
Abstract
Choking results from the acute obstruction of the upper airways by food or other objects. For both the patient and the bystanders it can be an extremely distressing event. Obstructions can partially or completely occlude the airway. Choking most commonly affects young children and the elderly and often occurs in locations devoid of medical facilities, such as restaurants or schools. Emergency medical teams may not arrive in time to save a choking victim's life. Therefore, successful management relies on prompt and effective first aid administered at the scene to expel the object. Collectively, these factors make this an important topic for GPs.
The GP curriculum and choking
Recognize and evaluate acutely ill patients (primary care management) Recognize and manage respiratory symptoms such as wheeze, breathlessness, stridor and choking (knowledge base) Understand the basic principles in initial management and appreciate the response time required in order to optimize the outcome (emergency care) Recognize patients who are likely to need acute care and advise them on prevention, effective management and when and who to call for help (comprehensive approach)
Epidemiology and causal factors
Children
Nearly 25 000 children in the UK are taken to hospital every year after choking. Of these, two-thirds are under 5 years and most of these accidents occur within the home. In 2008, approximately 16 deaths attributed to choking occurred in persons under the age of 15 in England and Wales (Royal Society for the Prevention of Accidents, 2008).
Babies are naturally inquisitive and learn much about their surroundings by placing objects into their mouths. Smaller objects can become lodged in the throat and choking ensues. However, toys account for only a small proportion of choking cases. Non-food-related choking accidents are most often caused by coins in infants aged 3 and under. Almost half of all choking accidents in young children involve food—usually sweets, nuts or fish bones. Narrower airways, the lack of adult teeth and a tendency to overfill their mouths, speak and run around while eating contribute to the increased risk.
Adults
Choking is less common in adults than in children but still causes deaths. In adults, choking most often occurs when food is not chewed properly. Pieces of food may ‘go down the wrong way’ if talking or laughing while eating. The normal protective mechanisms initiated during the process of swallowing may be slowed if the person is under the influence of alcohol or drugs. Other risk factors include advancing age, poorly fitting dental work, strangulation and pathologies such as motor neurone disease, Parkinson's disease and oesophageal dysmotility. Rarely choking can occur nocturnally with epilepsy and obstructive sleep apnoea.
Protection of the airways
Blockages can be partial or complete, the former permitting minimal ventilation around the object and having a greater chance of expulsion. Spasm and oedema of the airways also contribute to the overall obstruction and reduce the likelihood of spontaneous ejection. The ensuing hypoxia following airway obstruction can result in irreversible brain damage or death in 4–6 minutes. Indeed, the chances for survival and complete recovery decrease rapidly with the duration of hypoxia.
Swallowing is a well orchestrated event, the goal of which is to move food into the digestive system and keep it out of the respiratory system. During swallowing, the hyoid and larynx elevate and the epiglottis moves downward to protect the entrance to the airway. In children, the larynx and hyoid cartilage are higher in the neck and closer to the base of the epiglottis, providing added protection of the airway. Concurrently, the aryepiglottic folds and the true and false vocal folds contract, providing additional airway protection (Fig. 1).
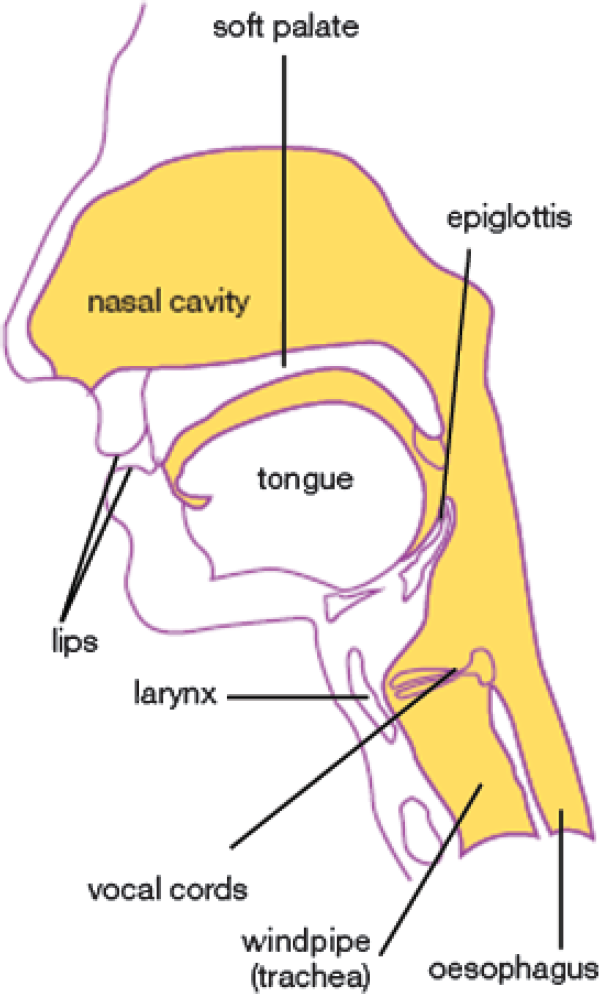
Cross section of mouth and throat. Food and foreign objects may become lodged at level of the pharynx or larynx (above or below the vocal cords). The epiglottis and vocal cords act as protective gates to the airway. Nevertheless, if swallowing is uncoordinated or an object is unintentionally swallowed it may cause choking, impeding airflow to the lungs and thus oxygenation of the organs.
