeon. The card ascertains the presence of an implant and can be presented at security checks, thus aiding security personnel and alleviating patient anxiety. Further details can be found at www.jointaction.org.uk.
Antibiotic prophylaxis for dental procedures
There is no consistent scientific evidence to prove a link between bacteraemia associated with dental procedures and haematogenous spread of infection to a prosthetic joint. Similarly, it has been demonstrated that the significant risk of adverse side effects of antibiotics, their cost and the risk of encouraging antibiotic-induced resistance far exceeds the potential benefit of routine dental prophylaxis for arthroplasty patients. The BOA advises prophylaxis only if patients are immunocompromised or prior to a lengthy dental procedure.
Key points
Arthroplasty is a common safe procedure with many options to suit patient need If in doubt refer back to surgeon—they will always want to know complications as early as possible Do not blindly treat with antibiotics Never aspirate a prosthetic joint.