As the trachea divides into bronchi and bronchioles, the dimensions of the air tubes become increasingly smaller. Objects that erroneously enter the airways become stuck as the tubes narrow. The majority of larger objects wedge in the pharynx or the trachea at the level of the vocal cords. Objects wedged above, rather than below, the vocal cords have a better prognosis as they are more amenable to dislodging with therapeutic manoeuvres.
Coughing also helps to protect the airways from particles that have been inhaled. Three phases occur. During inspiration, the larynx opens wide to permit rapid and deep inspiration. Tight closure of the glottis and strong activation of expiratory muscles and expulsion occurs during compression. The larynx then opens widely and a sudden outflow of air results.
Diagnosis of choking
The presentation of choking varies between adults and children as evidence is more subtle in children. If a mild partial blockage has occurred, the subject is ordinarily able to speak, cry, cough or breathe. Stridor, cyanosis, a reduced conscious level and a sudden inability to talk suggest a severe complete obstruction. Children often cry weakly, cough, gag and become stridulous. When an adult is choking, the following behaviours may be observed: coughing or gagging, hand signals to the throat (Heimlich's ‘universal sign’) and panic.
Assessment and basic first aid
The Resuscitation Council (UK) has produced comprehensive guidelines on the management of choking tailored to the severity of the episode and whether the subject choking is an adult (Fig. 2) or a child (Fig. 3).

Algorithm for management of choking in adults.

Algorithm for management of paediatric foreign body airway obstruction.
Choking in adults
If blockage of the airway is only partial, the victim will usually be able to dislodge the foreign body by coughing. If obstruction is complete, urgent intervention is required to prevent asphyxia. Check if the victim is coughing effectively. Signs of an effective cough include:
Fully responsive—the victim is able to speak, cough and breathe In response to the question ‘Are you choking?’, the victim answers and says ‘Yes’
If an effective cough is present, encourage the victim to cough and monitor the patient. Signs of an ineffective cough include:
The victim is unconscious The victim is unable to breathe Attempts at coughing are silent Breathing sounds wheezy or In response to the question ‘Are you choking?’, the victim either responds by nodding or is unable to respond
If the victim has an ineffective cough, call for assistance (for example, send a bystander to call for an emergency ambulance) and assess the patient's conscious level. If the victim is conscious but has absent/ineffective coughing, give up to five back blows (Box 1) as needed. If back blows do not relieve the obstruction, give up to five abdominal thrusts (Box 1) as needed. Do not use abdominal thrusts in pregnant women or people who are obese.
Back blows and chest thrusts for adults
Back blows for adults
Stand to the side and slightly behind the victim Support the chest with one hand and lean the victim well forwards so that when the obstructing object is dislodged, it comes out of the mouth Give up to five sharp blows between the shoulder blades with the heel of the other hand
Abdominal thrusts for adults (Heimlich manoeuvre)
Stand behind the victim and put both arms around the upper part of the abdomen Lean the victim forwards Clench your fist and place it between the umbilicus and bottom end of the sternum Grasp this hand with your other hand and pull sharply inwards and upwards. Repeat up to five times as needed.
Following back blows, or abdominal thrusts, reassess the patient. If the object has not been expelled and the victim is still conscious, continue the sequence of back blows and abdominal thrusts. If the object is expelled successfully, assess the patient's clinical condition (including abdominal examination if abdominal thrusts have been used). If there is any suspicion that part of the object is still in the respiratory tract or there are any intra-abdominal injuries as a result of abdominal thrusts, refer to the emergency department for assessment.
If the victim becomes unconscious, support the victim carefully to the ground and immediately call for ambulance support (if an ambulance has not already been called).
Begin cardiopulmonary resuscitation (CPR) with 30 chest compressions at a rate of 100 compressions per minute, even if a carotid pulse is present.
Choking in children
If the child is breathing spontaneously, encourage the child's own efforts to clear the obstruction. Only intervene if the child's own efforts are ineffective. Assess whether the child is coughing effectively. Signs of an effective cough include:
The child being fully responsive—this is indicated by crying or verbal response to questions Loud cough with the child being able to take a breath before coughing
If the child has an effective cough, encourage the child to cough and monitor him or her. Signs of an ineffective cough include:
The child being unable to vocalize Quiet or silent cough The child being unable to breathe, with or without cyanosis Decreasing level of consciousness
If the child has an ineffective cough, call for ambulance assistance immediately and assess the child's conscious level. If the child is conscious but has absent or ineffective coughing, give up to five back blows as needed (Box 2). If back blows do not relieve the obstruction, give:
Back blows, chest thrusts and abdominal thrusts for children
Back blows for small children/infants
Place the child in a head-downwards prone position (e.g. across your lap). Support the head if needed by holding the jaw. Deliver a smart blow with the heel of one hand to the middle of the back between the shoulder blades. Repeat up to five times as needed.
Back blows for older children
Support the child in a forward-leaning position Deliver a smart blow with the heel of one hand to the middle of the back between the shoulder blades from behind. Repeat up to five times as needed.
Chest thrusts for infants under a year old
Turn the child into a supine position with head down (e.g. by holding the child's occiput and laying the child along your arm, supported on your thigh) Deliver five sharp chest thrusts (like chest compressions but at a slower rate of approximately 20 compressions a minute) to a point one finger's breadth above the xiphisternum
Abdominal thrusts for children over a year old
Stand behind the child (kneel if a small child). Place your arms under the child's arms and encircle his/her torso. Clench your fist and place it between the umbilicus and xiphisternum Grasp your clenched hand with your other hand and pull sharply inwards and upwards. Repeat up to five times as needed.
Note: Ensure that pressure is not applied to the xiphoid process or the lower rib cage as this may cause abdominal trauma.
After the child has been given five back blows and either five chest thrusts (if under a year old) or five abdominal thrusts (if over a year old), reassess the situation. If the object has not been expelled and the victim is still conscious, continue the sequence of back blows and chest (for infant) or abdominal (for children) thrusts. Do not leave the child.
If the object is expelled successfully, assess the child's clinical condition (including abdominal examination if abdominal thrusts have been used). If there is any suspicion that part of the object is still in the respiratory tract or there are any intra-abdominal injuries as a result of abdominal thrusts, refer to the nearest emergency department.
If the child is unconscious, do not leave the child. Place the child on a firm flat surface and call out for help or send for help if it has not already arrived. Open the child's mouth and look for any obvious object causing the airway obstruction. If one is seen, make an attempt to remove it with a single finger sweep. Do not attempt repeated finger sweeps. If this is unsuccessful:
Open the airway and attempt five rescue breaths. Assess the effectiveness of each breath—if a breath does not make the chest rise, reposition the head before making the next attempt. If there is no response to the rescue breaths, proceed immediately to chest compression — regardless of whether the breaths were successful. Follow the paediatric basic life support sequence of 15 chest compressions to every two rescue breaths for 1 minute before summoning help again if it is not already there.
If it appears that the obstruction has been relieved, open and check the airway. Deliver rescue breaths if the child is not breathing. If the child regains consciousness and is breathing effectively, place him in a safe side-lying (recovery) position and monitor breathing and conscious level while awaiting the arrival of the emergency services.
Specialist management of acute airway obstruction
Failure to relieve obstruction by simple first aid manoeuvres may necessitate the insertion of an airway adjunct or an alternate airway to bypass or remove the obstruction. Usually this requires specialist equipment, although there are many recorded cases in which equipment has been improvised using household objects. GPs should consider including simple airway adjuncts in their bags as part of general preparedness for any emergency as long as they have received proper training in their use, which is regularly updated.
Intubation
Insertion of an endotracheal tube may be performed in unconscious or sedated patients to push the obstructing object out of the way enough to ventilate the lungs mechanically. During orotracheal intubation, the airway can also be clearly visualized with the laryngoscope. If the object is visible, it can be removed using Magill's forceps.
Cricothyroidotomy
When attempts to intubate a patient with complete airway obstruction are unsuccessful, a surgical procedure known as a cricothyroidotomy may be required (Fig. 4). This procedure provides a temporary emergency airway bypassing an obstruction at or above the level of the larynx. It is quicker and easier to perform than emergency tracheostomy and associated with fewer complications. The procedure takes about 2 minutes to complete and in emergency situations, where there is no access to medical equipment, cricothyroidotomy has been done using a drinking straw or pen casing and penknife.

Cricothyroidotomy. An incision is made in the cricothyroid membrane bypassing the pharyngeal/laryngeal obstruction and permitting ventilation. Depending on the situation, a wide-bore cannula or endotracheal tube can be inserted through the membrane.
Cricothyroidotomy should be used as a last resort and is best carried out by experienced hands. For safe and effective completion of the procedure, a good working knowledge of laryngeal anatomy is required. The procedure can be performed using a specialist kit, cannula or endotracheal tube.
In all cases the overlying skin is cleaned and local anaesthetic instilled if the patient is conscious. Next, an incision is made in the cricothyroid membrane, a membrane running between the thyroid and cricoid cartilages. This can be identified from surface anatomy. A finger run down the midline from the superior notch of the thyroid cartilage locates the depression signifying the cricothyroid membrane.
In the case of a needle cricothyroidectomy, pierce the membrane at an angle of 45° caudally with a large bore (14G) intravenous (IV) cannula. Aspirate the needle as it is introduced confirming correct positioning by withdrawal of air. Then connect the cannula to an oxygen supply. This technique can usually only be used for 30–45 minutes before carbon dioxide retention becomes significant. Also, expiration is not possible through the cannula so with complete upper airway obstruction, the oxygen flow should be reduced.
Surgical cricothyroidectomy incorporates a larger incision through the membrane through which a small cuffed endotracheal tube or tracheotomy tube (maximum 8 mm) can be installed. The tube should be aimed downwards as it is inserted to avoid damage to the vocal cords. Position can be confirmed with visualization of chest movements and auscultation over lungs and stomach. The tube can then be secured.
Bronchoscopy
Once at hospital, obstructions can be visualized and removed with a bronchoscope. Bronchoscopy entails the insertion of a flexible fibre-optic scope into the trachea that has the potential for the attachment of instruments to remove the object. The patient must be heavily sedated. The procedure can be performed quickly if the person is in distress.
Late complications and recurrent choking
Late complications can occur if the obstructing object was organic. Particles may be aspirated and result in pneumonia. Patients who develop a persistent cough or fever following an episode of choking should be investigated further with a chest X-ray.
Patients who have regular choking episodes require referral to the local ear, nose and throat (ENT) department. Due to the inherent risk of this condition, they require further investigations to ascertain the severity, risk and potentially identify a cause. Speech and language therapy teams can use a flexible nasoendoscope (FNE) to assess a patient's swallow and if they primarily choke at meal times. FNE can diagnose defects in the function of the epiglottis and vocal cords. With the information from such assessments, modifications to a patient's lifestyle can be made such as replacing solid foods for a more pureed diet.
General preventative advice for patients
Prevention is better than cure. Waiting room leaflets or strategically placed posters to educate the public can be life saving. Those targeted should include patients caring for young children and the elderly. Parents should be advised to avoid giving young children hard foods or small objects that are likely to become lodged in their airways. It is recommended that foods such as nuts, seeds, gum, hard candy, peas and tough meats should not be given to any child younger than 4 years of age. Toys should be carefully vetted for small removable parts that a child may be tempted to place into his or her mouth. Small objects such as buttons and batteries should be kept out of a child's reach. Finally, children should be encouraged to remain stationary while eating and chew their food thoroughly before swallowing.
Adults should avoid placing objects such as nails or pins in the mouth for quick access. Advise adults to take small bites of food and chew properly and be aware that alcohol and poorly fitting dentures may impair the ability to swallow, increasing the risk of choking.
Foreign body in the throat
A sensation of a foreign body in the throat usually occurs after eating; a fish bone or food bolus is the most common cause. This can result in severe discomfort, distress and inability to swallow saliva.
If suspected, refer immediately to the local emergency department or ENT department for investigation with lateral neck X-ray and/or laryngoscopy. Most fish bones have passed and the discomfort comes from mucosal trauma. Food boluses often pass spontaneously (especially if the patient is given a smooth muscle relaxant) but occasionally need removal under general anaesthetic.
Key points
Choking is common in young children and the elderly and a cause of deaths in the home Obstructions can be partial or complete Rapid assessment and initiation of first aid are the key factors affecting prognosis Guidelines for the management of choking are available from the Resuscitation Council (UK) and are age specific Where simple first aid measures fail, specialist interventions are necessary to relieve/bypass the obstruction